
Abstract
Klippel-Trenaunay syndrome (KTS) is a rare congenital disorder characterized by a port-wine stain birthmark, venous anomalies, and soft-tissue hypertrophy. Diagnosis of KTS is made based on two of the three characteristic diagnostic features. Klippel-Trenaunay syndrome is unilateral and more commonly affects the lower extremities. This case report describes a unique patient who lacked a patent deep system in the affected limb, making the traditional treatment of varicosities a dangerous outcome for this patient.
Klippel-Trenaunay syndrome (KTS) is a rare congenital abnormality that is caused by the failure of the blood vessels or lymph vessels to properly develop. A noninherited genetic mutation in the PIK3CA gene is believed to be responsible for these malformations. Klippel-Trenaunay syndrome is a sporadic disease with no distinct family history. 1 Characteristics of KTS include a port-wine stain birthmark, venous anomalies, and soft-tissue hypertrophy.
This case study describes a 37-year-old Caucasian woman, who presented for a standing reflux sonogram and had a history of right leg varicose veins, port-wine stain birthmark, and pain. The results of the examination found a diminished femoral vein with no visualization of the popliteal vein and distal calf veins. Prominent varicose vein collaterals were seen along the lateral thigh, knee, calf, and foot.
Case Report
A 37-year-old Caucasian woman reported to the vascular lab for a standing venous reflux study and evaluation of the varicose veins, on her right leg. The patient had a history of a port-wine stain birthmark on the right leg, a history of right leg varicose veins, and limb enlargement. Significant varicose veins extended from the lateral right leg onto the foot. The toes of the right foot were discolored. Large vascular malformation was present on the right lower thigh/upper calf with large collateral vessels in the leg and upper thigh, and smaller vascular malformations in the right foot. The patient had a previous consultation with vein care, and surgery was scheduled to remove the vein, but the patient was hesitant to proceed with surgery and wanted a second opinion. The patient had no significant family history.
The patient had a magnetic resonance imaging (MRI) examination and an MRI angiogram/MRI venogram of the right lower extremity, in 2009. The MRI examination did document her right-sided varicosities (see Figure 1). The interpreting physician reported a probable absence of the femoral vein and popliteal vein, as well as the deep calf veins. A correlation with sonography was recommended. Large superficial vessels were seen in the leg and thigh which connected to a large vessel extending from the common femoral vein. A large area of prominent vessels was noted surrounding the knee. A large vessel was seen at the ankle as well as an enhancing vessel in the mid tibial region, which may have been vascular. Vessels in the foot could not be evaluated due to limited field of view. A conventional angiogram was recommended to further evaluate the flow dynamics and other details of the vascular abnormalities. No further diagnostic imaging was performed following the MRI until 2023.
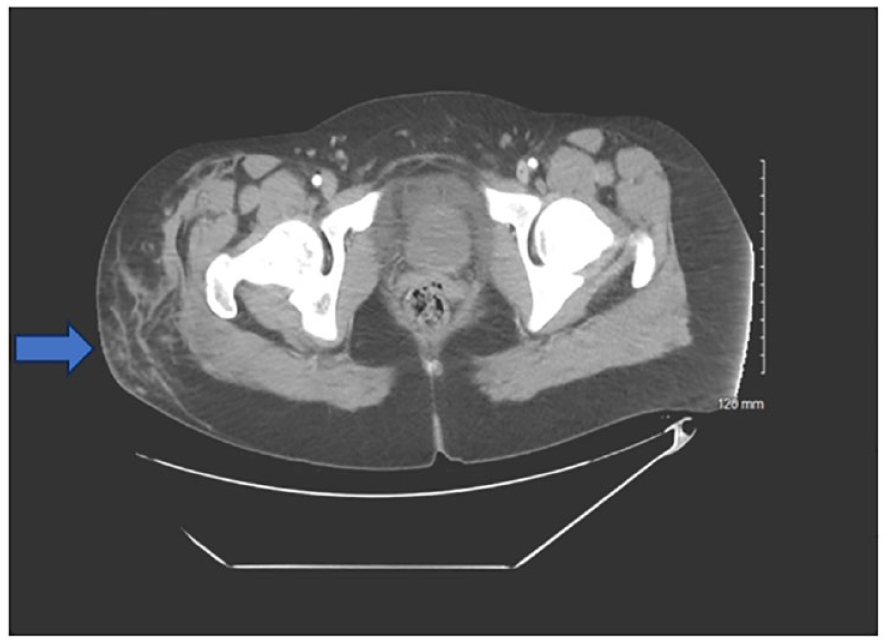
This axial T1 magnetic resonance imaging slice demonstrates varicosities on the right side of the patient (noted by blue arrow).
