
Abstract
A man undergoing long-term peritoneal dialysis who had no history of mental illness suffered psychosis and auditory hallucination 2 days after clindamycin was initiated at a single dose of 0.6 g per day for pulmonary infection. His mental symptoms disappeared after clindamycin was discontinued and peritoneal dialysis was strengthened. The patient’s body temperature was mildly elevated the day before he was admitted to the hospital, and no abnormalities were observed on head and chest computed tomography imaging at admission, except for a slow rhythm on electroencephalogram. Many factors were involved in this case; antibiotic-related encephalopathy caused by clindamycin may be one factor. Physicians should carefully consider the use of antibiotics, especially in patients with end-stage renal disease.
Keywords
Introduction
Encephalopathy refers to a group of symptoms that can be caused by heredity, trauma, poisoning, tumor, inflammation, or improper use of antibiotics, resulting in damage to the brain parenchyma and a decline in brain function. Encephalopathy can manifest as memory decline, impaired mobility, and behavior or personality changes.
We report here a case of suspected antibiotic-associated encephalopathy. A middle-aged patient who had undergone long-term peritoneal dialysis for many years suffered encephalopathy in our hospital. In our analysis of causes, we determined that this might be a case of clindamycin-associated encephalopathy.
Case report
On May 3, 2019, a 34-year-old man was admitted to our hospital due to agitation, auditory hallucinations, and abdominal pain for 2 days. Four years prior to admission, the patient had been diagnosed with chronic renal failure and hypertension. Since then, he had undergone stable continuous ambulatory peritoneal dialysis using 2.5% peritoneal dialysis fluid four times per day. The ultrafiltration volume was about 1,000 mL. The patient had a fever 3 days before admission with a peak temperature of 37.8°C, accompanied by dizziness and discomfort in his neck. He took ibuprofen and his temperature returned to normal, but there was no significant improvement in dizziness. A local physician initiated an infusion treatment (clindamycin 0.6 g + normal saline 250 mL, dexamethasone 5 mg, vitamin C 200 mg + normal saline 250 mL), which slightly improved the patient’s dizziness. One day later, the patient reported discomfort in his upper abdomen accompanied by restlessness, auditory hallucinations, and emotional agitation. He continued to receive peritoneal dialysis. The patient visited our hospital accompanied by his family; he was diagnosed with chronic renal failure, hypertension, chronic left cardiac dysfunction, and a symptomatic mental disorder. Signed informed consent was obtained from the patient, and this study was approved by the ethics review committee of the Lianyungang No. 1 People’s Hospital.
The patient had a history of hypertension lasting more than 6 years, with a maximum blood pressure of 200/100 mmHg. He was treated with nifedipine controlled-release tablets, 20 mg twice a day, and metoprolol tartrate tablets, 47.5 mg once a day orally. The patient had also suffered from chronic left ventricular dysfunction for several years. Echocardiogram showed cardiac enlargement, a decrease in ventricular activity and cardiac function, valvular regurgitation of the second and tricuspid valve, and severe pulmonary hypertension (pulmonary artery systolic pressure 97 mmHg; left ventricular ejection fraction 28%). He had no history of medication allergies.
Physical examination showed that the patient had a temperature of 36.4°C, blood pressure of 99/65 mmHg, and heart rate of 55 beats per minute. The patient was restless, agitated, and kept complaining about upper abdomen discomfort. He could not respond to questions when asked about his medical history. A few abnormal breath sounds (moist rales) were revealed when listening to the chest with a stethoscope (auscultation). The patient’s peritoneal dialysis catheter was stable and fixed in place. No edema in the lower limbs was noted. Laboratory examination revealed the following results: leukocyte count of 12.98 × 109/L, neutrophil ratio of 84.8%, lymphocyte percentage of 7.2%, hemoglobin level of 137 g/L, platelet count of 344 × 109/L, blood creatinine level of 1,687.8 µmol/L, blood urea nitrogen level of 33.64 mmol/L, potassium level of 3.23 mmol/L, chlorine level of 89.7 mmol/L, calcium level of 1.85 mmol/L, phosphorus level of 3.87 mmol/L, and sodium level of 137.4 mmol/L. There was no obvious abnormality observed on head and chest computed tomography (CT). Electroencephalogram on day 2 of hospitalization showed moderately abnormal brain topography and basic rhythm (Figure 1). Blood ammonia and blood glucose were normal.
