
Abstract
Objective:
The implementation of sonography has revolutionized anesthesia, especially local anesthesia. High-resolution sonography as an essential, well-established, and versatile technique now makes it possible to perform targeted nerve blocks and therefore to anesthetize with increasing precision. Ultrasonographic (US)-guided nerve blocks on cadavers are often used as pilot studies to investigate new techniques. The aim of this review was to map out US-guided pericapsular nerve group (PENG) block in human cadavers.
Materials and Methods:
A systematic scoping review following PRISMA-ScR guideline. A systematic literature review has been carried out, with relevant studies discovered in the following databases: MEDLINE, EMBASE, CENTRAL, BIOSIS Previews, and Web of Science Core Collection. The publishing year was not subject to any extra limitations. Only sonography studies on human cadavers were included. The article was included if the PENG block was the subject of the study.
Results:
The search found 9821 matches, from which 291 investigated nerves. Four studies investigated the PENG block. A total volume of 2396 ml dye was injected with an average volume of 19.01 ml for each PENG block. 126 US-guided PENG blocks were performed on human cadavers.
Conclusion:
Based on our assessment, this study is the first review to screen US-guided PENG blocks on human cadavers. US-guided labeling techniques in human cadavers are a widespread tool to examine new nerve block techniques through staining targeted nerves by dye and investigating staining quality and quantity by dissecting. These results suggest that PENG block should be further investigated on cadavers to determine the MEV90 for the targeted nerves of the PENG block and to test possible novel injection pathways of these nerves.
A common approach to investigated novel ultrasonographic (US)-guided injections techniques on peripheral nerves is to inject colored dye into human cadavers and evaluate staining quality and quantity via dissection.1 –3 The stepwise procedure from pre-investigations of US-guided nerve blocks on human cadaver nerves to the implementation of them in patients’ anesthesia is widespread4,5 and can lead to better anesthesia. 6
Testing new US-guided nerve blocks on cadavers provides an excellent opportunity but should be approached with caution. Often, cadaver sample sizes in studies are small, sometimes as low as n = 1. 7 Quality criteria should be upheld even in cadaver studies, especially in the reporting of sonographic methodology. 8 Furthermore, before transitioning to the next phase of testing a new injection technique on patients, it is recommended to establish a solid data foundation on cadavers.
As a recent study data show, the pericapsular nerve group (PENG) block is still under investigation, and the amount of local anesthetic truly required to ensure sufficient anesthesia varies. 9
Therefore, the aim of this review was to describe the PENG block technique and provide an outline of the existing ultrasonographic observations on PENG blocks in human cadavers. The specific objectives of this scoping review were to conduct a systematic search of the published and gray literature for US-guided PENG block on human cadavers to describe the cadaveric data foundation underlying the PENG block.
The PENG Block
The PENG block, first described by Girón-Arango et al, 10 is a regional anesthesia technique that targets the nerves supplying the anterior aspect of the hip joint, specifically the articular branches of the femoral nerve (FN), obturator nerve (ON), and accessory obturator nerve (AON). The PENG block is effective in reducing postoperative pain following hip surgery, thereby decreasing the need for opioid analgesics. 11 It is particularly advantageous for patients undergoing hip fracture repair, joint replacement, or arthroscopic labral repair, as it provides optimal analgesia. This is especially beneficial for older patients recovering from hip fracture surgery, where pain relief without motor dysfunction or inhibition can significantly enhance postoperative recovery. 12
The studies included in this review reported an injection volume ranging from 20 to 30 ml. The innervation of the hip joint is complex, involving multiple articular branches. The anterior hip capsule is primarily innervated by the articular branches of the FN, ON, and AON, while the posterior capsule receives innervation from branches of the sacral plexus. Research by Short et al 13 indicated that the FN and AON play a particularly significant role in hip innervation. Nociceptive fibers are predominantly concentrated in the anteromedial and superolateral aspects of the capsule, whereas the posterior hip innervation, mainly provided by the sciatic nerve, is associated with mechanoreceptors that mediate proprioceptive information.