The patient had a standing venous reflux sonogram study performed with Epiq Elite (Philips Healthcare, Bothel, WA), in June 2023, for severe right leg varicosity from the upper thigh to the foot. The patient complained of pain in the right leg and bleeding from varicosities. Her medical laboratory results indicated an elevated hemoglobin and hematocrit. No evidence of deep venous thrombosis was found. A cluster of venous structures was seen along the lateral aspect of the mid-thigh and knee joint, which may represent arteriovenous or venous malformations.
Sonographic findings showed a diminished/hypoplastic right femoral vein, as evidenced by visualization of a normal femoral vein decreasing in size and eventually disappearing as imaging progressed distally in the thigh (see Figure 2). Popliteal and distal calf veins were not visualized (see Figure 3). Prominent varicose veins and multiple venous collaterals were found along the lateral thigh, knee, calf, and foot. The right small saphenous vein was not visualized. Reflux of greater than 3 seconds occurred in the great saphenous vein at the thigh and calf (see Figures 4 and 5), with no reflux at the sapheno-femoral junction (see Figure 6). The right calf anterior arch branch was not visualized, and the posterior arch branch had reflux of greater than 3 seconds. The great saphenous vein diameter at the thigh was dilated and measured 10.6 mm (see Figure 7). A study by Hyun Joh and Park reported the average diameter of a normal great saphenous vein was 5.0 ± 2.4 mm while the average diameter of a refluxed great saphenous vein was 6.4 ± 2.0 mm2. This same study defined venous reflux as retrograde flow lasting longer than 0.5 seconds. 2 In this patient case, her physician recommended a venogram and a consultation with vascular surgery. Given the patient’s history, clinical findings of some absent deep veins, and symptoms consistent with KTS, the vascular surgeon did not recommend surgical intervention.
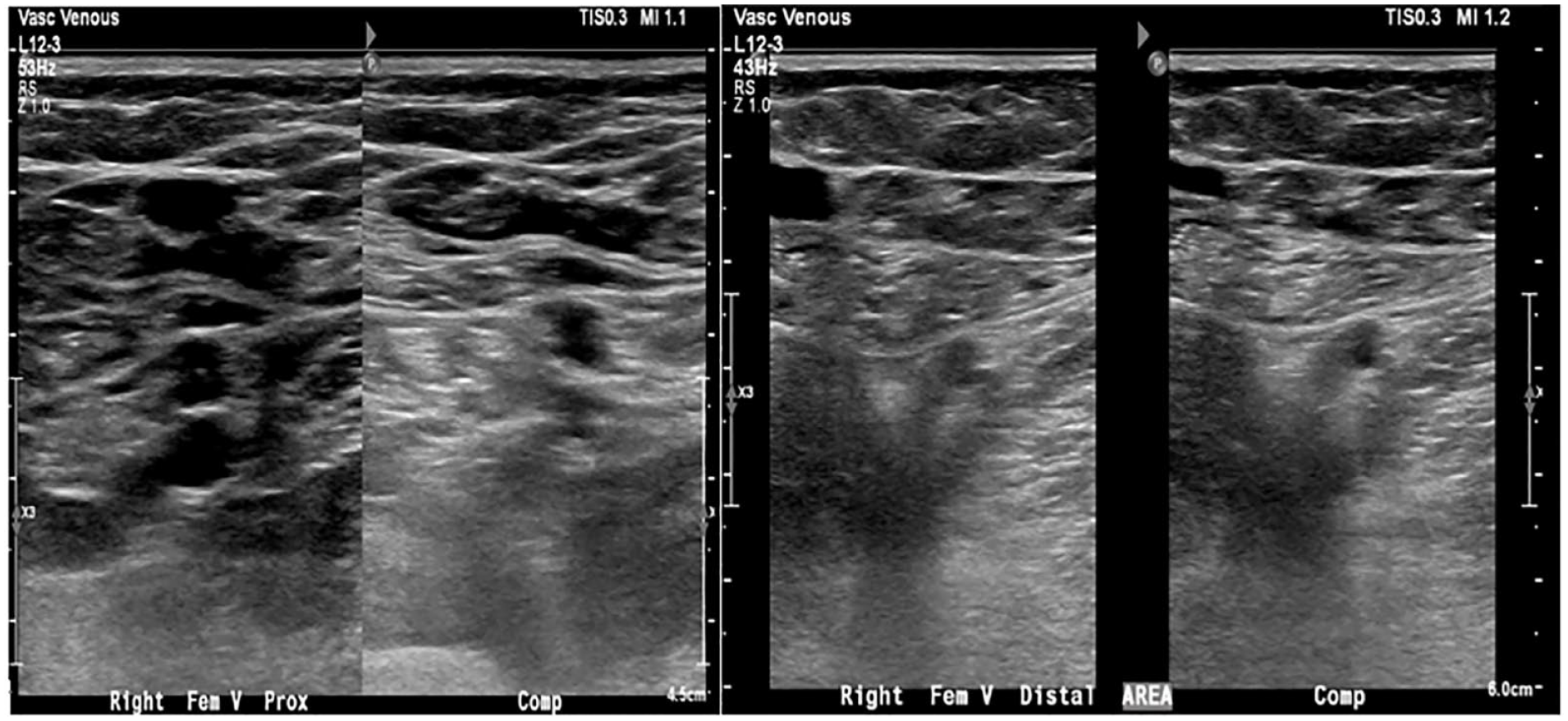
This series of dual sonographic images of the femoral vein (compression and noncompression) demonstrate the proximal vessel system but was not seen distally.
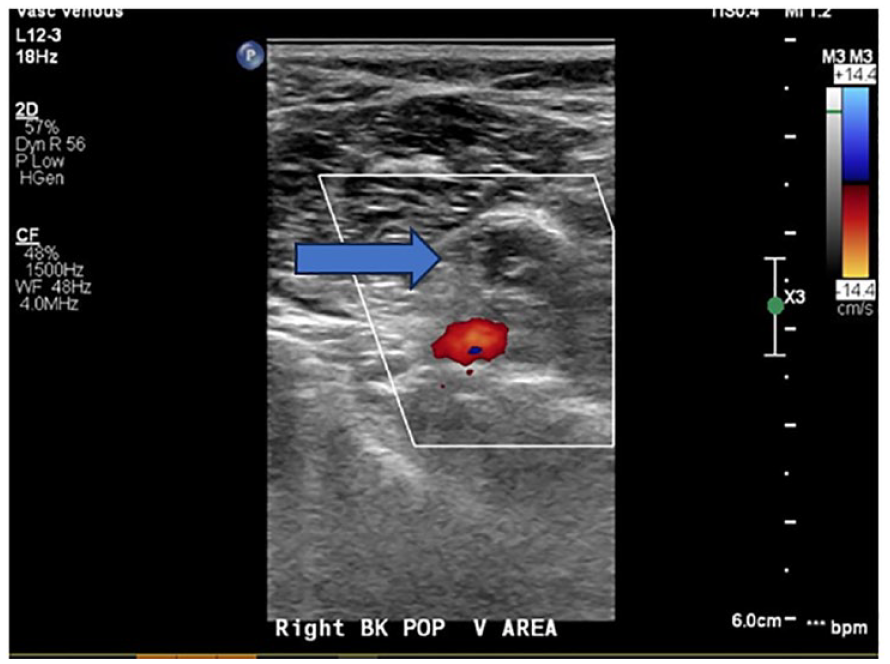
The transverse sonographic image of the popliteal area has added color Doppler, which demonstrated the right popliteal artery but a missing popliteal vein.