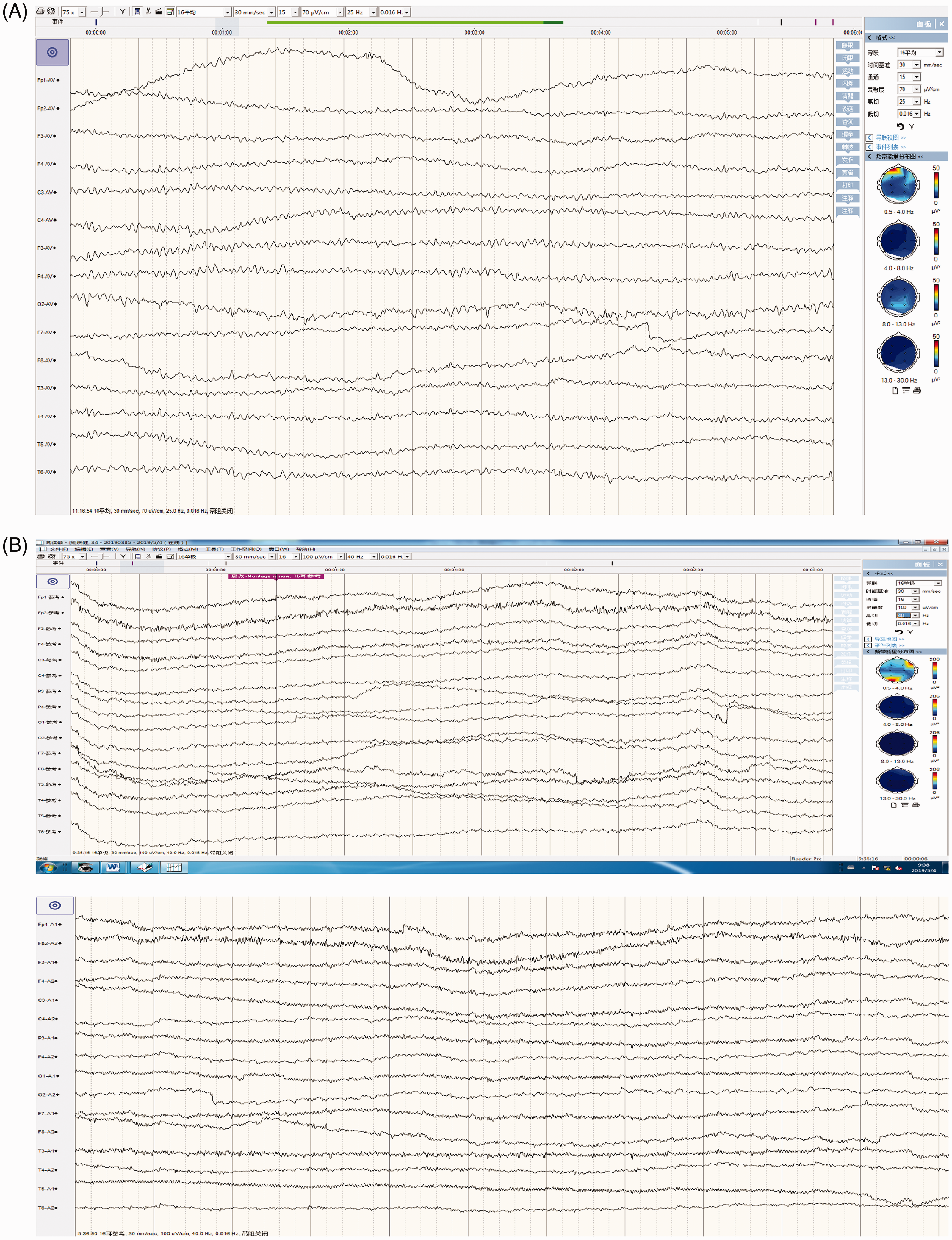
(A) Electroencephalogram on day 2: large amount of low-amplitude fast wave activity superposition, 6- to 7-Hz low and medium θ wave activity are visible. (B) Electroencephalogram after discharge: roughly symmetrical on both sides, 9- to 10-Hz, 10- to 60-µV natural rhythm can be seen, with good waveform and good amplitude modulation, mixed with a small amount of 14- to 24-Hz, 5- to 20-µV wave activity. A small amount of 6- to 7-Hz, 10- to 50-µV rhythm was observed in each region.
