
Abstract
The intrauterine device (IUD) is a popular contraception choice for women worldwide, due to a low failure rate. Although it is highly effective, it does not eliminate the risk for an ectopic pregnancy. An ectopic pregnancy occurs when a previously fertilized ovum implants outside of the uterus that can become life-threatening. In this case study, a female patient presented to a freestanding emergency department with abdominal pain, without bleeding. A sonogram showed a normal uterus with an IUD in the correct location, normal ovaries, as well as significant fluid in the pelvis and abdomen. A pregnancy test was ordered after imaging, which came back as a positive result. The patient’s blood pressure as well as her complete blood count continued to decrease, and she underwent surgery that revealed a ruptured ectopic pregnancy in the right fallopian tube and hemoperitoneum. This case highlights the importance that a properly placed IUD, without issue, does not exclude the possibility of an ectopic pregnancy.
Keywords
Intrauterine devices (IUDs) used for contraception are popular because they are reversible, long-acting, do not require much maintenance, and have a 99.8% efficacy rate. 1 That statistic is encouraging, although if there is contraception failure, the risk of ectopic pregnancy is more than four times than that of oral contraceptive users. 2 Ectopic pregnancies affect roughly 1% to 2% of women of reproductive age 3 and occur when a zygote (fertilized egg) implants in a location other than the uterus. These pregnancies can be located in several areas including the fallopian tube being the most common at 98%, Cesarean scar, cervical, ovarian, or abdominal. 4 In the instance that the ectopic pregnancy ruptures, it can lead to hemoperitoneum, which is a life-threatening condition. Visualizing free fluid in the right upper quadrant has a 99.5% association resulting from a ruptured ectopic. 5
Case Report
A 19-year-old female came into a standalone emergency medicine site with the complaint of lower abdomen pain that radiated into her pelvis. The pain began 9 hours prior to her arrival to the facility. She experienced nausea and dizziness in addition to this pelvic pain. The patient was in a great deal of discomfort and was unable to empty her bladder prior to having a sonogram. Her last menstrual period (LMP) was two weeks prior; she had a Mirena IUD placed since January 2023, without previous issues, and had never been pregnant. A transvaginal sonogram was ordered within the first hour of her arrival.
Clinical Findings
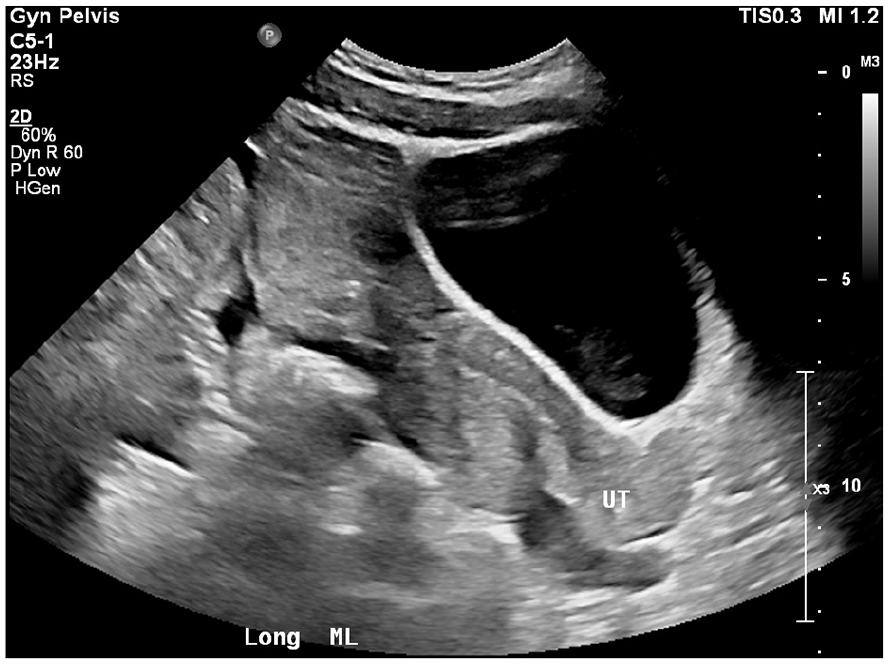
The transvaginal sonographic protocol began with sagittal and coronal images of the uterus and endometrium. In the initial image, it was apparent that there was a substantial amount of heterogeneous free fluid surrounding the uterus and ovaries (See Figure 1). Cine loops were acquired in both sagittal and coronal imaging planes to show that the IUD was in the correct location as well as the use of three-dimensional (3D) imaging (See Figure 2). Color and spectral Doppler images were obtained to confirm normal arterial and venous blood flow, within the right and left ovaries, although both were surrounded by complex fluid (See Figure 3). Transabdominal imaging was performed, and it was evident that the fluid was more extensive than originally visualized transvaginally, as the fluid extended proximally within the abdomen, as well as in Morrison’s pouch and over the dome of the liver (See Figures 4 and 5).