The articular branches of the FN and AON are located between the anterior inferior iliac spine (AIIS) and the iliopubic eminence (IPE) (See Figure 1). Although these nerves are often too small to be visualized using ultrasonography, the anatomical plane in which they are situated can be readily identified during an US-guided PENG block procedure. If necessary, the articular branches of the ON can be blocked separately at the inferior aspect of the inferomedial acetabulum. However, typically, a pericapsular spread of the anesthetic volume between the AIIS and IPE is sufficient to achieve analgesia of the anterior hip capsule. The recommended injection volume for this block is 20 ml. 10
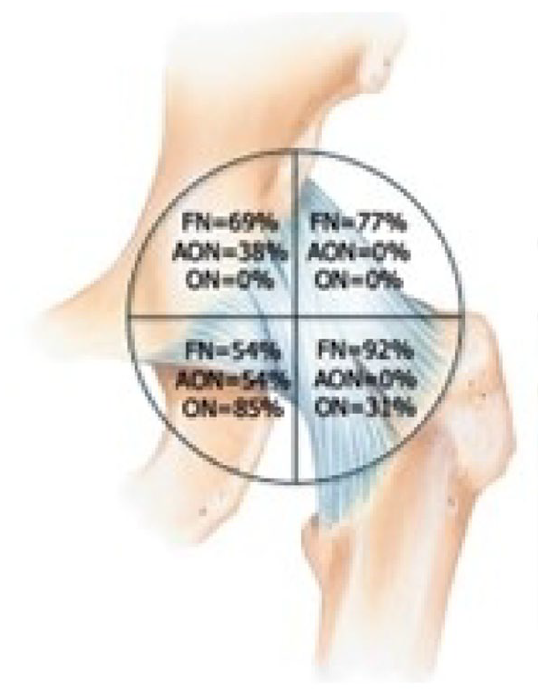
The nerve supply of the anterior hip capsule. AON, accessory obturator nerve; FN, femoral nerve; ON, obturator nerve.
The Technique
The PENG block is performed with the patient in the supine position. The procedure is started by placing the ultrasound transducer over the anterior superior iliac spine (ASIS) in a transverse plane and moving the transducer slowly inferiorly to visualize the bony AIIS. Once the AIIS comes into view, the transducer is pivoted toward the pubic symphysis until the IPE becomes visible. To ensure the optimal positioning of the transducer over the two landmarks (AIIS and IPE), the depth of the AIIS is kept constant during the probe pivoting to get an optimal view (See Figure 2). In slimmer patients, a linear transducer with the extended field of view mode can be used but in most of the patients a curvilinear transducer is the optimal choice. Recommended ultrasound frequencies are between 7.5 and 12 MHz, depending on the habitus. The procedure can be done as an in-plane or as an out-of-plane technique.
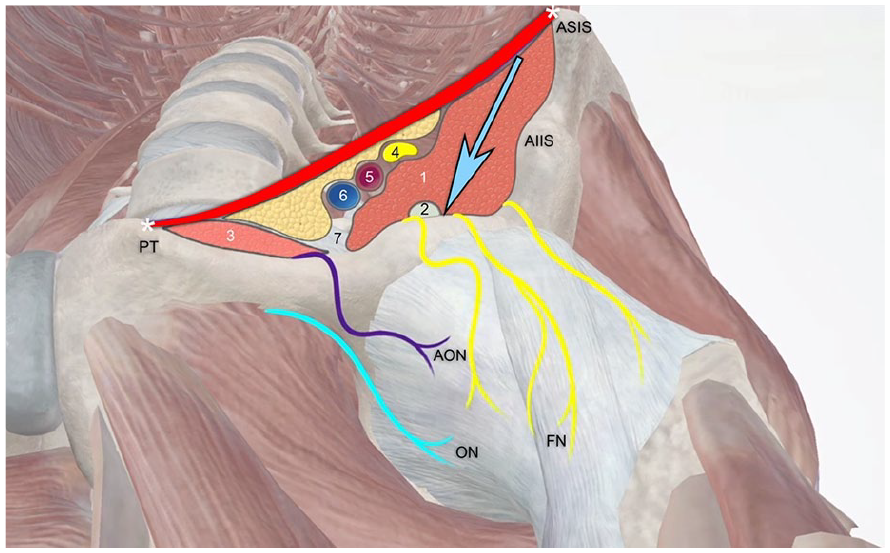
The nerve supply of the anterior hip capsule and the external and internal landmarks for the ultrasound-guided PENG block. 1, iliacus muscle; 2, psoas tendon; 3, pectineus muscle; 4, femoral nerve; 5, femoral artery; 6, femoral vein; 7, iliopubic eminence; AIIS, anterior inferior iliac spine; AON, accessory obturator nerve; ASIS, anterior superior iliac spine; FN, femoral nerve; ON, obturator nerve; PT, pubic tubercle.