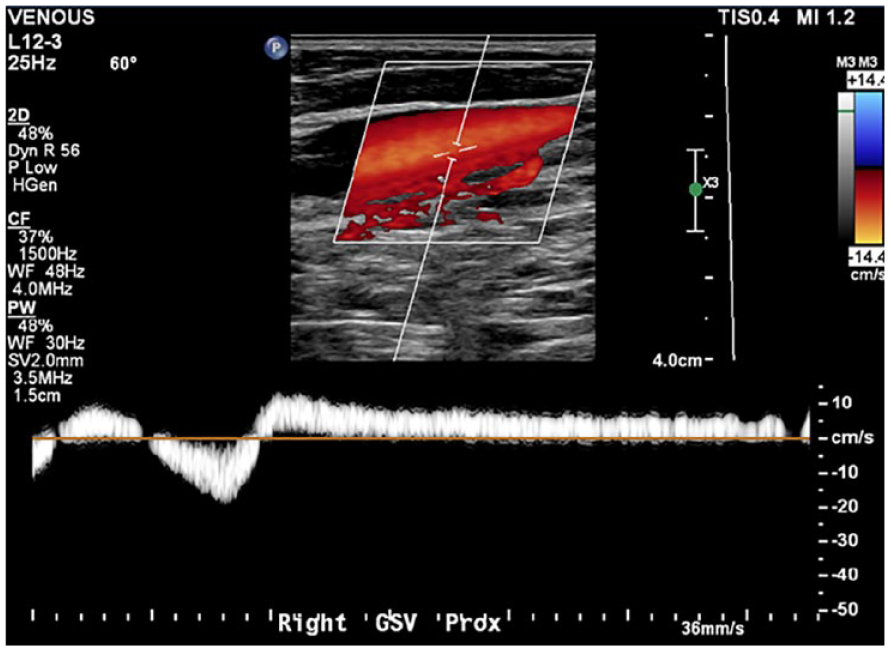
This sagittal triplex image of the right greater saphenous vein documented reflux of greater than 3 seconds, at the proximal portion of the vein.
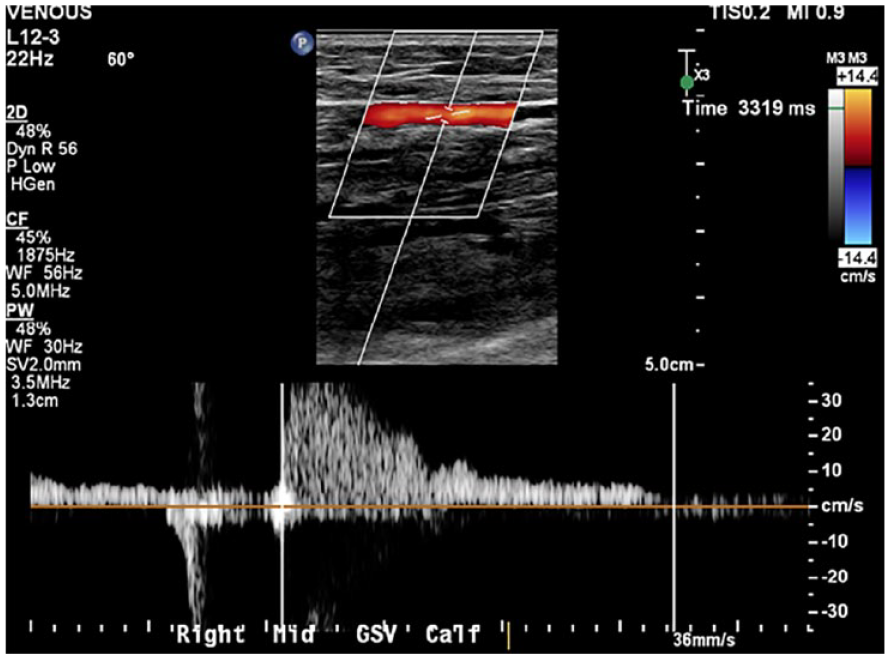
This sagittal triplex image of the right greater saphenous vein documented reflux of greater than 3 seconds, at the mid portion of the vein.
