
Abstract
Objective:
This study aimed to investigate the effect of a static ultrasonographic (US) examination of the central venous structures before central venous catheterization (CVC) and the success of the procedure.
Materials and Methods:
In this prospective study, patients who underwent CVC, in an emergency department (ED), were divided into two groups: patients who underwent CVC using the anatomical landmark technique (n = 34) and patients who underwent CVC using a static US examination (n = 33). The procedure times, success rates, and number of catheters used were compared.
Results:
A total of 67 patients who underwent CVC were included in the study. Compared with the anatomical landmark technique, the static US examination had a higher procedural success rate (P = .001), fewer total interventions (P = .001), and fewer postprocedural catheter dysfunctions (P = .048). While there was no difference in the duration of the CVC between groups (P = .222), the total time spent was longer using a static US examination (P = .022).
Conclusion:
The static US examination was a practical, easy-to-apply method that could be used for CVC placement in an ED. This study demonstrated sonography had a high success rate in CVC procedures and contributed to a reduction in the number of interventions and catheters used.
Central venous catheterization (CVC), provides reliable access to the circulatory system and is an invasive procedure, used widely in various specialties, including anesthesiology, oncology, and emergency medicine. In the emergency department (ED), the main indications for CVC include fluid therapy in hypovolemia and shock, transfusion of blood and blood products, infusion of inotropic and hypertonic drugs and fluids, inability to establish vascular access through a peripheral vein, pacemaker placement, and emergency hemodialysis and apheresis procedures.1,2 Traditionally, an anatomical landmark technique and dynamic ultrasonographic (US) examination are used for CVC intervention. Procedure failure and procedure-related complications, such as pneumothorax, hemothorax, arterial puncture, subcutaneous hematoma, infection, catheter malposition, chylothorax, air embolism, and cardiac arrest, can occur during CVC intervention. For CVC procedures compared with the anatomical landmark technique, the US guidance approach is recommended due to the increased success rates and reduced frequency of mechanical complications.3–5 There are some limitations to utilizing US guidance for catheter placement and those are the need for a second provider to conduct the US, the necessity to maintain the sterilization conditions of the ultrasound equipment and transducer, prolonged procedure times, and time constraints, especially in busy ED. Therefore, CVC intervention methods, using US that are more suitable to an ED environment, and continue to be a clinical research focus. 6
In preparation for this study, a static US examination was utilized, which assists in marking the site for CVC placement, prior to the procedure. This imaging approach was planned and compared with a more traditional anatomical landmark technique for CVC insertion. This anatomical landmark technique is based on determining the best central venous vessel, prior to the procedure. This is guided by finding a vessel with the widest lumen diameter, lack of thrombus, a normal relationship with the adjacent artery, and anatomical variations that will not complicate the procedure. 5 The advantage of the static US examination, unlike the dynamic US-guided method, is that it requires less preparation prior to the procedure, does not require a sterile technique, and can be performed by a single provider, without assistance (See Table 1).
A Comparison Is Provided of the Three Types of Examinations That Could be Used to Prepare for a Central Venous Catheter Placement (CVC).