The In-Plane Technique
The ultrasound transducer is positioned transversely over the AIIS and moved inferiorly to visualize the pubic ramus. In this plane, the femoral artery and the IPE are identified, and then, using an in-plane technique, a 100-mm nerve block needle is advanced from lateral to medial through the skin at a 30° to 45° angle toward the superior pubic ramus and lateral to the tendon of the psoas muscle. After the tip of the needle comes into contact with the superior pubic ramus, 20 ml of local anesthetic is deposited between the psoas tendon anteriorly and pubic ramus posteriorly. 14 This volume of the local anesthetic elevates the psoas tendon away from the superior pubic ramus (See Figures 3 and 4).
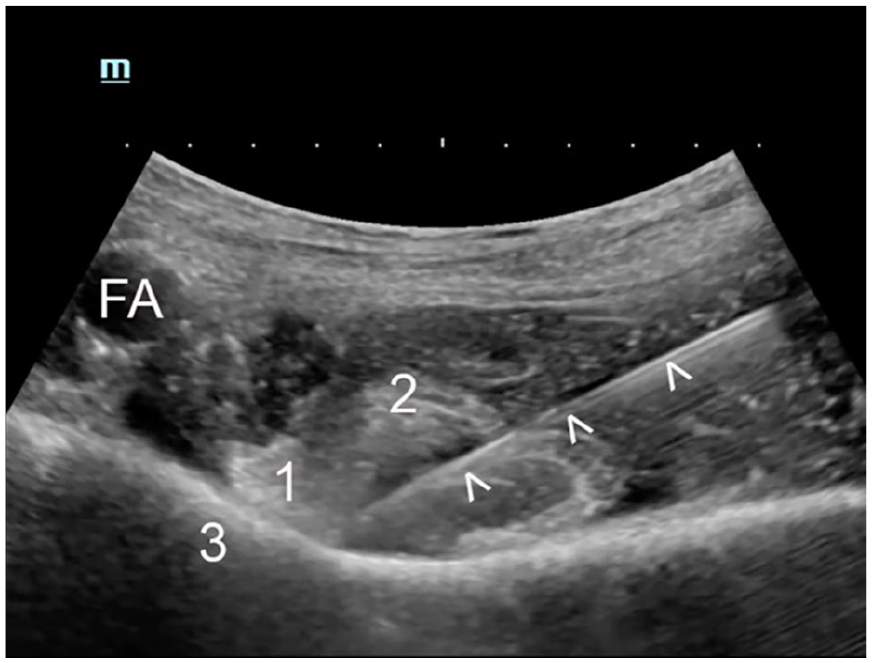
The position of the needle (arrow heads) lateral from the psoas tendon (1) and in contact with the superior pubic ramus. 3, iliopubic eminence; FA, femoral artery; 2, iliacus muscle.