At admission, the clindamycin treatment was discontinued, and peritoneal dialysis was strengthened. The patient was treated with low-calcium peritoneal dialysis solution (lactate-G2.5%) 2,000 mL intraperitoneal injection, five times a day; reducing glutathione 1,200 mL intravenous injection, once a day; calcium gluconate 1 g + 5% glucose intravenous injection 20 mL, once a day; 250 mL of sodium bicarbonate intravenous injection, once a day; alprostadil 10 µg + saline 100 mL intravenous injection, once a day; and other support treatments. No antibiotics were administered during the hospitalization. On the night of 3 May, the patient’s anxiety and excitement increased. He began throwing and damaging his personal belongings. The doctor on duty administered diazepam 5 mg static push, olanzapine 2.5 mg orally, and haloperidol 5 mg intramuscular injection assisted sedation. On 4 May, the patient’s abdominal pain eased and irritability gradually diminished. The patient was able to remember information and control his emotions. On 8 May, he was discharged from the hospital without any neurological deficits.
Discussion
Case analysis
The patient had the following characteristics: chronic cardiac and renal failure; long-term use of metoprolol and nifedipine; pneumonia; use of hormones; and history of antibiotic abuse, all of which were preconditions for the occurrence of this case. Encephalopathy can occur in many conditions, including electrolyte abnormality, blood ammonia accumulation caused by hepatic encephalopathy, drug abuse, pneumonia, central nervous system infection, cerebrovascular accident, or antibiotic encephalopathy. According to the results of blood ammonia and electrolyte analysis, an electrolyte abnormality and hepatic encephalopathy could be preliminarily excluded. The patient quickly recovered and refused further examination for economic reasons. Pneumonia, central nervous system infection, and antibiotic encephalopathy could not be ruled out because we were unable to conduct a lumbar puncture and magnetic resonance imaging examination. However, following withdrawal of antibiotics, the patient quickly recovered to a stable neurological state. The CT examination of the head and chest during admission revealed no abnormalities. Psychiatric symptoms caused by pneumonia and central nervous system infection were less likely. The patient had no reported history of illegal or excessive use of drugs. A keyword search of PubMed using “encephalopathy,” “clindamycin,” “encephalopathy, dexamethasone,” and “encephalopathy, vitamin C” revealed a few supporting cases. Based on the similar mechanisms of action of lincomycin (such as clindamycin) and macrolides (both act on the 50S subunit of the bacterial ribosome), we suspected a form of macrolide-associated encephalopathy, as supported by previous cases. 1 We propose that clindamycin-associated encephalopathy might occur in patients with renal insufficiency. Our patient presented obvious central nervous symptoms after taking clindamycin, which may be explained by the following factors. (1) The patient had chronic renal failure, and prolongation of the drug’s half-life resulted in an increase of the drug’s concentration in serum and accumulation in the body. (2) Patients with chronic renal failure have reduced plasma binding protein, decreased protein glycosylation and carbamylation, and thus an impaired blood–brain barrier. Parts of the clindamycin molecule in free form can permeate the blood–brain barrier. (3) The patient has a history of chronic left heart insufficiency and hypertension, which may have resulted in abnormal cerebral blood perfusion, increasing the possibility of cerebral hypoxia and acidosis.
