
Abstract
Objective:
The aim of this study was to assess maternal, obstetric, and fetal risk factors, as well as shoulder dystocia (SD) maneuvers and perinatal outcomes, in the management of SD.
Materials and Methods:
This descriptive retrospective cross-sectional study analyzed 66 documented patient cases of SD from a pool of 36 390 singleton vaginal deliveries. This review was based on hospital deliveries that occurred between 2017 and 2022. In addition, 201 control cases were selected from a computer-assisted randomization program, which were based pregnancy, delivery, fetal, and newborn outcome data. Regression analysis was used to elucidate the relationship between SD and associated risk factors.
Results:
The SD group exhibited a significantly higher mean age (p < .05) compared with control group. Notably, the abdominal circumference (AC) measurement (sensitivity = 81.8% and specificity = 91.0%) and birth weight (sensitivity = 62.4% and specificity = 91.5%) emerged as the most significant risk factors for SD.
Conclusion:
These retrospective findings may suggest that aside from birth weight and AC measurements, other risk factors for SD demonstrate low sensitivity. This work also underscored the unpredictable nature of this obstetric complication.
Shoulder dystocia (SD) is defined as a condition requiring additional obstetric maneuvers because the fetal shoulders cannot be delivered spontaneously, after the head is delivered, during vaginal birth. In more concise terms, SD is a documented head-to-body delivery takes longer than 1 minute. 1 SD is an unpredictable and unavoidable obstetric emergency and a serious complication that occurs in 0.5%–1.5% of deliveries. 2 It is important obstetric condition because it has a high perinatal mortality and morbidity. 2 For these reasons, complications due to SD are high on the list of patient cases that are referred for obstetric malpractice. The most common fetal complication is transient brachial plexus injury (BPI) (e.g., rate of 3%–17%); other complications include clavicle (e.g., rate of 1.7%–9.5%) and humerus (e.g., rate of 0.1%–4.2%) injuries, permanent BPI (e.g., rate of 0.5%–1.6%), hypoxic-ischemic encephalopathy (e.g., rate of 0.3%) and infant mortality (e.g., rate of 0.35%). 3 Maternal complications may include vaginal and cervical tears, uterine rupture, postpartum hemorrhage, perineal tears, and even fistula in the late phase. 3 Although most patient cases of SD occur without maternal/fetal risk factors. The known risk factors include dystocia in previous births, maternal obesity, gestational, or overt diabetes, excessive prenatal weight gain, prolonged labor, fetal macrosomia, and postmature pregnancies. 4
Among the various risk factors associated with SD, diabetes is considered the most significant contributor to this obstetric emergency. 5 Elevated maternal blood glucose levels not only increase the likelihood of macrosomia but also heighten the risk of a difficult delivery, due to the larger size of the fetus. As a result, individuals with diabetes face an augmented risk of encountering SD-related complications, including brachial plexus injuries, clavicle fractures, and prolonged labor. 6
Obstetric measurements play a pivotal role in the management and prevention of SD, offering numerous benefits to health care providers and patients alike. 7 By accurately assessing fetal sonographic measures of abdominal circumference (AC), biparietal diameter (BPD), femur length (FL), and estimated fetal weight (EFW), obstetricians can proactively identify those who are at higher risk for SD 8 (see Figure 1). These sonographic measurements serve as valuable predictors, enabling health care providers to implement appropriate interventions and prepare for potential complications, during delivery.
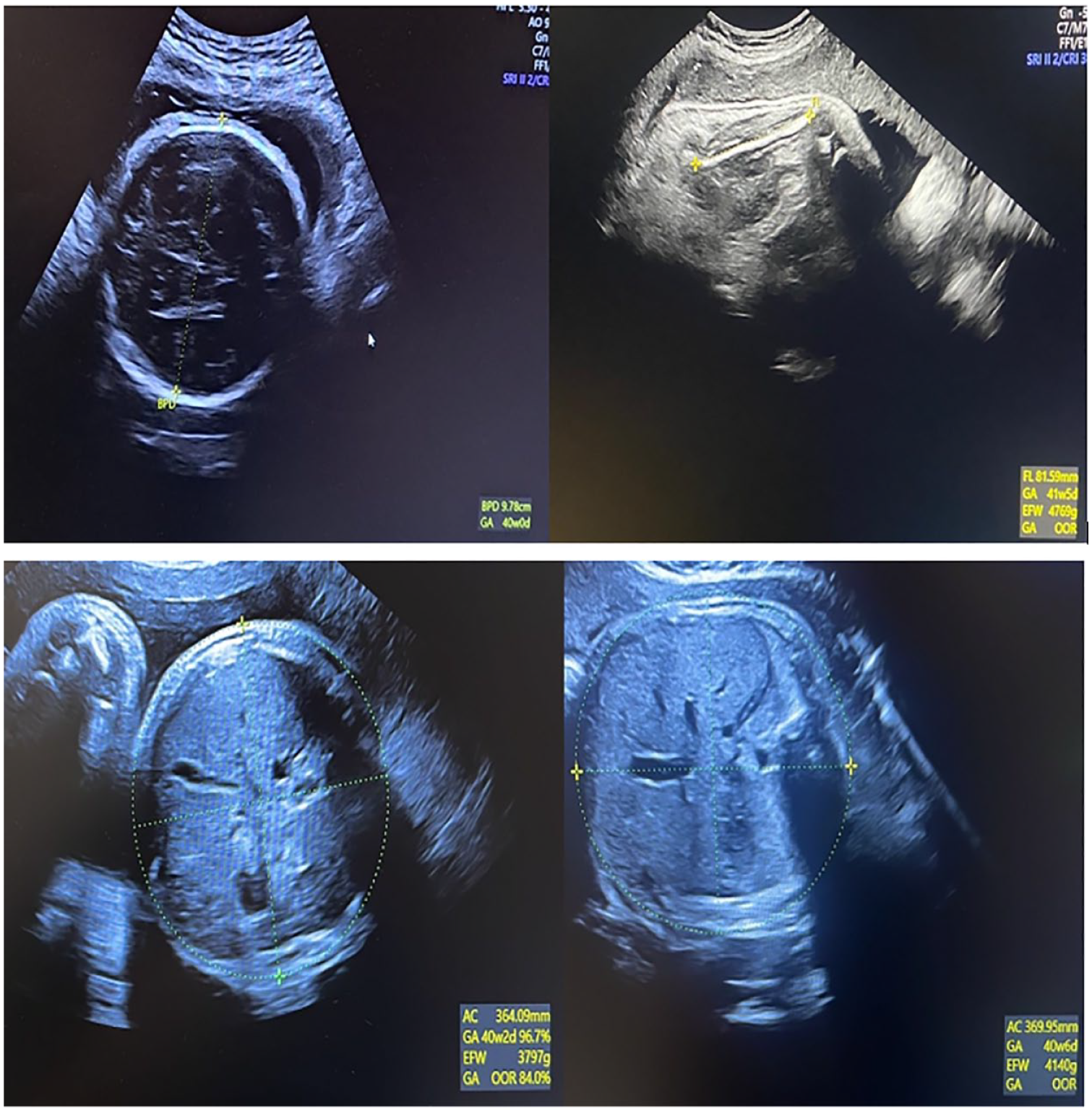
Examples of sonographic images of obstetric measurements, such as abdominal circumference (AC), biparietal diameter (BPD), and femur length (FL).