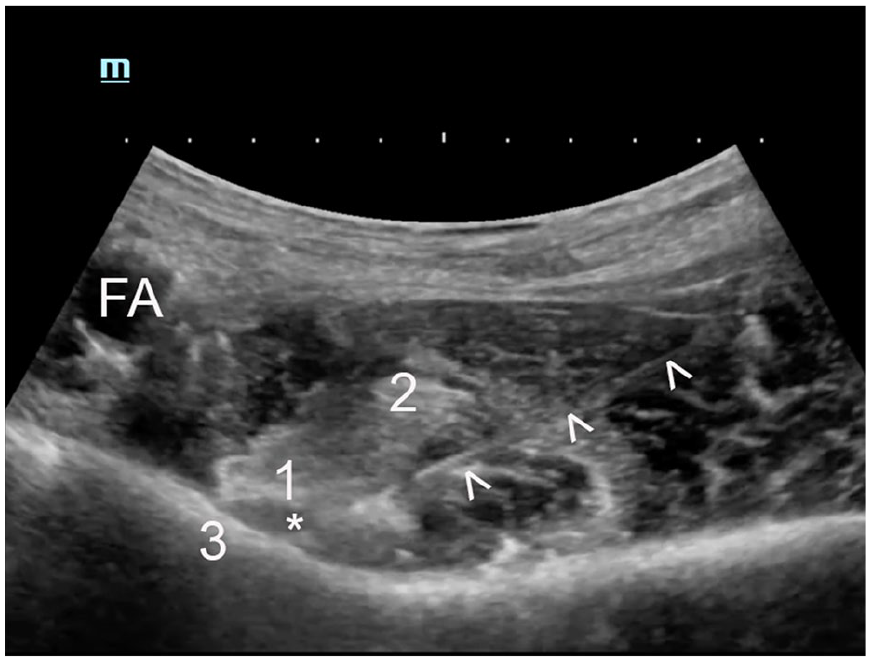
This sonogram shows the initial deposit of local anesthetic (*) between the psoas tendon (1) and the superior pubic ramus. 3, iliopubic eminence; FA, femoral artery; 2, iliacus muscle.
The Out-Of-Plane Technique
At the level of the ASIS, the ultrasound transducer is placed parallel to the inguinal fold, and scanning is performed with a slow movement of the probe. When the lower AIIS is identified, the transducer is rotated slightly median until the hyperechoic shadow of the superior pubic ramus is visible. This maneuver allows the identification of the psoas tendon, as a hyperechoic structure above the pubic ramus. The target is in the plane between these two structures. The pubic ramus should be in the center of the image just medial to the AIIS. Using a 100-mm hyperechoic nerve block needle, the local anesthetic is deposited between the psoas tendon anteriorly and the pubic ramus. 15
Materials and Methods
This scoping review was based on a search on the use of sonography on human cadavers and was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. 16 Accordingly, a protocol for the review was registered on OSF Registries (osf.io/mx468) on November 28, 2022.
The search process is precisely described by Margenfeld et al. 8 The initial search process from 3rd of January 2023 was updated by a second search performed on the June 20, 2024. The research strategy is attached below and was developed with a librarian. To improve the database’s usability, all citations were organized by the