Antibiotic-related encephalopathy
Uniform diagnostic criteria are not available for antibiotic-associated encephalopathy. According to mainstream diagnosis, antibiotic-related encephalopathy can be diagnosed based on the following features and exclusions: (1) a clear history of antibiotic use; (2) a series of neurologic symptoms such as dizziness and restlessness following administration of antimicrobial agents; (3) except for metronidazole-associated encephalopathy, which can show clear abnormal changes on skull MRI, other types may not have clear changes in blood biochemistry or imaging; (4) organic disease, severe electrolyte disorder, abnormal blood sugar metabolic disease, dialysis imbalance syndrome, and neural problems caused by other drugs should be eliminated; (5) neurologic symptoms disappear after withdrawal of antibiotics.
Mechanisms of clindamycin-related encephalopathy
In recent years, there have been many reports on antibiotic-related encephalopathy among patients with renal insufficiency caused by cephalosporins and quinolones, yet lincosamide-related encephalopathy is rare.2,3 According to Bhattacharyya et al., antibiotic-related encephalopathy can be classified into three types based on clinical features. Type 1 is mainly caused by penicillin and cephalosporins (most commonly in those with renal insufficiency) and is characterized by myoclonic seizure. Type 2 is mainly caused by procaine penicillin and sulfonamides and is marked by psychosis. Type 3 is mainly caused by metronidazole and is associated with cerebellar signs. Different drugs are involved in different mechanisms. 4 Currently, the mechanism underlying type 1 is relatively clear and involves induction of chloride ion internal flow, production of inhibitory postsynaptic potential, and interference with the gamma-aminobutyric acid (GABA) signaling pathway and improved action potential threshold. There is no clear hypothesis for the mechanisms underlying types 2 and 3. Our case may belong to type 2, where psycho-sensitive psychosis is predominant. Some researchers speculate that in this type, the metabolism of cortisol and prostaglandins is altered such that antibiotics interact with glutamine and GABA. 5
Mechanism of clindamycin action
Clindamycin is a substituted derivative of lincomycin 7-hydroxyl group, which belongs to the lincosamides. It has an antibacterial effect at low concentrations and a bactericidal effect at high concentrations. It is used clinically for infections caused by Gram-positive and anaerobic bacteria. Clindamycin products can be in the form of hydrochloride, phosphate, palmitate, or capsule. By acting on the 50S subunit of the bacterial ribosome, clindamycin affects the initiation of peptide chain synthesis, suspending bacterial protein synthesis. 6 Clindamycin is mainly metabolized by the liver, with a half-life of 2.4 hours in patients with normal renal function and 6 hours in those with abnormal renal function. 7 Clindamycin can reach an effective blood concentration in most parts of the body, such as blood, bone, and liver. Urine and blood may have antibacterial properties; thus, it has a wide range of clinical applications. However, the drug cannot cross the blood–brain barrier (unless the barrier is damaged, such as in meningitis), so it is rarely used to treat infections of the central nervous system.
Preventive measures and treatment
During disease progression, it is more likely for patients with chronic renal failure to have encephalopathy, which can be caused by cerebrovascular accident, uremia encephalopathy, dialysis imbalance syndrome, and other risks; it is difficult to distinguish antibiotic-associated encephalopathy from these other causes. For patients such as ours, antibiotic-associated encephalopathy is a point to note. To fully understand the diagnosis and treatment of antibiotic-associated encephalopathy, clinicians must understand the indications and pharmacokinetics of various antimicrobial agents; select appropriate drugs based on glomerular filtration rate, liver function, mental state, and personal differences; and carefully monitor the blood concentration of antimicrobial drugs. For patients with severe antibiotic encephalopathy, there are no specific therapeutic drugs at present. In addition to symptomatic support, the first treatment is to stop or adjust the dosage of the suspected drugs, apply diuretics, and strengthen dialysis or other forms of blood exchange. However, peritoneal dialysis was unable to effectively clear clindamycin in this case. The patient recovered rapidly after discontinuation of the suspected medication, most likely because of natural metabolism.8,9 Further research is needed into the mechanisms underlying development of encephalopathy in patients with chronic renal failure.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was funded by the 13th Five-Year Project of Strengthening Health through Science and Education for the key medical talents and founded by the 521 High level Talent Training Project for the key talents of the 5th batch in Lianyungang.