The aim of this study was to investigate the maternal, obstetric, and fetal risk factors associated with SD, as well as the maneuvers employed to manage cases of SD, as well as the impact on perinatal outcomes, in a hospital setting. By analyzing these factors and outcomes, the goal was to identify key risk factors and evaluate the efficacy of interventions.
Materials and Methods
The study was conducted as a retrospective analysis of maternal, obstetric, and fetal risk factors. In addition, it was important to capture obstetrical rescue maneuvers and perinatal outcomes associated with SD, during childbirth. Data from 66 documented patient cases of SD (e.g., incidence of 0.18%) and 201 control groups were extracted from a cohort of 36 390 singleton vaginal deliveries. These patient cases occurred between 2017 and 2022, at an obstetrics and gynecology hospital. Using a computer-assisted randomization program, 210 control groups were selected to maintain an appropriate case/control ratio and accounting for potential lost data. Subsequently, nine patient cases, from the control group, were excluded due to insufficient data.
In this study, SD cases were defined as those that required additional obstetric interventions, due to the fetal shoulders not spontaneously straighten, after delivery of the head, during a vaginal delivery. SD cases were recorded using a form titled, “Follow-up form for infants with shoulder dystocia.” This form was used for all SD cases to ensure standardization of records and to provide a legal basis for possible legal proceedings. This form contained data about the pregnancy, the birth process, the fetus, and the newborn. Pregnancy-related data include the age, height, and weight of the pregnant woman, the presence of late pregnancy, the presence of maternal diabetes mellitus (DM), gestational diabetes DM, and a history of SD, in previous deliveries. Data were also recorded based on the labor itself, such as duration of active phase and second phase of labor, duration of SD, direction of shoulder in dystocia, use of episiotomy, type of anesthesia, maneuver, and mode of delivery. In addition, the recorded data on the fetus/neonatal were as follows: EFW, AC, Apgar scores, cord blood hydrogen levels (pH), birth weight (BW), direction, newborn examination results from a pediatrician (arm weakness, clavicle fracture, admission to the neonatal intensive care unit [NICU]), and extended examination results requiring orthopedic/physiotherapeutic consultation. 9 Other data not included in this form, such as the value of oral glucose tolerance test (OGTT), hemoglobin (Hb) level before and after birth, sex of the newborn, obstetric history, and additional sonographic measurements, such as BPD, FL, were obtained from delivery records for both patient groups.
Data Analysis
The study was approved by the institutional review committee (IRB#13/32). Data were analyzed using SPSS statistical software v20.0 (IBM, SPSS Inc.). Descriptive data were presented as frequencies, percentage, mean, standard deviation, median, and range. According to the normality of the data, parametric and nonparametric methods were used to compare the dependent and independent variables. Binary stepwise logistic regression and receiver-operating characteristic (ROC) curve analysis methods were used to describe the data, as well as explaining the relationship between SD and the risk factors. The results were analyzed with a significance level p < .05 and a confidence interval of 95%.
Results
In the study, the mean age of the SD group was 28.44 ± 5.73 years, while in the control group it was 26.43 ± 5.12 years. The difference between the two groups was statistically significant (t = 2.681, p = .008). In addition, there was a statistically significant difference in both prenatal and postnatal Hb levels between the groups (p < .05). The blood glucose levels, as determined by the 50 g OGTT results were significantly higher in the SD group (z = 2.167, p < .05). In the entire patient cohort, the rate of comorbid disease was 3.7%, with DM comprising 2.2% of the cases.
While 13.6% of the SD group had comorbid disease and 9.1% had DM, 0.5% of the control group had comorbid disease (e.g., chronic diabetes mellitus, hypertension, and thyroid diseases) and none of the patients presented with DM. The difference between the two groups was statistically significant (Fisher’s exact test, p < .001) (see Table 1).
The Between Group Comparisons of Sociodemographic and General Health Characteristics.