anatomical structures covered in each study. A list of 12 main categories and 241 subcategories was created by a reviewer to sort each study into corresponding folders (See Supplementary Appendix Table 3). For this scoping review, the main category “nerve” was reviewed by two independent reviewers to identify PENG block studies. Any disagreements were resolved with the assistance of a third reviewer at each review stage.
Results
Search and Selection of Included Studies
The search yielded a total of 9821 results, of which 291 met the predefined eligibility criteria. All eligibility decisions were made unanimously by the authors after discussion, with no need for third-party adjudication. Both forward and backward citation tracking of the 291 included studies did not identify any additional relevant publications. The PRISMA flow diagram is shown in Figure 5.
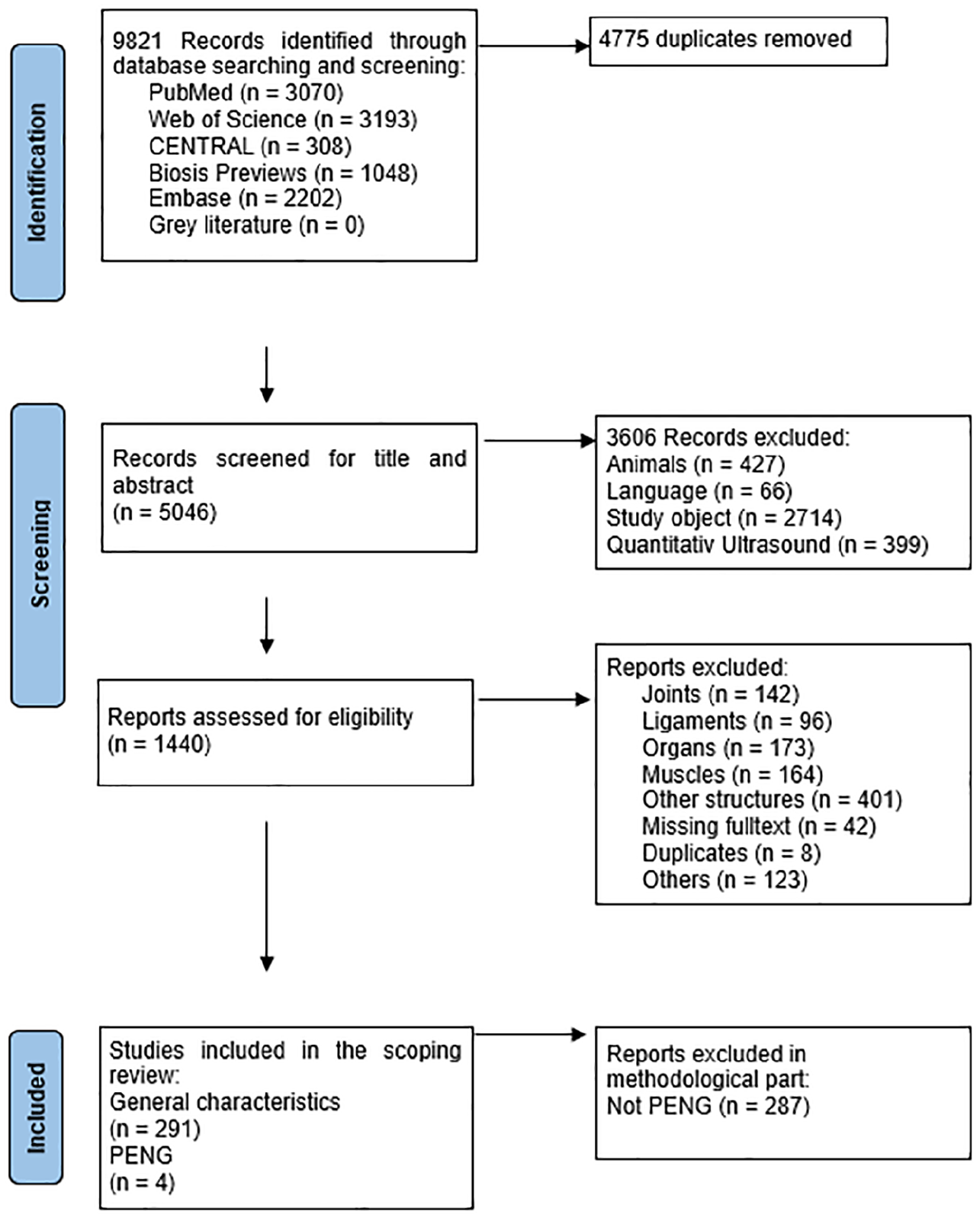
The PRISMA flowchart that provides the breakdown of articles reviewed and retained.
General Characteristics of Included Studies
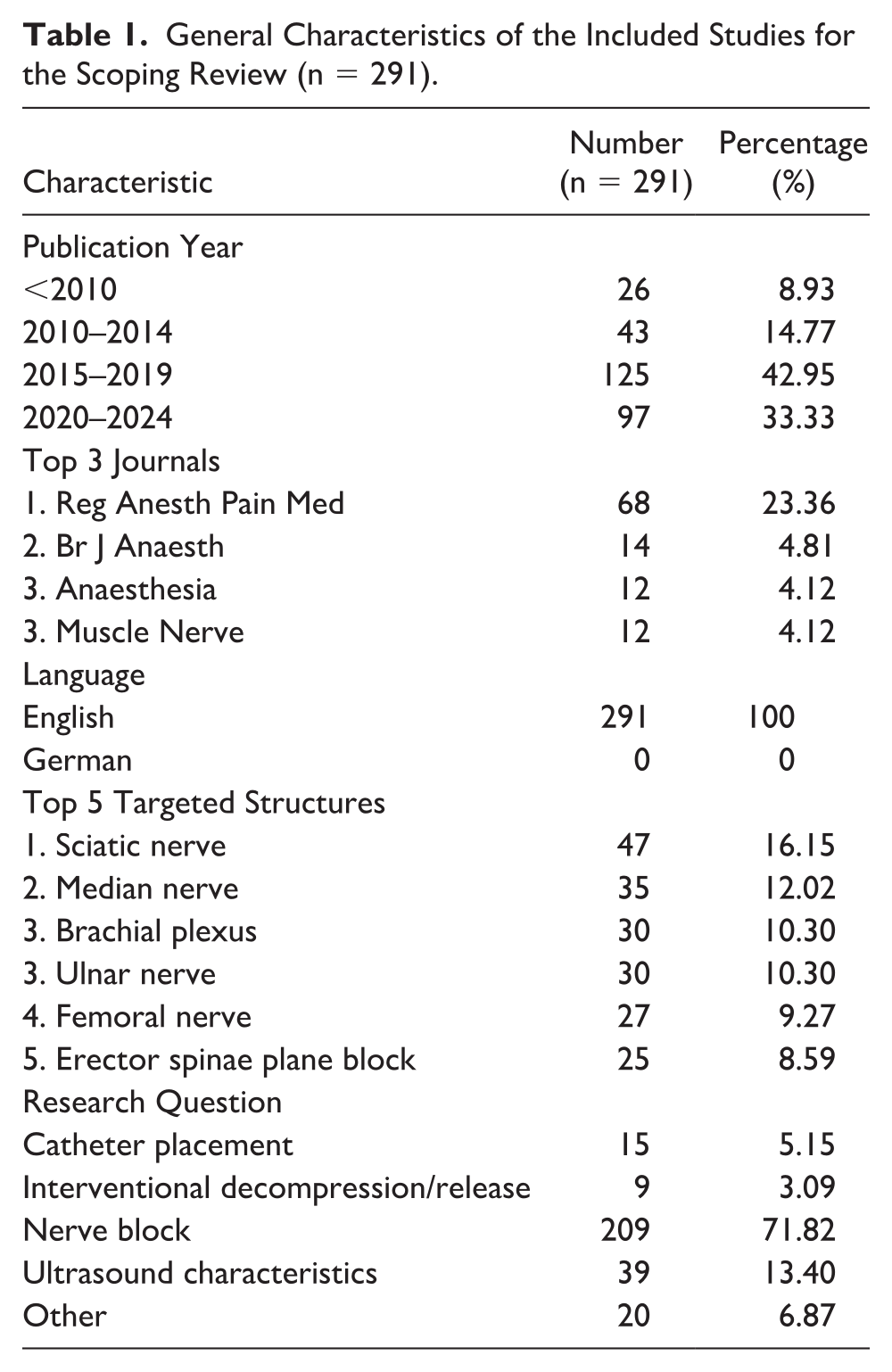
The general characteristics of the 291 studies which were sorted in the main category “nerve” (See Supplementary Appendix Table 3) are presented in Table 1.
General Characteristics of the Included Studies for the Scoping Review (n = 291).
Characteristics of the Ultrasound-Guided PENG
In the methodological analysis, four studies were included. The characteristics of the included studies is summarized in Supplementary Table 2 of Appendix.