An example sonographic sagittal view of the uterus, which demonstrated a large volume of complex fluid, from the cul de sac to above the uterine fundus.
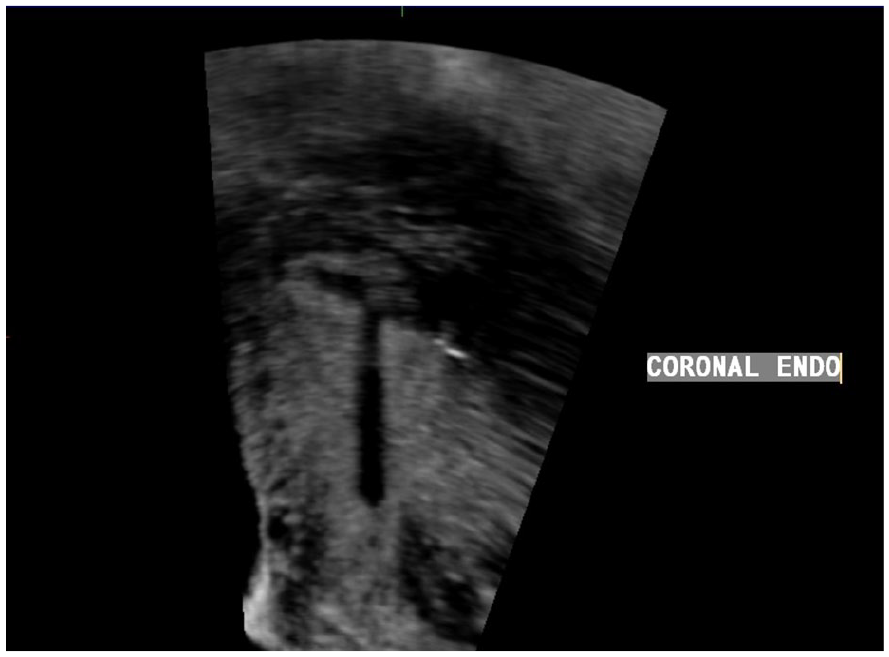
This 3D image provided confirmation that the Mirena IUD was in proper location, within the endometrium.

A sonographic sagittal image of the right ovary surrounded by complex fluid.
This transabdominal sonographic view of the patient’s pelvis showed substantial heterogeneous fluid extending beyond what was visualized transvaginally.

This sonographic view of the abdomen demonstrated fluid within Morrison’s pouch confirmed extensive fluid within the abdomen.
An adnexal mass was not visualized transvaginally or transabdominally, due to the large amount of heterogeneous fluid. The sonographer raised concern for ectopic pregnancy to the nursing staff. A pregnancy test was ordered by the emergency medicine physician. The imaging report was completed prior to the Beta HCG (human chorionic gonadotropin) lab being completed.