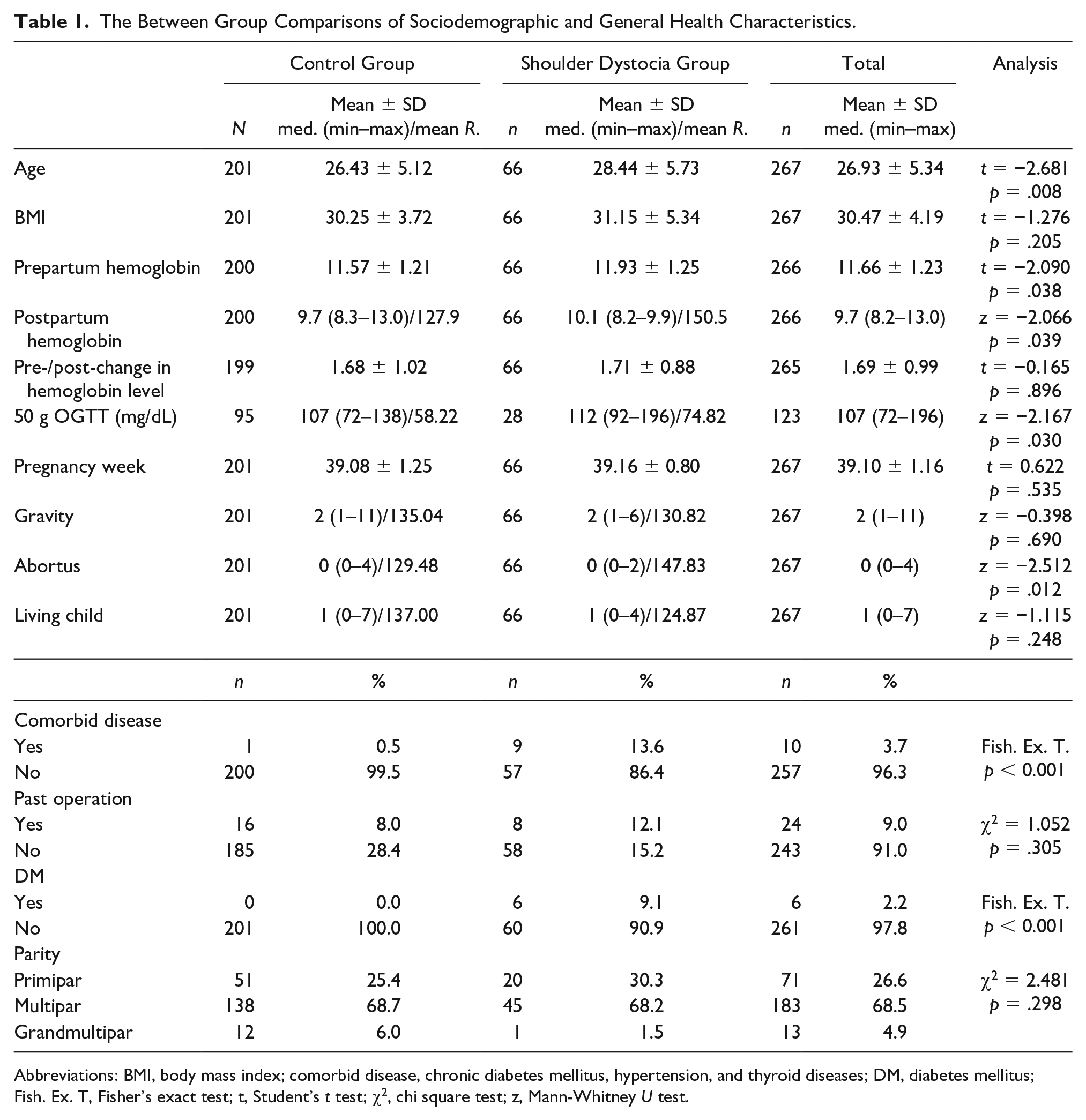
Abbreviations: BMI, body mass index; comorbid disease, chronic diabetes mellitus, hypertension, and thyroid diseases; DM, diabetes mellitus; Fish. Ex. T, Fisher’s exact test; t, Student’s t test; χ2, chi square test; z, Mann-Whitney U test.
The duration of the first stage of labor was similar between groups (p > .05), the duration of the second stage was longer in the SD group (z = 4.736, p < .001). Although the median durations of the third stage were similar, it was significantly longer in the SD group (z = 2.574, p < .05). There was no statistically significant difference between groups in the presence of preterm delivery, mode of delivery, induction status, amniotic fluid index (AFI), and placental location (p > .05). Episiotomy was performed more frequently in the SD group (χ2 = 21.174, p < .001). The mean EFW at fetal assessment was 3248.44 ± 293.26 g, in the control group and 3648.20 ± 270.22 g, in the SD group (t = 9.792, p < .001), and the BW was 3215.57 ± 365.98 g in the control group and 3879.47 ± 427.47 g in the SD group (t = 12.251, p < .001), the difference between them was statistically significant. The macrosomia rate (e.g., ≥ 4000 g) was 34.8% in the SD group, while it was 3.5% in the control group and the difference between them was statistically significant (χ2 = 49.011, p < .001). In the SD group, BPD (t = 5.573, p < .001), AC (t = 13.913, p < .001), FL (z = 6.748, p < .001), AC/BPD (z = 9.325, p < .001), EFW/FL (z = 8.265, p < .001) were significantly higher and FL/AC (z = 8.229, p < .001) and umbilical pH (t = 6.242, p < .001) values were significantly lower. The Apgar scores at the first minute (z = 7.561, p < 0.001) and the fifth minute (z = 6.803, p < .001) were significantly lower in the SD group. NICU requirements were 19.7% in the SD group and 4.5% in the control group, and the difference between them was statistically significant (χ2 = 15.221, p < .001) (see Table 2).
The Between Group Comparison of Maternal Obstetric Characteristics and Fetal-Neonatal Characteristics.