The study by Diwan et al 17 was conducted on eight soft-embalmed cadavers. Colored dye was injected by an experienced practitioner in US-guided nerve blocks. Dissection was performed by an anatomist who was blinded to the blocks administered. A total of 16 PENG blocks, each with 20 ml of green dye, were carried out. In addition, a suprainguinal fascial iliac block with 30 ml of methylene blue was performed on the left side. The ultrasound procedure was clearly described using anatomical landmarks. The needle was positioned laterally to medially toward the psoas tendon, with attention given to observe if the psoas tendon was elevated by the injection. The subsequent dissection process was thoroughly detailed. In all 16 PENG blocks, the dorsal portion of the iliac fascia was stained. The nerve marking rates for nerves innervating the hip capsule were as follows: anterior division of the femoral nerve (10/16), anterior division of the obturator nerve (7/16), accessory obturator nerve (6/16), posterior division of the femoral nerve (10/16), and posterior division of the obturator nerve (0/16).
Also, Hamra et al 18 conducted a PENG block with 20 ml of methylene blue on 20 not formalin-preserved cadavers. An US-guided PENG block was performed on 20 hips, while the other 20 hips received the block without US guidance. Both approaches achieved a 95% success rate, as verified by subsequent dissection. A detailed description of the stained nerves was not provided. A detailed description of the investigators and whether the dissectors were blinded was lacking.