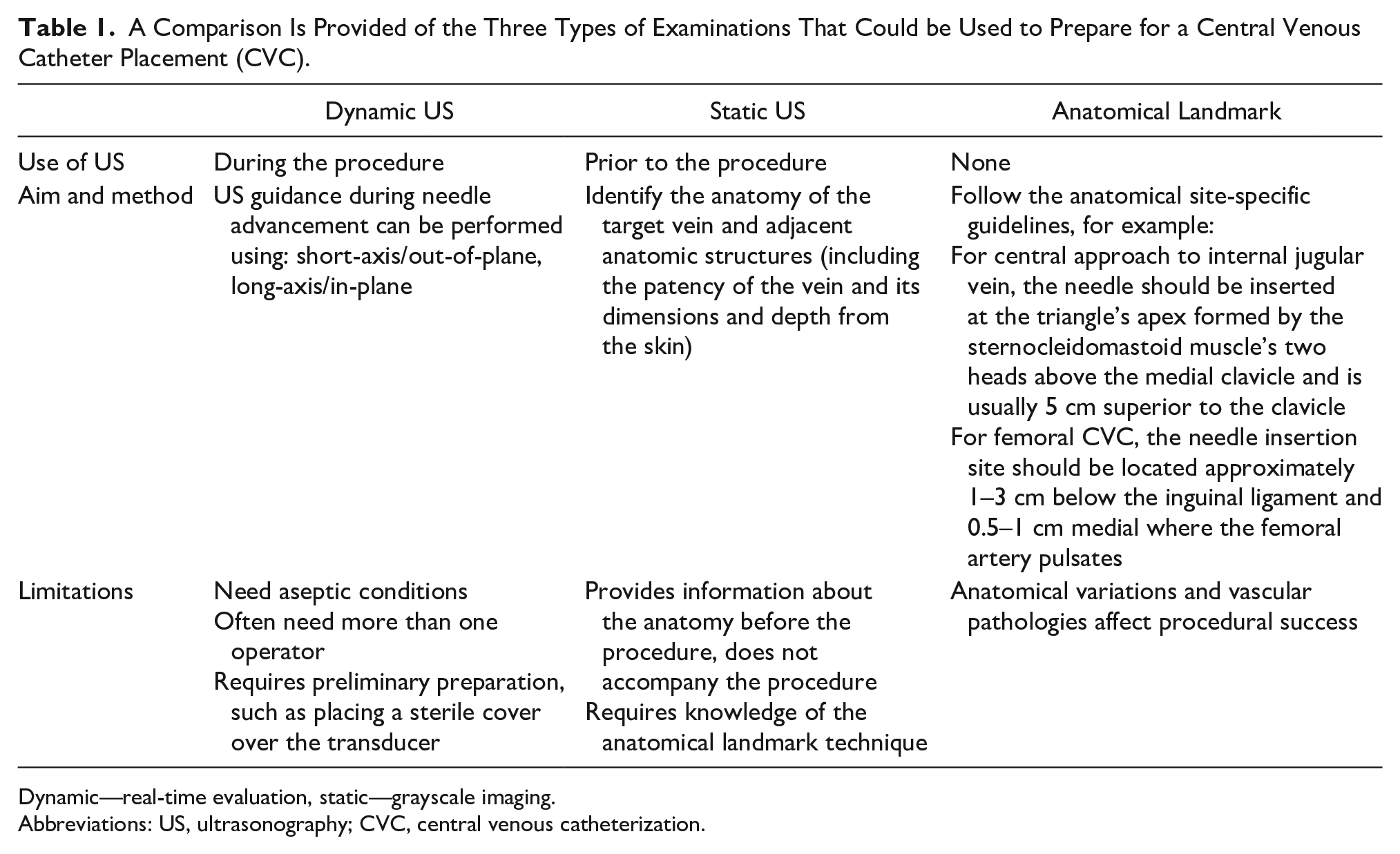
Dynamic—real-time evaluation, static—grayscale imaging.
Abbreviations: US, ultrasonography; CVC, central venous catheterization.
The aim of the proposed study was to compare the static US examination and the anatomical landmark technique in terms of procedural success, completion time, number of attempts/trials, and complications.
Materials and Methods
This cross-sectional, prospective clinical trial was initiated after approval from the local university ethics committee (IRB# 2019-85-41). The study consented 67 adult patients who underwent CVC insertion, in the ED, between January 1, 2019, and January 31, 2020.
The patients were divided into two groups: those who had the static US examination for CVC placement and those who received the anatomical landmark technique. Patients who had a static US examination, were completed with a Sonosite FC1 (Fujifilm. Lexington, MA) and a 13-6 MHz linear transducer, which was used by a senior emergency medicine resident and researcher. The provider was certified in advanced sonography training, had sufficient sonography experience, and had been trained in the evaluation of venous structures, as well as the detection of anatomically different, occluded, or problematic venous structures. Both the femoral and jugular veins were examined using the static US examination and the problematic vein as well as the site of intervention were determined (See Figure 1). The anatomical landmark technique was used for the group of patients where the site of intervention was determined by using the patient’s anatomy without preprocedural dynamic US, prior to CVC placement. Both patient groups had CVC interventions performed on by experienced senior emergency medicine residents, who were adequately trained in performing this intervention.