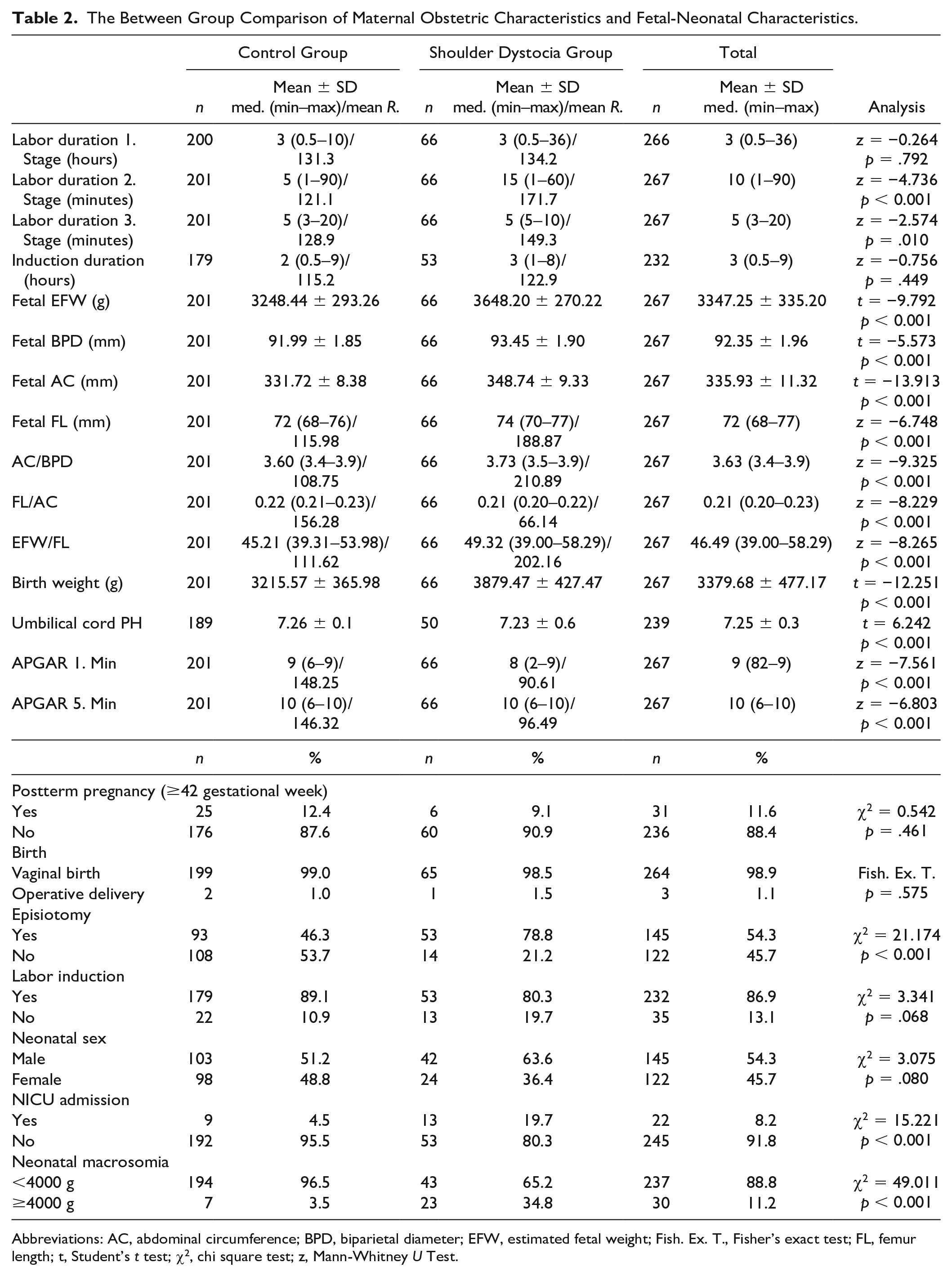
Abbreviations: AC, abdominal circumference; BPD, biparietal diameter; EFW, estimated fetal weight; Fish. Ex. T., Fisher’s exact test; FL, femur length; t, Student’s t test; χ2, chi square test; z, Mann-Whitney U Test.
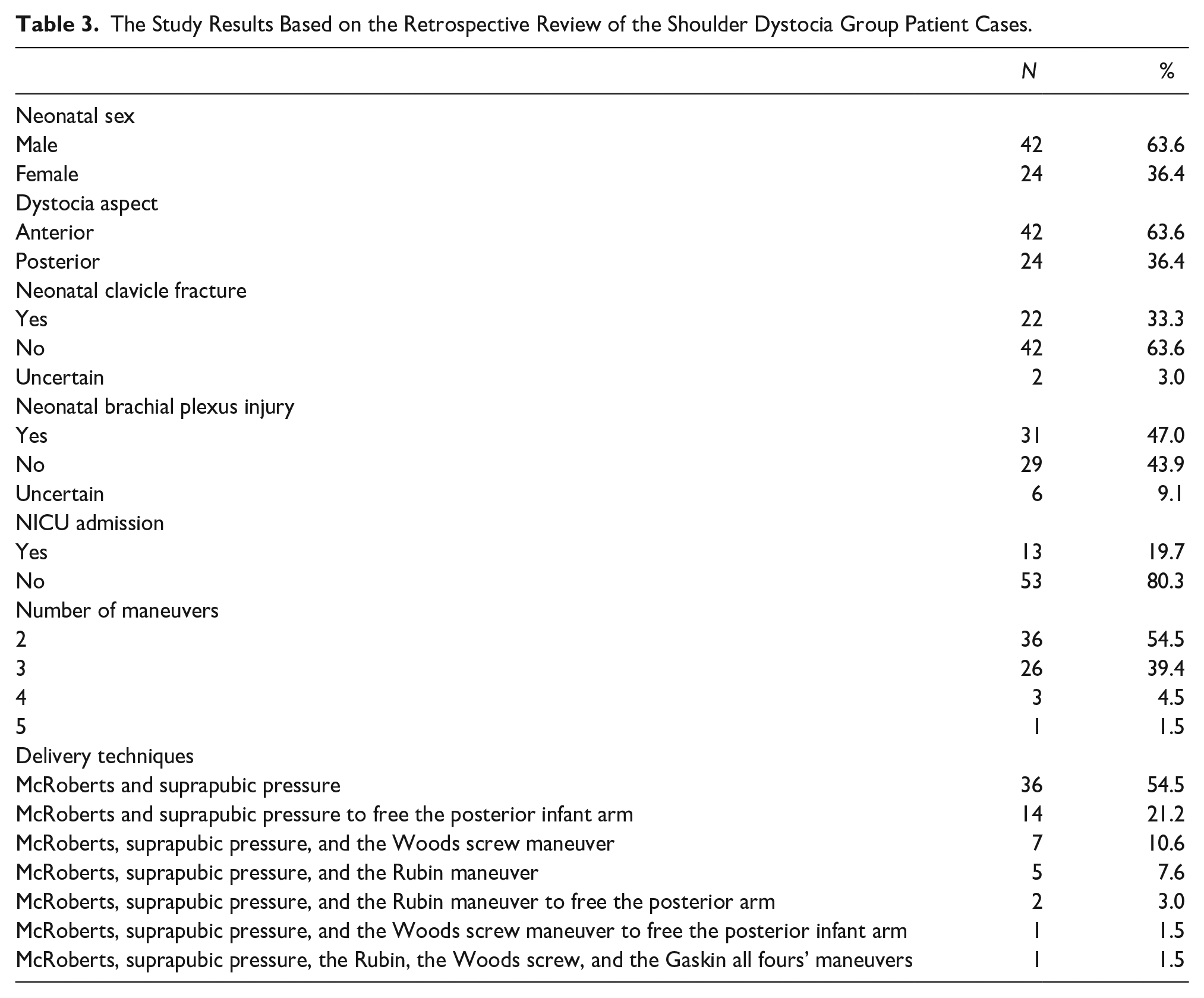
In the study, the total number of vaginal deliveries was 36 390, with a recorded incidence of SD occurring in 66 cases over a 5-year period, resulting in an incidence rate of 0.18%. Among infants affected by SD, 63.6% were male, while 36.4% were female. SD primarily occurred in the anterior shoulder in 63.6% of cases, while 36.4% involved the posterior shoulder. Infant clavicle fractures occurred in 33.3% of SD cases and in 3% the situation could not be clarified, and further investigation was recommended. Postnatal chest radiographs displayed clavicle fractures and shoulder radiographs also were included to augment the investigation of perinatal outcomes (see Figure 2). A BPI occurred in 47% of cases, with 9.1% of cases, which required further investigation, due to unclear circumstances. The referral rate to the NICU was 19.7% (n = 13). The most used maneuvers for managing SD were as follows: McRoberts maneuver and suprapubic pressure (n = 36, 54.5%), McRoberts maneuver and suprapubic pressure, to retrieve the posterior infant arm (n = 14, 21.2%), McRoberts maneuver, suprapubic pressure, and the Wood screw maneuver (n = 7, 10.6%) and McRoberts maneuver, suprapubic pressure, and Rubin’s maneuvers (n = 5, 7.6%). Wood screw maneuver (n = 7, 10.6%) and McRoberts maneuver, suprapubic pressure, and Rubin’s maneuvers (n = 5, 7.6%) (see Table 3).