Leurcharusmee et al 19 estimated the MEV90 for femoral-sparing PENG block to be 13.2 ml (95% CI [12.0, 20.0]). The success rates for the different volumes were 8/9 for 22 ml, 13/16 for 20/ml, 9/11 for 18 ml, 3/4 for 16 ml, 3/4 for 14 ml, and 10/10 for 12 ml. A PENG block was counted as successful when the femoral nerve was not stained before removing the iliopsoas muscle. The staining of other nerves was not regarded. The investigation was conducted on 32 fresh cadaveric hemipelvis specimens. The qualifications of the practitioner performing the nerve blocks were not provided; however, the dissections were conducted by two to three anatomists.
A precise description and differentiation of the stained nerves, articular branches and fascia was also mentioned in the study by Kim et al 20 They investigated three different injection volumes: 10, 20, and 30 ml, using 18 fresh frozen cadavers. The allocation of cadavers to the injections was randomized. The distribution of the injectate was first assessed using contrast-enhanced computed tomography (CT) and subsequently verified through dissection. The injections were performed under US guidance by an experienced anesthesiologist using a linear ultrasound transducer (6-13 MHz, HS50; Samsung) and a 22-gauge, 80-mm needle. The CT evaluation was conducted by a professor of anatomy with radiological expertise, who was blinded to the injected volume (10, 20, or 30 ml). The dissection was performed by two additional unspecified examiners, who were uninformed regarding both the volumes used and the radiological evaluation. The statistical analysis revealed a significant linear-by-linear association (increased volume leads to increased staining of nerves) for the femoral nerve, the obturator nerve, the lateral femoral cutaneous nerve, and the low articular branch of the femoral nerve.
In total, 126 PENG blocks were performed. A total volume of 2296 ml was injected leading to an average injected volume of 19.01 ml with injections of volumes between 12 and 22 ml. The injection and dissection procedures were clearly explained and reproducible across all studies.
Discussion
This literature review presents the first systematic scoping review addressing US examinations of PENG block on body donors.
The publication years of the identified studies sorted in the main category “nerve” affirmed the rapid growth of this field. The large conduction pathways such as the brachial plexus and the sciatic nerve represented the most frequently examined structures. Also, under the heading of “multiple nerves,” the brachial plexus and three of the four major arm nerves (radial, ulnar and median nerve) accounted for most injection techniques studied on and around nerves. This trend may be attributed to the increasing recommendation of regional anesthesia 21 particularly for surgery such as joint replacements, which remain among the most common surgical interventions worldwide.
With only four cadaver studies, the US-guided PENG block is still relatively understudied compared with the overall data. The data suggest that a lower volume administration is equally effective and should be preferred due to the desired motor-sparing PENG block. A MEV 90 for femoral-sparing PENG block of 13.2 ml was suggested by Leurcharusmee et al. 19 Also, the statistical analysis by Kim et al 20 revealed a significant linear-by-linear association (increased volume leads to increased staining of nerves) for the femoral and the lateral femoral cutaneous nerve. It should be noted that higher volume injections maybe lead to better analgesic effects and thereby reduce postoperative opioid requirements because of the risk of blocking additional nerves, particularly the lateral femoral cutaneous nerve, which innervates the structures commonly encountered during lateral surgical approach for hip surgery. But the lateral femoral cutaneous should be blocked separately. 22 Studies indicate that only a few milliliters of local anesthetic are sufficient to block peripheral nerves. 23 Further studies should investigate whether even smaller volumes are adequate to achieve the desired effect of the PENG block. In this case the question also arises whether it might be feasible to alternatively block the articular branches of the hip joint individually, especially the posterior division of the femoral nerve and the accessory obturator nerve. High volumes and plane blocks should be critically examined due to the high degree of variants in anatomy (e.g., the presence or absence of the accessory obturator nerve described in the above studies), and the missing regarding of anatomical variants in health curriculum. 24 Probably, a more individualized approach of nerve blocking may be beneficial. Further studies are required.