The result of that test had a lab value of >2000 IU/L (international units per liter) with a threshold of >5 IU/L representing a patient who is pregnant. A complete blood count (CBC) showed that her hemoglobin was that of 11.4 grams per deciliter (e.g., reference range of 11.8-16.1 g/dL) and hematocrit of 32.8% (e.g., reference range of 36.5%-48.9%), which is suggestive of anemia. During the time between the positive pregnancy test and the hospital transfer, the patient’s blood pressure dropped significantly to 98/56 mm Hg with an increased heart rate of 102 bpm. She received intravenous fluids, and her systolic blood pressure was 118 by the time emergency services arrived to transfer to the hospital, to receive a higher level of care.
The patient underwent a diagnostic laparoscopy, upon arrival, to reveal a right ruptured tubal ectopic pregnancy that was actively bleeding, resulting in 1600cc hemoperitoneum. The uterus and ovaries were reported to be normal. While in the hospital, she had a second CBC drawn at noon that showed her hemoglobin at 7.1 and hematocrit at 20.3%. Post-surgical treatment included two red blood cell transfusions, the first being 116.67 mL and the second being 300 mL. The patient was discharged home with pain medication at 16:30 4:30pm that same evening without any further complications.
Discussion
IUD usage within women of reproductive age is very common, in the United States, accounting for roughly 4.4 million users. 6 Those patients who experience IUD failure have an ectopic pregnancy risk of 15% to 27%. 7 Symptoms of an ectopic pregnancy can be nonspecific including pelvic pain, vaginal bleeding, or mimic other conditions such as a kidney stone or appendicitis, 8 which makes it initially challenging to discern. Abdominal pain and vaginal bleeding are the two most frequent presenting symptoms with a tubal ectopic pregnancy with bleeding being more common than only pain. 9 The patient reviewed in this case study did not experience vaginal bleeding, which made her scenario additionally thought-provoking. It initially appeared that she had nonpregnancy-related pain, until it was discovered that she was hemorrhaging internally from a ruptured tubal ectopic pregnancy.
Risk factors for an ectopic pregnancy include age, prior ectopic pregnancy, injury to the fallopian tubes, smoking, infertility, and contraception failure. 10 There are 4% to 6% of maternal deaths attributed to massive internal bleeding from a ruptured ectopic pregnancy. 10 The gestational sac that has been implanted within the fallopian tube continues to expand and eventually the tube ruptures causing bleeding to follow. 10 Those patients who have ruptured can present with signs of shock such as hypotension and tachycardia 2 just as the case study patient had with a heart rate of 102 bpm and blood pressure of 98/56.
The patient’s inability to void her urinary bladder, prior to the exam, could initially be seen as a limitation for a transvaginal sonogram; however, it did allow for the pelvic anatomy to be visualized, through the full bladder, during transabdominal imaging. The acoustic window made it possible to see the extent of the large volume of complex fluid, within the pelvis. The possibility of a ruptured ectopic should not be excluded in a situation where an adnexal mass is not visualized; there is significant complex fluid that extends to Morrison’s pouch, although an IUD is in proper position, within the endometrial canal.
A comparative case study 2 followed a 21-year-old woman who was treated at her community emergency department, for abdominal pain and syncope. She had a previously placed IUD, without issue, and reported no vaginal bleeding. Her blood pressure was documented at 78/64 mm Hg, which increased after a saline bolus to 101/55 mm Hg; however, laboratory results revealed she was anemic. These factors along with her symptoms pointed to the potential of hemoperitoneum and transabdominal sonography demonstrated free fluid in Morrison’s pouch and an IUD in proper location, within the uterus. A urine pregnancy test result was positive, and the patient had a transvaginal sonogram, where a 10-cm mass was visualized posterior to the uterus, as well as free fluid and the lack of an intrauterine pregnancy. The patient was then given a blood transfusion and transferred via air ambulance to the regional care center to receive a higher level of care. Upon arrival, she was taken to surgery, and the ectopic was in the posterior cul-de-sac and lateral to the rectum, in addition to significant hemoperitoneum that was removed. The patient recovered well and was discharged later in the day.