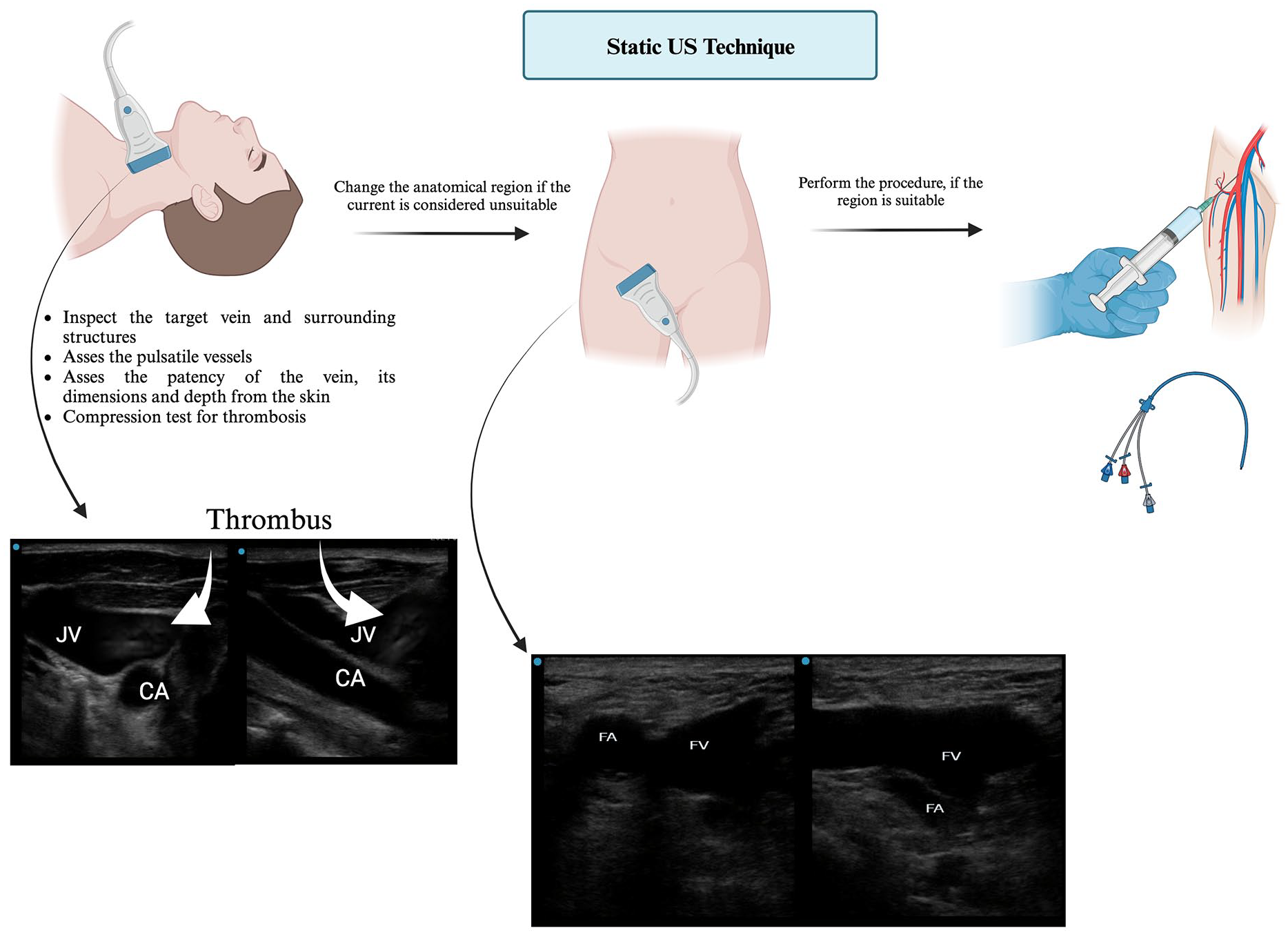
A pictorial display of how the static ultrasonography examination was used, as part of the central venous catheterization procedure. The graphic was created with biorender.com.