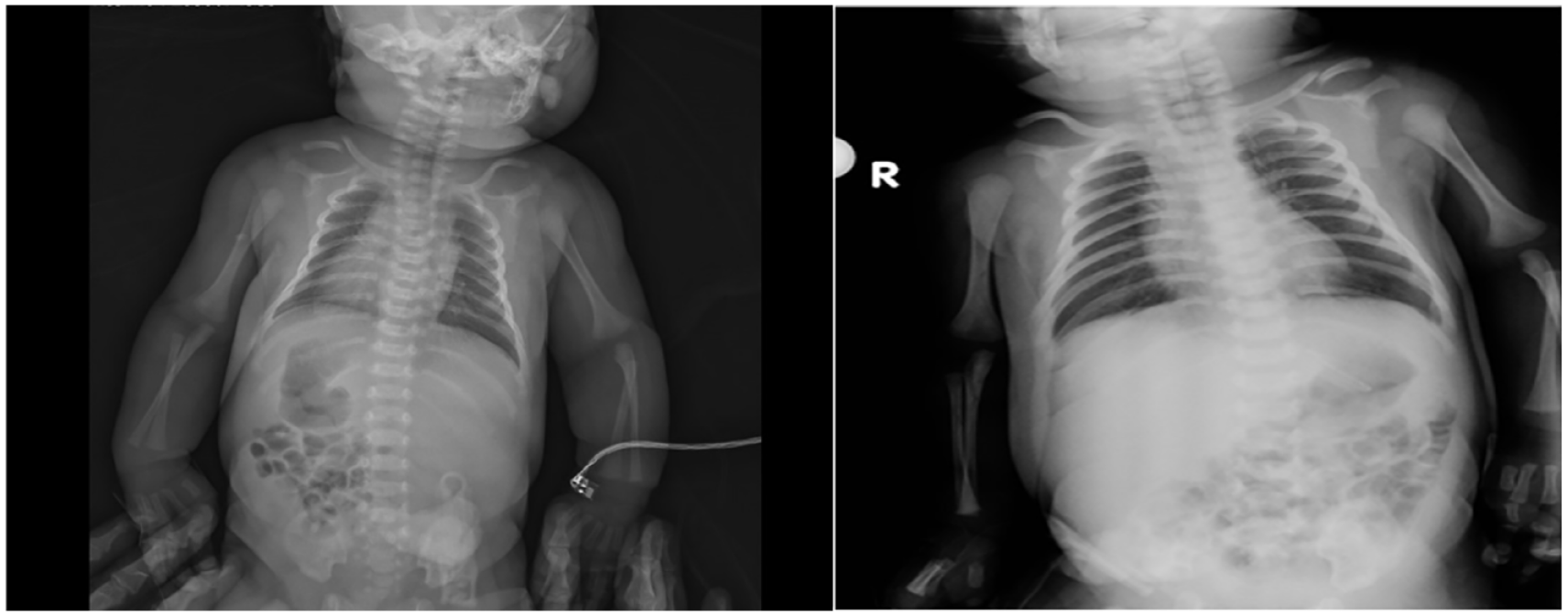
Example of postnatal chest x-rays showing clavicle fractures in cases with SD.
The Study Results Based on the Retrospective Review of the Shoulder Dystocia Group Patient Cases.
No significant risk factor for neonatal clavicle fracture and/or BPI was noted in either simple or multiple logistic regression analysis. When comparing SD cases with and without neonatal complications (e.g., clavicle fracture and/or BPI), no significant differences were found in maternal sociodemographic and obstetric characteristics. This was similar when considering the neonatal variables, such as the duration of SD, number of maneuvers performed, neonatal sex (p > .05), except for the Apgar scores. The median Apgar score at first minute was 7.5 (2–9)/26.50 in the group with complications and 9 (5–9)/43.00 in the group without complication, with the difference being statistically significant (z = 3.690, p < .001). Similarly, the median Apgar at the fifth minute was 9 (6–10)/27.11 in the group with complications and 10 (8–10)/42.18 in the group without complications, with the difference also being statistically significant (z = 3.480, p < .001). The median duration of SD was 30 (5–120) seconds.
