
Abstract
This case report provides a review of the occurrence, variations, signs/symptoms, and gender/side preferences of an absent common carotid artery (CCA) anatomical variant. Normal embryology of the carotid arteries and associated structures are also discussed. The relationship between absent common carotid bifurcations and the risk for plaque development is also considered but is limited due to the lack of empirical evidence. This report also outlines and demonstrates an absent right CCA with direct, separate origins of the right external carotid artery and right internal carotid artery from the right subclavian artery. An absent CCA is a rare vascular anomaly with multiple variations. There are typically no associated signs/symptoms, and there are no gender or side preferences.
The absence of a common carotid artery (CCA) is a rare, congenital anatomical variant. There are multiple different anatomical variations that can be associated with an absent CCA. As outlined in literature, one individual may have an absence of their right CCA with a common origin of the innominate artery and left CCA. 1 Another variant involves a bilateral absence of the carotid arteries, although there have only been 2 reported cases on bilateral absence of the carotid arteries in literature. 2 Regardless of the variations associated with an absent CCA, there are fewer than 50 reports of individuals with a congenital absence of one or both of their common carotid arteries. 3 A majority of patients with an anomalous absence of a CCA are asymptomatic and most cases of an absent CCA are found incidentally. 1 Of the reported cases, there have been no significant gender or side preferences determined. 4
Case Report
A 59-year-old African American male presented to the sonography department for a carotid sonogram, status-post a 10-second episode of slurred speech, which may have been related to a transient ischemic attack (TIA). The patient had a reported history of hyperlipidemia. The purpose of the carotid sonogram was to evaluate the carotid arteries for a possible stenosis.