The demographic characteristics of the patients, indications for CVC, complications that occurred during and after the procedure, number of interventions, the success rate of intervention, vascular pathologies, diameters and lumen lengths of vascular structures, and procedure times were all recorded. The procedure times, the total time spent for the CVC, (in minutes) and the time spent during the CVC procedure (in minutes) were all recorded. The total time spent on a CVC procedure (in minutes) was determined by the moment the transducer first touched the body. Likewise for the alternative method, total time began, the moment the intervention site was determined using anatomical landmarks. The exam time was concluded when the procedure was deemed successful and this was gauged by sampling blood from the inserted catheter and/or infusing fluids through the catheter, as this verified vascular access. The time elapsed, during the CVC procedure (a successful CVC procedure time allotment) was determined from the moment the first needle entered the site until the first blood sample was flowing from the catheter. The catheterization success rate was obtained by dividing the number of successful catheter applications by the total number of trials and multiplying by 100. Patients over the age of 18 who were CVC candidates were enrolled only if they had given written consent to participate in the study. The subclavian vein has specific challenges as a conduit for this procedure, due to its small diameter, deep location, a higher relative risk of pneumothorax, less accessibility to US, and existing in a non-compressible location. In addition, the staff at the research site (e.g., emergency medicine, cardiovascular surgery, and nephrology) did not prefer to use the subclavian vein for CVC, except in renal failure patients where subclavian catheter complications may preclude potential future arteriovenous (AV) fistula. Therefore, patients who had undergone subclavian catheterization were excluded from the study.
Data Analysis
A power analysis was informed by the work of Airapetian et al, 7 therefore, it was determined that each group needed 26 patients to achieve a statistical power of 95% and a P value of .05. The plan was to enroll a total of 52 patients to reach the 95% statistical power. The study was successful in recruiting 67 total patients and was terminated at the end of the first year.
The collected data were analyzed using SPSS for Windows 21.0 (SPSS Inc., Chicago, IL). The distribution of data was checked for normality using the Kolmogorov-Smirnov and Shapiro-Wilk tests. In the comparison of paired groups of continuous variables, the Student t test was used for paired groups and confirmed normal data distribution. The Mann-Whitney U test was used for paired groups, but it demonstrated a nonnormal data distribution. The chi-square test and Fisher’s exact test were used for categorical data comparison. Descriptive statistics were presented as mean (±) standard deviation, median (minimum-maximum), frequency distribution, and percentage. Absolute risk reduction (ARR) was calculated as the net difference between the rate of development of catheter dysfunction, after the procedure (Experimental Event Rate = EER). In the static US examination group, the rate of development of catheter dysfunction after the procedure (Control Event Rate = CER), as well as those in the anatomical landmark technique group. The number needed to treat (Number Needed to Treat = NNR) was calculated as 1/ARR.
Results
A total of 67 patients completed the full study. The mean age of all patients was 52.3 ± 16.7 years and 73.1% of the patients were men. No significant differences were found between the patient groups regarding age, gender, Glasgow Coma Scale score, intubation rate, accompanying chronic diseases, and indications of CVC. The most common indication for CVC in both groups was hemodialysis planning due to intoxication (48.5% and 64.7%). The most commonly used vein in both groups was the right femoral vein (63.6% and 76.5%). Table 2 summarizes the comparison of sociodemographic and clinical data between the patient groups.
A Comparison of the Study Cohort’s Sociodemographic and Clinical Data, Which Were Variables in the Study.