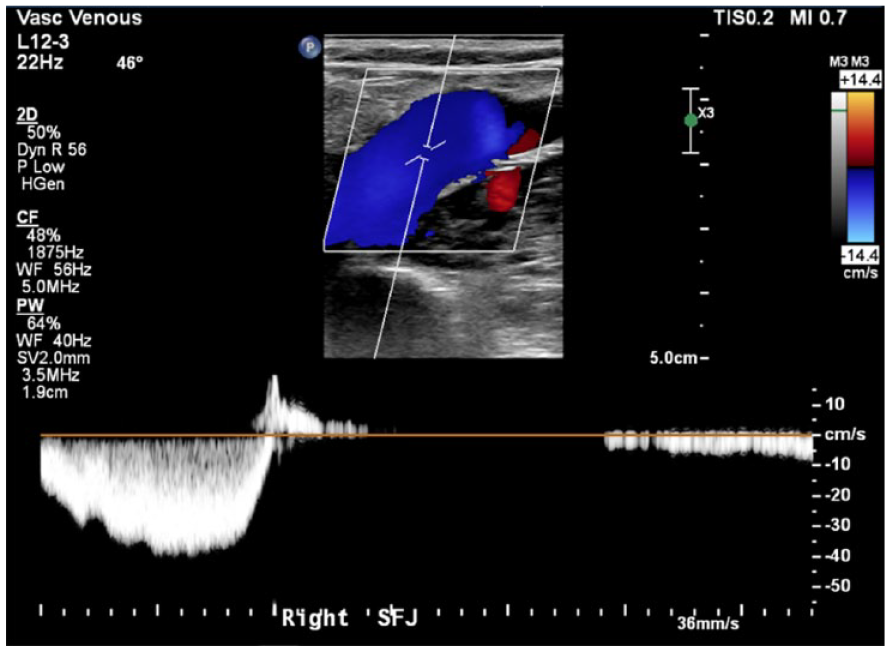
This sagittal triplex image of the right sapheno-femoral junction vein documented a lack of venous reflux.
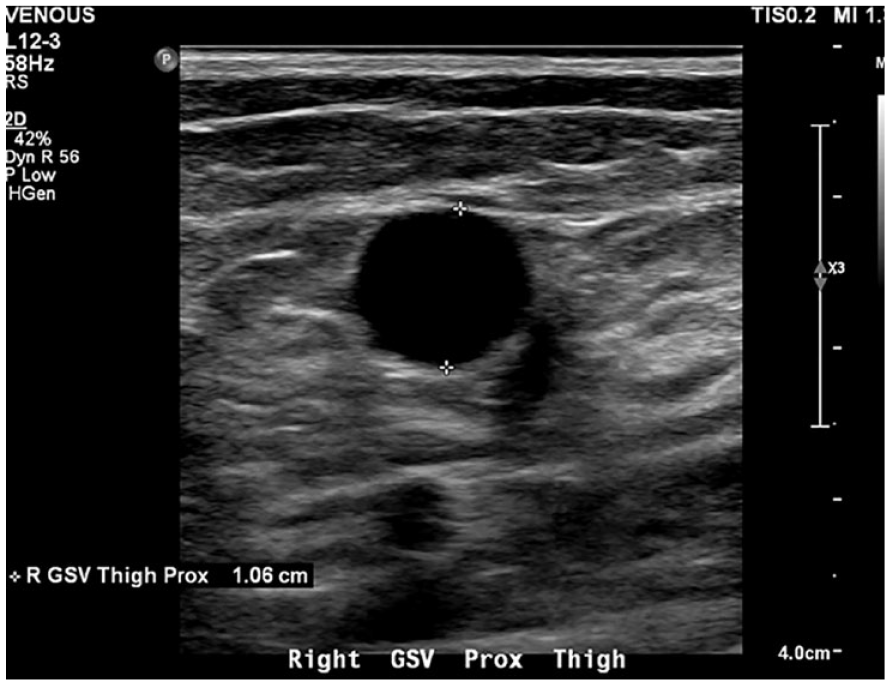
This transverse sonographic view of the greater saphenous vein, at the level of the thigh, had a diameter of 1.06 cm.