It appears that new peripheral nerve blocks can be realistically studied on cadavers. Various types of human cadavers are utilized in US investigations, each with unique advantages and disadvantages. None of the studies were conducted on formalin-fixed body donors, as formalin causes a loss of the natural flexibility of the body tissues 25 and therefore the “feeling” of the US injection procedure is not comparable with injection on living subjects. A higher injection pressure must be generated to inject the fluid even though the quality of ultrasound imaging in formalin-preserved cadavers seems to be sufficient and comparable with the sonographic image quality of living subjects. 26 In contrast, soft-embalmed cadavers retain a more authentic texture; however, they are prone to mold if not stored properly, and their embalming process is more intricate and expensive compared with that of formalin-embalmed cadavers. 27
The sonographic quality of fresh frozen cadavers is comparable with that of living subjects, aside from the lack of blood flow. This absence of blood flow should not be underestimated, particularly when comparing ultrasound versus not US-guided nerve blocks on cadavers. An anesthesiologist experienced in nerve blocks can successfully perform a PENG block without any ultrasound assistance, as shown in the study by Hamra et al 18 (even though the investigator is not described in detail). However, this should not lead to the misconception that the use of ultrasound is unnecessary because with US guidance it is possible to detect anatomical variations and avoid vessels along the injection pathway, thus avoiding undesirable effects such as bleeding. 28
In the long term, the goal should be to fully exploit the capabilities of increasingly sophisticated ultrasound equipment systems and to perform nerve or nerve branch blocks as precisely as possible using minimal volumes. The study of even the smallest communicating branches such as the communicating branch of Berrettini via sonography underline the ongoing improvement of sonographic quality and provide progressively more insights into neural structures. 29 The barrier to histological analysis is already being affected. 30 Testing on cadavers should be intensified, providing the advantage of exchanging anatomical knowledge across disciplines. A further opportunity to provide a more precise blockade of the surgical operation site could be to fully utilize the radiological findings prior to anesthesiologic consultation (e.g., CT examinations) to identify individual anatomical variations.
Prior scoping reviews have indicated that US-guided labeling techniques were very accurate and that the spread of the injectate can be examined reliably.8,31 Therefore, US-guided nerve blocks can be practiced and refined on cadavers, which will inevitably lead to improved patient care. In addition, US-guided decompression of nerves on cadavers demonstrates this benefit clearly. Such US-guided decompressions were tested for example on the median,32,33 ulnar,34,35 sciatic,36,37 and suprascapular nerves 38 of human cadavers among other reasons that entrapment neuropathies are a common condition that are usually caused by mechanical irritation of the nerve and can therefore often only be corrected mechanically. 39
The procedures in the current review were conducted with rigor and transparency, adhering to a protocol registered in the OSF Registries. To ensure a comprehensive literature review, the investigation incorporated searches across five digital bibliographic databases as well as an exploration of gray literature. Given the initial objective of examining all ultrasound studies performed on cadaveric specimens, the search terms were intentionally broad. Due to the abundance of data retrieved, the study focused on analyzing a subset of the data. Consequently, the search yielded many studies, making the title and abstract screening process time-consuming and potentially prone to errors.
Conclusion
The present scoping review is the first comprehensive review of sonographic studies on human cadaveric nerves in general with deeper focus on the PENG block. US-guided labeling techniques in human cadavers are a widespread tool to examine the spread of the injectate. These results suggest that PENG blocks should be further investigated on cadavers to determine the MEV90 for the targeted nerves of the PENG blocks and to test possible novel injection pathways of these nerves.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793241303167 – Supplemental material for Pericapsular Nerve Group (PENG) Block on Cadavers: A Scoping Review
Supplemental material, sj-docx-1-jdm-10.1177_87564793241303167 for Pericapsular Nerve Group (PENG) Block on Cadavers: A Scoping Review by Felix Margenfeld, Adib Zendehdel, Amélie Poilliot, Giorgio Tamborrini, Matthias Beck and Magdalena Müller-Gerbl in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-2-jdm-10.1177_87564793241303167 – Supplemental material for Pericapsular Nerve Group (PENG) Block on Cadavers: A Scoping Review
Supplemental material, sj-docx-2-jdm-10.1177_87564793241303167 for Pericapsular Nerve Group (PENG) Block on Cadavers: A Scoping Review by Felix Margenfeld, Adib Zendehdel, Amélie Poilliot, Giorgio Tamborrini, Matthias Beck and Magdalena Müller-Gerbl in Journal of Diagnostic Medical Sonography
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.