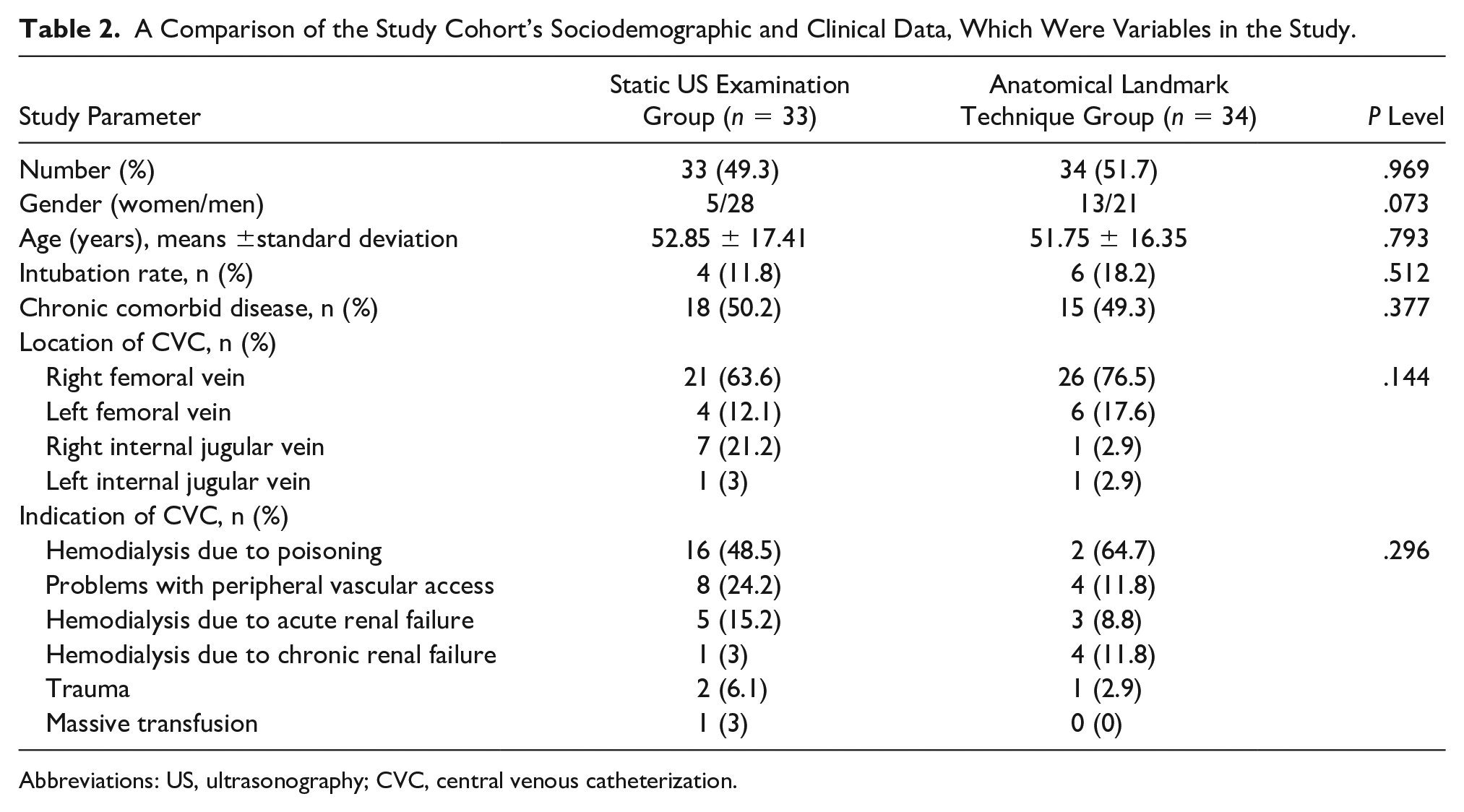
Abbreviations: US, ultrasonography; CVC, central venous catheterization.
Catheter dysfunction was found to be higher in the anatomical landmark technique group (P = .048), and the procedure success rate was significantly higher in the static US examination group (P = .001), and the total number of attempts for successful CVC was significantly lower (P = .001). The total time spent during CVC was significantly lower in the anatomical landmark technique group (P = .022). Six (8.9%) of the patients included in the study had mechanical complications related to CVC. In the static US examination group, the complication rate was 9.1% and these complications were thrombosis (n = 1), hemorrhage (n = 1), and AV fistula (n = 1). In the anatomical landmark technique group, the complication rate was 8.8% and these complications were as follows: pneumothorax (n = 2) and guidewire entrapment in the lumen (n = 1). There was no significant difference between the two groups in terms of complication rates (P = .649). For catheter dysfunction after CVC (3.0% and 20.6%), the ratio of number needed to treat/number needed to harm (NNT/NNH) was calculated as 5.7. For the CVC intervention success rate (90.9% and 64.2%), the NNT/NNH ratio was calculated as 3.7. The comparison of the procedure success criteria in the patient groups included in the study is given in Table 3.
A Comparison of the CVC Procedure Success Criteria, Within the Patient Groups, Included in the Study.