Discussion
Klippel-Trenaunay syndrome is diagnosed clinically based on physical signs and symptoms. Pain, swelling, lymphedema, bleeding, superficial thrombophlebitis, and deep vein thrombosis are symptoms of KTS. 3 Clinical features of KTS include port wine stain, lymphatic, and venous malformations with overgrowth of the affected limb. 1 Venous anomalies are the most common vascular malformation found in KTS. These anomalies can affect the superficial and deep venous systems. 4 Deep vein atresia has been reported in a small number of KTS patients. 5 The femoral and popliteal veins are the most affected deep veins. 5 Port wine stains have been reported in 98% of KTS cases while varicosities have been reported in 72% of cases. 1 Lymphatic malformations occur in 11% of KTS patients. 1 Limb hypertrophy occurs in 67% of KTS patients, with 88% involving the lower limb and 71.5% involving a single limb. 1
A multidisciplinary approach is essential for the diagnosis and evaluation of KTS. Magnetic resonance imaging is used to evaluate the full extent of underlying vascular malformations in KTS. 4 Sonography can be used to examine the presence and size of persistent embryonic veins in superficial locations. Macrocystic lymphatic malformations and superficial blood clots can be identified with the use of sonography. 4
The treatment of KTS involves symptom management. Compression garments are used to reduce limb swelling, venous engorgement, and discomfort, and sclerotherapy may be used to treat macrocystic lymphatic malformations. 3 Sirolimus has been used in some KTS patients to offset the progression of vascular malformations and improve symptoms. 4
The prognosis of KTS depends on the extent of the disease and potential complications. 3 Pulmonary emboli have been reported and some patients may develop chronic thromboembolic pulmonary hypertension.3,4 The severity of KTS can vary widely from cosmetic deformity to severe disability, chronic pain, and blood clots.
The three primary clinical features of port-wine stain, varicosities, and limb hypertrophy in our case are similar presentations to other reported cases of KTS.6–8 The current patient case differs from those published as this patient did not have a patent deep venous system. However, a series of cases presented by Volz et al 5 did describe several cases where the deep veins were not identified and took note of the need for careful imaging and management in these situations. The current patient was justified in questioning the vein care surgeon, who recommended superficial vein removal, as this would have limited the available venous return and been detrimental to the patient. This case report highlights the importance of ensuring proper in-depth imaging is performed to document a patent deep system before any invasive vein treatment.
Conclusion
Klippel-Trenaunay syndrome is a rare vascular anomaly characterized by vascular malformations, limb hypertrophy, and port-wine stains. Limb hypertrophy and port-wine stains can be assessed with a physical examination, but imaging is necessary to examine vascular malformations. Klippel-Trenaunay syndrome is diagnosed and managed using a multimodality approach involving MRI and sonography. Sonography is used to evaluate the extent of vascular anomalies, examine varicosities, and check for thrombus and patency of the deep system. Patients with KTS will require monitoring to prevent and manage complications of this syndrome. Some cases will have limited treatment options due to other variables, such as the current patient case that had no patent deep venous system.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because only anonymous information was used in this report.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).