In the simple binary logistic regression analysis conducted with variables potentially influencing SD were age, BPD, AC, FL, EFW, AC/BPD, FL/AC, EFW/FL, BW, prepartum Hb value, and duration of the second stage of labor. These all generated statistically significant associations (p < .05). In multiple binary logistic regression analysis, a stepwise model was constructed with significant variables. AC/BPD, FL/AC, and EFW/FL were excluded from the model as they demonstrated multicollinearity. The model in which prepartum Hb (g/dL), AC (cm), FL (cm), EFW (kg), BW (kg), and duration of the second stage of labor (minute) were significant and were provided in Table 4. Specifically, for each kilogram (kg) of increase in BW (odds ratio [OR] = 58.857; p < .001), each centimeter (cm) of increase in AC (OR = 48.720, p < .001), each g/dl increase in prepartum Hb (OR = 2.005, p < .05), and each minute increase in duration of the second stage of labor (OR = 1.033; p < .05), increased the risk for SD. Conversely, each kg increase in EFW and each cm increase in FL showed a significant and low negative predictive power for SD risk (OR = 0.003 and OR = 0.004) (see Table 4).
The Results of the Binary Stepwise Logistic Regression to Predict Infant Shoulder Dystocia.
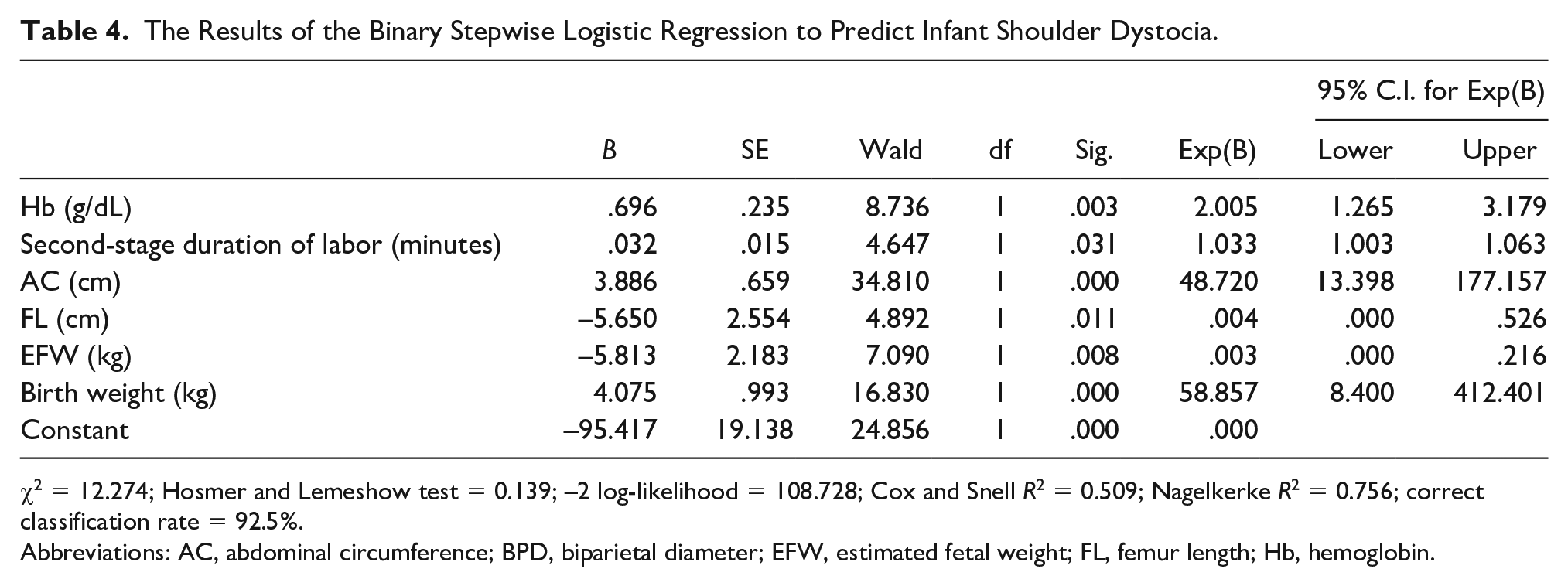
χ2 = 12.274; Hosmer and Lemeshow test = 0.139; –2 log-likelihood = 108.728; Cox and Snell R2 = 0.509; Nagelkerke R2 = 0.756; correct classification rate = 92.5%.
Abbreviations: AC, abdominal circumference; BPD, biparietal diameter; EFW, estimated fetal weight; FL, femur length; Hb, hemoglobin.
The ROC curve chart and table with SD risk factors are also provided. Examining the predictive significance of risk factors for SD, based on the size of the area under the curve, the AC was very good predictor; BW, EFW, AC/BPD, EFW/FL, and FL/AC were good predictors; FL and BPD were moderate predictors. The duration of the second stage of labor, age, and prepartum Hb were noted to be weak predictors. Among the risk factors, the sensitivity of AC was 81.8% and specificity was 91.6%. The sensitivity of BW was 62.4%, specificity was 91.5%, and the sensitivity of the other risk factors was considered low (see Figure 3 and Table 5).
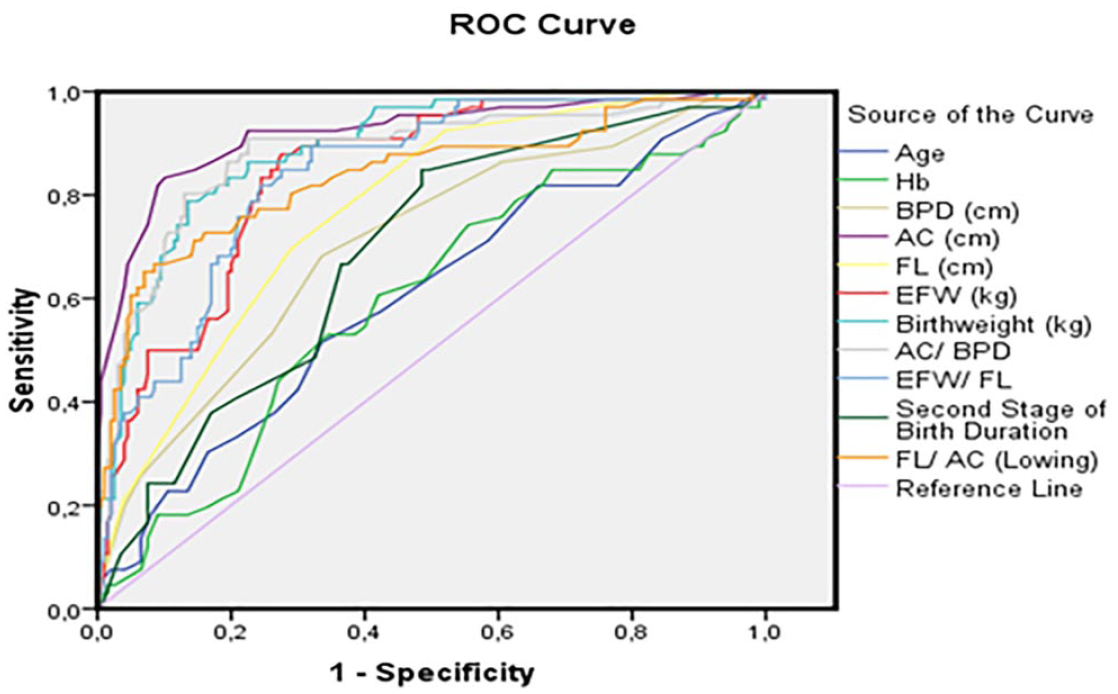
The graphic receiver-operating characteristic (ROC) curve to determine the risk factors for fetal shoulder dystocia.