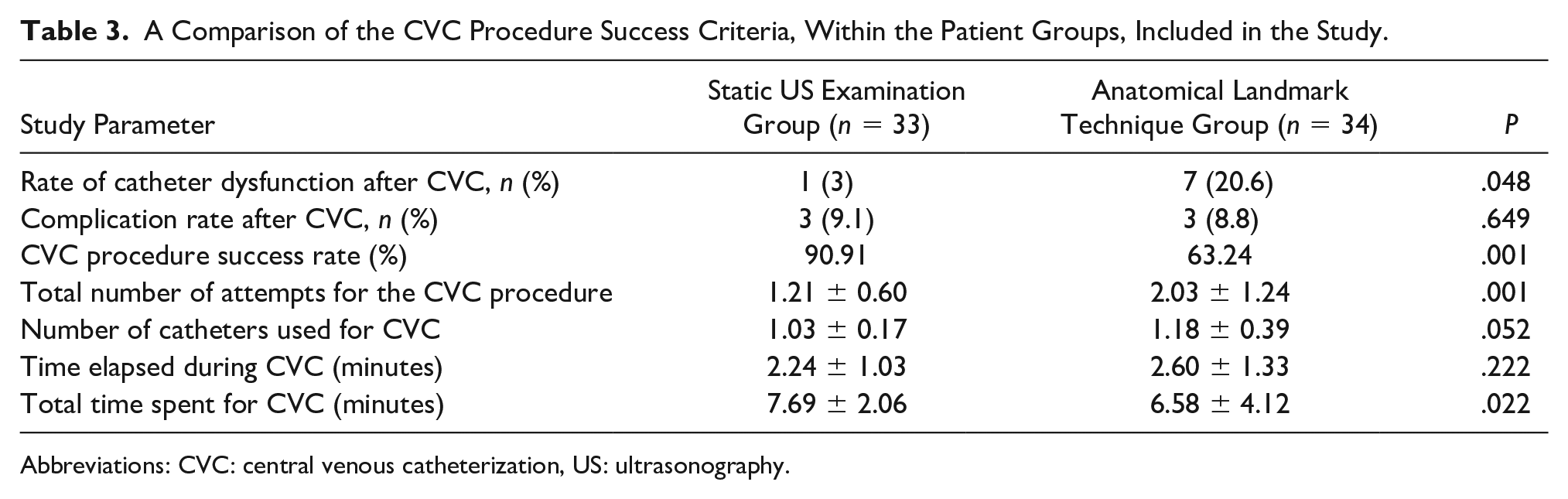
Abbreviations: CVC: central venous catheterization, US: ultrasonography.
Discussion
In this cohort of patients, utilizing CVC after identifying the most appropriate vessel with US, significantly enhanced the success rate, reduced the catheter dysfunction rate, and lowered the total number of interventions.
In CVC, correct indication and procedural success are the key indications of success. Increased procedural success rates increases patient comfort, decreases patient complications, reduces catheters used, which makes the procedure effective and a cost savings. The US-guided CVC technique is currently the most recommended technique in the literature to increase the success rate of CVC interventions. 5 The use of US guidance for CVC placement has been described for many years. In the first studies, it was found that the use of US significantly increased the success rate of the procedure compared with those performed without US. In one of the first studies, Legler et al 8 reported that the success rate of internal jugular cannulation without Doppler was at a rate of 28.6%, while the success rate of cannulation with Doppler was 77.3%. In the following years, Denys et al 9 in a study comparing internal jugular vein cannulation in 302 patients using the external landmark technique and in 928 patients using US guidance. Their success rates were 38.4% and 78% at first attempt, respectively. In a prospective randomized controlled study of 115 patients, Armstrong et al 10 found that the rates of successful internal jugular vein cannulation, at first attempt for CVC, were 52.6% in the group using the anatomical landmark technique and 75.6% in the group using the US guidance.
Regarding the use of US guidance during CVC placement, in the femoral vein, Brass et al 11 found that the success rate was 89% but only 78.9% with the anatomical landmark technique. In the same study, the CVC success rate at first attempt was 85% for US guidance compared with 48.7% for using the anatomical landmark technique. In the present study, the success rate at first attempt in CVC performed using the static US examination was 90.91% compared with 63.24% for the anatomical landmark technique.