The similarities between that case 2 and the present study are noteworthy since both women were close in age, were nulligravida, did not experience vaginal bleeding, required blood transfusions, and experienced ruptured ectopic pregnancies. The two major differences were presenting symptoms and where the ectopic was located. The patient who was followed in the present case study was nauseous, and her ectopic was in the right fallopian tube. This is in comparison to the comparative case study, 2 as the patient experienced syncope, and the ectopic pregnancy was in posterior cul-de-sac.
An additional case report 3 detailed a 30-year-old woman who had two previous full-term pregnancies, presented to emergency medicine for abdomen pain, as well as vaginal spotting for three weeks. A point-of-care bedside sonogram demonstrated fluid within the pelvis, the IUD in proper location, and a large heterogeneous mass within the right adnexa. The patient was then taken to surgery where it was discovered that she had a ruptured right tubal ectopic pregnancy, with a hemoperitoneum of 100 mL. She was discharged later that day without further complications.
In the comparison report, 3 the patient experienced a ruptured tubal ectopic pregnancy while having an IUD in the appropriate location, which is like the present patient case. The differences between the two scenarios are an 11-year age difference between patients and that the patient had two children prior to the ectopic. This contrasts with the present case where the female did not have any prior pregnancies. Vaginal spotting was a symptom for the older patient and was not a symptom that this patient reported. The emergency department was aware that the older patient 3 was pregnant due to a positive pregnancy test prior to any imaging while a positive blood pregnancy test was not available, until transvaginal and transabdominal imaging was completed. The amount of hemoperitoneum was considerably minimal at 100 mL for the 30-year-old compared to the 1600cc resulting in two blood transfusions for this patient. Otherwise, both women experienced a right tubal pregnancy that required surgical intervention, and fortunately, no additional difficulties afterwards.
In some instances, an IUD can migrate outside of the endometrial cavity. In another published case, 11 a 34-year-old woman presented with vomiting and abdominal pain for three days, as well as vaginal bleeding for five days. She was para 1, gravida 2, and had an IUD in for two years, without issues. The patient had been seen by a provider, a year prior, to remove the IUD, in order to conceive. The strings were not visualized, and the IUD was not seen on the sonogram. Follow-up care was not completed until the above symptoms began and she was seen in the emergency department. An HCG lab result of over 7000 mIU/mL revealed that the patient was pregnant. A transvaginal sonogram showed a mass in the left adnexa, complex free fluid within the pelvis that reached up into Morrison’s pouch and no signs of pregnancy, within the uterus. Upon surgical intervention, the IUD was found to be embedded within the fimbrial end of the left fallopian tube, along with a ruptured ectopic pregnancy in the ampulla, and 700 mL of hemoperitoneum was also removed. The patient was discharged the following day and was able to conceive three months later.
The major distinctions between this previous case report 11 and the present study was the age difference of 13 years, the older patient has been pregnant previously, had nausea and vaginal bleeding, previous complications with her IUD, minimal internal bleeding, a left adnexal mass was visualized sonographically, and an IUD that migrated into left fallopian tube. Similarities between the two scenarios were that both women sought emergency medical care, had IUDs, underwent surgery, and were diagnosed with ruptured ectopic pregnancies.
This current case report highlights the importance of recognizing the signs of a ruptured ectopic pregnancy even when presenting symptoms and contraception history does not initially indicate a diagnostic concern. The use of transvaginal and transabdominal sonography can provide critical information that can expedite medical diagnosis, in an emergent situation.
Conclusion
The utilization of sonography for female patients, with pelvic pain, is critical in determining a diagnosis and treatment. Transvaginal sonography is commonly used to aid in diagnosing women who present with pelvic pain, especially those with an IUD. Those patients with an IUD are still at risk of an ectopic pregnancy even in situations where the device has not caused prior complications. Sonographers should be prepared to notify nursing staff or the interpreting physician of the concern for an ectopic pregnancy if they encounter a similar patient, especially considering the large amount of pelvic fluid and a properly placed IUD. As mentioned previously, the fact that a woman has an IUD without complications does not mean that the patient could not be pregnant and need emergent intervention.
Footnotes
Ethics Approval
Ethical approval was not sought for the present study since it did not comprise of a research study. The case study presented is for educational purposes only.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.