The Receiver-Operating Characteristic Curve Analysis to Determine the Risk Factors for Shoulder Dystocia.
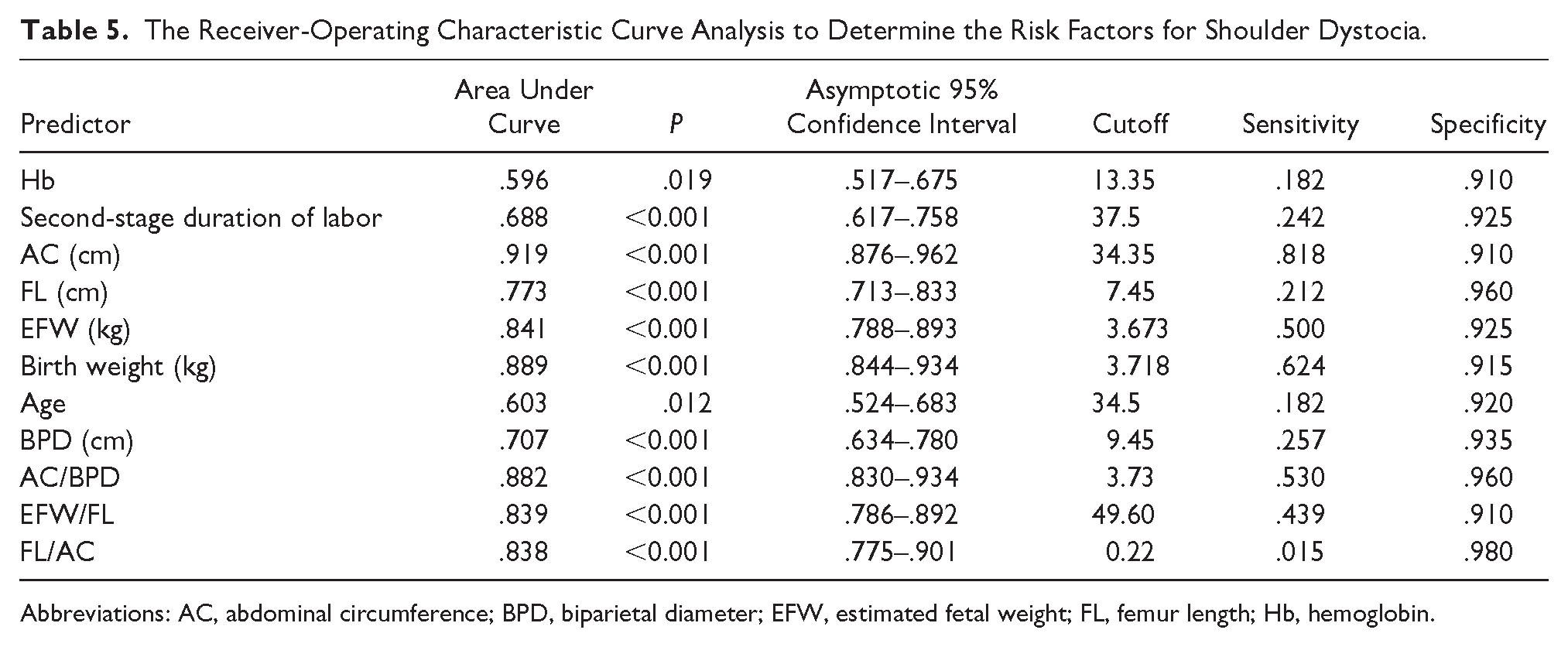
Abbreviations: AC, abdominal circumference; BPD, biparietal diameter; EFW, estimated fetal weight; FL, femur length; Hb, hemoglobin.
Discussion
SD is an obstetric emergency and one of the most important obstetric complications. It is associated with high mortality and morbidity if appropriate precautions are not taken. Despite the presence of major and minor risk factors, SD remains largely unpredictable. In the current study, based on 36 390 vaginal deliveries, over a 5-year period, the observed incidence rate of SD was 0.18%. Based on published evidence, the rate of SD was less than 0.5%, until the 20th century, however, contemporary rates range from 2% to 3%. 10 To address this increasing trend, the current study had the goal of identifying predictive risk factors, associated with SD.
Consistent with previous research, the current study findings corroborate the association between advancing maternal age and increased risk of SD (p < .05), as demonstrated by Harari et al. 11 In addition, studies by Daly et al 12 and Langer et al 13 have underscored the heightened risk of SD in women with diabetes during pregnancy (p < .001). The current study underscores these findings and reveals a significantly elevated risk of SD among pregnant women, with abnormal results on the 50 g OGTT and a diagnosis of DM (p < .001).
The various techniques used to free the fetus from the birth canal (e.g., McRoberts, Wood, Rubin, etc.), as well as episiotomy, have been suggested to prevent dystocia and reduce fetal injury. In a study, it was reported that the success rate reached 58%, when suprapubic pressure was used during the McRoberts maneuver. 14 The current study similarly found that the most commonly employed techniques used during labor were the McRoberts maneuver (54.5%) and the McRoberts maneuver combined with posterior arm rescue (21.2%). Gachon et al reported in their study that episiotomy was more frequently performed in patients who underwent maneuvers for SD (p < .05). 15 Consistent with this finding, the current study also observed a higher incidence of episiotomy in patients with SD (p < .001). It is possible to hypothesize that episiotomy facilitates the execution of maneuvers in the SD group, by creating additional space to free the trapped shoulder.