After the widespread use of central venous catheters, catheter-related dysfunction, and complications have also increased. Complications can be listed as artery puncture (carotid, subclavian, femoral artery), hematoma, hemothorax, chylothorax, pneumothorax, nerve damage (brachial plexus, stellar ganglion), and embolism due to cannulation; cardiac perforation, arrhythmias, and heart blocks due to catheter placement; thrombosis, thromboembolism, infection, and arrhythmia due to the presence of the catheter.12,13 Complication rates differ in many studies. Eisen et al 14 reported a mechanical complication rate of 39% for subclavian lines, 33% for internal jugular lines, and 24% for femoral lines, in a prospective study of 385 consecutive CVC attempts. However, failed attempts were also included as complications in that study. Steele et al 15 reported a complication rate of 4.2% for subclavian lines, 5.3% for internal jugular lines, and 0% for femoral lines in a retrospective study, including 643 central catheters, placed in the ED. With the use of US guidance in catheter placement procedures, a decrease in mechanical complications has been reported. For example, Denys et al 9 reported that carotid artery injury was 8.3% when the anatomical landmark technique was used in internal jugular vein catheter placement, while the placement of a CVC, with US guidance, had an injury rate of only 1.7%. Similarly, they reported injury rate, to the brachial plexus of 1.7% with anatomical landmarks compared with 0.4% with US guidance and hematoma development was 3.3% and 0.2%, respectively. In the current study, while the CVC complication rate was 8.8%, when using the anatomical landmark technique, this rate was found to be 9.1%, employing the static US examination. There was no statistically significant difference in complication rates within both patient groups. However, the rate of catheter dysfunction, after CVC, was 20.6% using the anatomical landmark technique and 3.0% with the static US examination. As noted, the catheter dysfunction was significantly reduced when utilizing the static US examination. Although these complication rates are relatively low, CVCs can have serious complications. Bagwell et al 16 reviewed a group of 75 patients and found the mortality rate 33% in 33 patients with serious complications, and fatal complications attributed to pneumothorax, hydrothorax, hemothorax, and cardiac tamponade. In the current study, pneumothorax developed in two patients during CVC, and these patients were diagnosed and treated early. There were no fatalities due to these complications.
In published studies Troianos et al 17 and Slama et al 18 study patients underwent US-guided CVC in less than 3 minutes (180 seconds). In another study by Miller et al, 19 CVC was performed in an average of 116 seconds with US. These procedural times were calculated from the moment that the needle touched the skin until the first aspiration of blood was drawn from the catheter. The preparation time for initiating the ultrasound equipment system and locating the vascular structures was not included in their tally. Although other studies in the literature have shown that US guidance decreases the duration of CVC, these studies did not allot for the time to preparation of the ultrasound equipment system, applying sterile technique, and overall procedural preparation. In the current study, although the duration of CVC was shorter for the patients undergoing a static US examination, there was no statistically significant difference in the duration of CVC between the patient groups.
In the current study, the total time spent for CVC was recorded by calculating the time lost between the preparation of the ultrasound equipment system, locating vascular structures, finding vascular structures by anatomical landmarks, unsuccessful procedural attempts, and any change in provider. When the total times were compared between the groups, in current study, this time was found to be significantly shorter in the anatomical landmark technique group. The reason for increased procedural time was attributed to the static US examination of four central veins, which was included in the total time allotment, in that patient group. However, when reviewing the rates of catheter dysfunction, procedural success, and the number of procedural attempts, a few added minutes of procedure time, due to use of static US, may have minimized the rates of fail attempts and patient injury.
Limitations
The major limitation of this study is the preexperimental design, which has threats to internal and external validity. In addition, this was a convenient sample of patients that qualified for a CVC procedure. It is also important to point out that this study excluded subclavian venous catheterization and an assessment as to that approaches potential advantages or disadvantages. This limitation restricts the ability to fully generalize as to the practical effectiveness and reliability of subclavian venous catheterization.
Another limitation was that this study was executed in a single center with multiple providers conducting catheterization, as well as a single provider completing the static US examination. These personnel assignment may have affected procedure success. The patients consented composed a small cohort and may be unique to the host university’s ED.
Conclusion
This study demonstrated, in this cohort of patients, a static US examination shortened CVC procedural time, when conducted in the ED. In this cohort of patients, there was increased procedural success and decreased catheter dysfunction. The fact that this procedure can be performed by a single provider and does not require sterilization and preliminary preparation, may increase its applicability in the ED. In addition, the low-cost and widespread availability of US further enhances its potential in the ED. This procedural set-up is worth considering given the patient comorbidities and those with vascular compromise, which could expedite care in the ED.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from the local university ethics committee (IRB# 2019-85-41).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.