Contrary to some previous studies, Gandhi et al found that clavicle fracture did not significantly increase the risk BPI risk in neonates with SD. 16 Similarly, another study suggested that clavicle fracture alone is not sufficient to develop BPI, unless other contributing factors are present. 17 The current study also found no significant association between clavicle fractures and the development of BPI. Ancora et al showed that Apgar scores at the first and fifth minutes, and umbilical pH were lower, in patients who experienced SD. 18 In another study, the need for NICU was higher and fetal asphyxia was more frequent in the SD group. 19 Consistent with these findings, the current study revealed lower Apgar scores and a higher rate of NICU referrals in the SD group, compared with the control group.
The current study underscored the importance of maternal factors, such as advanced maternal age, maternal obesity, and diabetes during pregnancy, as significant contributors to SD risk. In addition, obstetric factors including prolonged labor duration and fetal macrosomia were identified as important risk factors. Furthermore, sonographic measurements, such as AC, FL, EFW and BW were identified as significant risk factors for SD. EFW can provide valuable information to guide appropriate precautions and minimize potential harm. Studies by Mourad et al and MacDonald et al have demonstrated a higher risk of SD in groups with elevated EFW.20,21 Consistent with these findings, the current study revealed a significantly higher EFW value in the SD group (p < .001). However, the OR value associated with EFW in the regression model was low (0.003), which may suggest a limited significant effect in terms of SD markers.
In Acker’s study, the incidence of SD was reported to be 1.1% in infants, with BW less than 4000 g, and SD was observed at 22.0% in infants, with BW greater than 4500 g. 22 In another study, Mehta et al reported that fetal macrosomia was directly related to SD. 5 In the current study, BW and macrosomia rate were significantly higher in the SD group (p < .001). In the regression analysis, BW was found to be a significant predictor (OR = 58.86, p < .001). In a study by Gilby et al, fetal AC > 38 cm and EFW were greater than 4500 g., and increased the risk for SD. 23 In a similar study, fetal AC > 36 cm was found to increase the risk for SD. 24 Sonography provides a visual of the fetal anatomy and any substantive differences, which makes it easier to predict the potential risk for SD. In the present study, sonography revealed significantly higher fetal AC values, in women who developed dystocia, compared with those without dystocia (p < .001). Fetal AC measurements emerged as a significant predictor in the regression model (OR = 48.72, p < .001). While FL values were significantly higher in the SD group (p < .001), FL was not a significant predictor in the regression analysis (OR = 0.004). Although there is no definitive evidence, on this topic in the literature, one study showed that FL had no significant effect on the prediction of SD. 25 Mehta et al reported that the duration of the second stage of labor exceeding 2 hours was directly related to SD. 5 In the current study, this duration was significantly longer in the SD group (p < .001), with each additional minute indicating an increased risk of SD (OR = 1.033, p < .05).
Surprisingly, the current study found that prepartum Hb levels were significantly higher in the SD group (p < .05) and served as a significant marker in the regression model (OR = 2.005, p < .05). This novel finding may suggest a potential positive effect of higher Hb levels on fetal weight. Maternal Hb is related to nutritional status, which influences neonatal BW. 26 Studies have shown a positive correlation between maternal Hb and BW. 27 Another study found that a significant positive correlation between maternal Hb and BW. 28 In the study of Çintesun et al, it was determined that Hb level is one of the predictors of fetal BW (β = 0.051; p = .046). 29 In the current study, the lack of statistically significant differences between pre- and postpartum Hb levels suggests that the observed differences between groups are likely attributed to prepartum Hb levels. This finding provides novel insights into the relationship between maternal Hb levels and SD risk and warrants further investigation.
The literature suggests that an AC/BPD ratio of ≥ 4 and an FL/AC ratio of ≤ 0.2 are associated with an increased risk for SD.30,31 However, in the present study, these specific cut-off values were not identified in either the case or control groups. While high AC/BPD, low FL/AC, and high EFW/FL ratios were initially identified as risk factors for SD, in the single regression model, however, it did not retain significance in the multiple regression model. The ROC analysis was the most useful predictor for SD, in this cohort, followed by values for BW, EFW, AC/BPD, EFW/FL, and FL/AC. Notably, an AC measurement greater than 34.35 cm exhibited a sensitivity of 81.8% in predicting SD, while a BW greater than 3718 g demonstrated a sensitivity of 62.4%. However, the low sensitivity of other risk factors implies that SD remains unpredictable. Therefore, the cut-off values for the AC measurement and BW may be important to make a clinical decision for the risk of SD. Likewise, the presence of other risk factors (EFW, AC/BPD, EFW/FL, and low FL/AC) should be a warning to prepare for the SD risk. Strategies, such as improved antenatal screening protocols and personalized management approaches tailored to individual risk profiles has the potential to reduce the incidence of SD and improve maternal-fetal outcomes.
Limitations
This study has important limitations based on the pre-experimental research design and the threats to internal and external validity. Although random selection was used for composing the control group, the patients enrolled in the study were a convenient set of patients. In addition, the relatively low number of SD cases recorded at the hospital, where the research was conducted, poses a challenge in extrapolating these results. The retrospective review of these maternal-fetal outcomes is also predicated on the data that were recorded on the forms and charts reviewed. The outcomes and results of this group of maternal-fetal patients are unique to them and cannot be generalized.
Conclusion
The measurement of the infant’s BW and AC emerged as the most significant risk factors for SD in this retrospective cohort study. In addition, the sonographic measurements, BPD, FL, and their ratios (AC/BPD, FL/AC, and EFW/FL), were identified as important risk factors. Higher levels of maternal Hb also contributed to the risk for SD. However, it is important to note that while these factors were significant, as they typically exhibit lower sensitivity but indicate the persistent unpredictability of SD. Therefore, health professionals should be aware of the multifactorial nature of SD risk and ensure that the necessary preparations are in place to effectively manage this obstetric complication.
Footnotes
Correction (October 2024):
Article updated to correct the p-values from .000 to < 0.001 in Tables 1, 2, and 5.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was waived by institutional committee on November 19, 2021 (13/32) because it was a retrospective study.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.