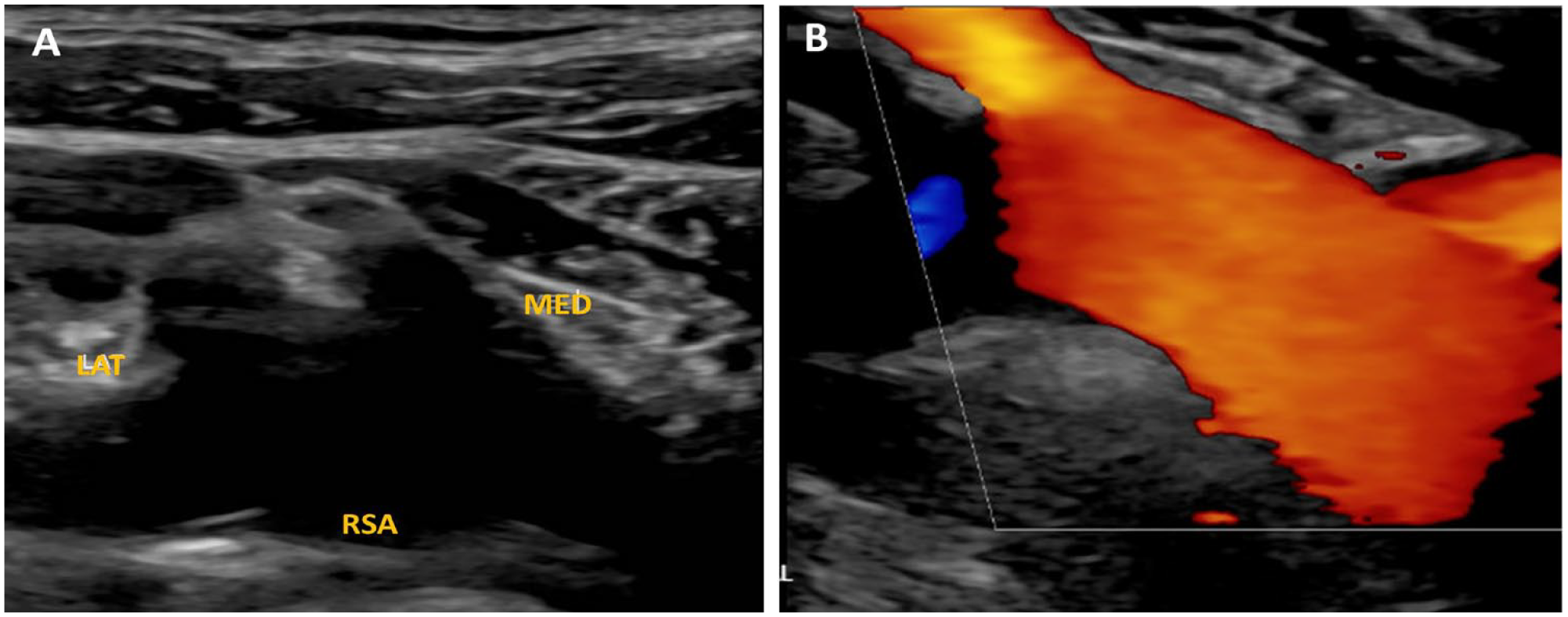
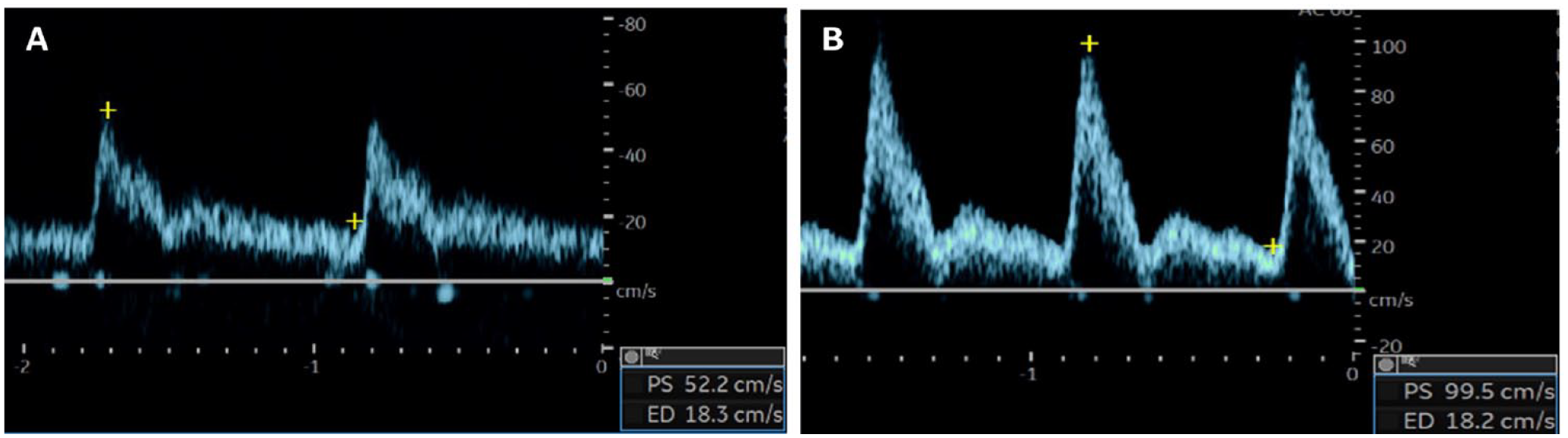
A Logic E10 (GE Healthcare, Waukesha, WI) ultrasound equipment system, equipped with a linear array transducer and center frequency of 9 MHz, was used to conduct an evaluation of the carotid arteries. Upon evaluating the carotid arteries, the right CCA appeared to be absent. Instead, there were two arteries that arose from the right subclavian artery near one another, but with separate vascular origins (Figure 1). One of the arteries arose from the right subclavian artery proximally (medially), and the other artery arose from the right subclavian artery distally (laterally). These arteries coursed superiorly and remained separate as they ascended. Color and pulsed wave Doppler were used to interrogate the arteries. When evaluating the spectral waveform of the distal vessel, this waveform appeared to have monophasic, low resistive characteristics, with a peak systolic velocity (PSV) of 52.2 cm/sec and an end diastolic velocity (EDV) of 18.3 cm/sec (Figure 2A). This vessel had a resistive index (RI) of 0.6. The spectral waveform of the proximal vessel appeared to be monophasic and have higher resistive characteristics, with a PSV of 99.5 cm/sec and an EDV of 18.2 cm/sec (See Figure 2B). The RI of this vessel was 0.8. There were no branches from either vessel observed extracranially. Given the waveform characteristics alone, it appeared that the proximal vessel was likely the external carotid artery (ECA), and the distal vessel the internal carotid artery (ICA). To prove this theory, a temporal tap (TT) was applied to the superficial temporal artery upon spectral Doppler evaluation of the proximal vessel. There was a diastolic variation in the waveform as the TT was applied (See Figure 3). This confirmed that the proximal vessel was the ECA supplying the patient’s facial structures, and the distal vessel was the ICA (See Figure 4).
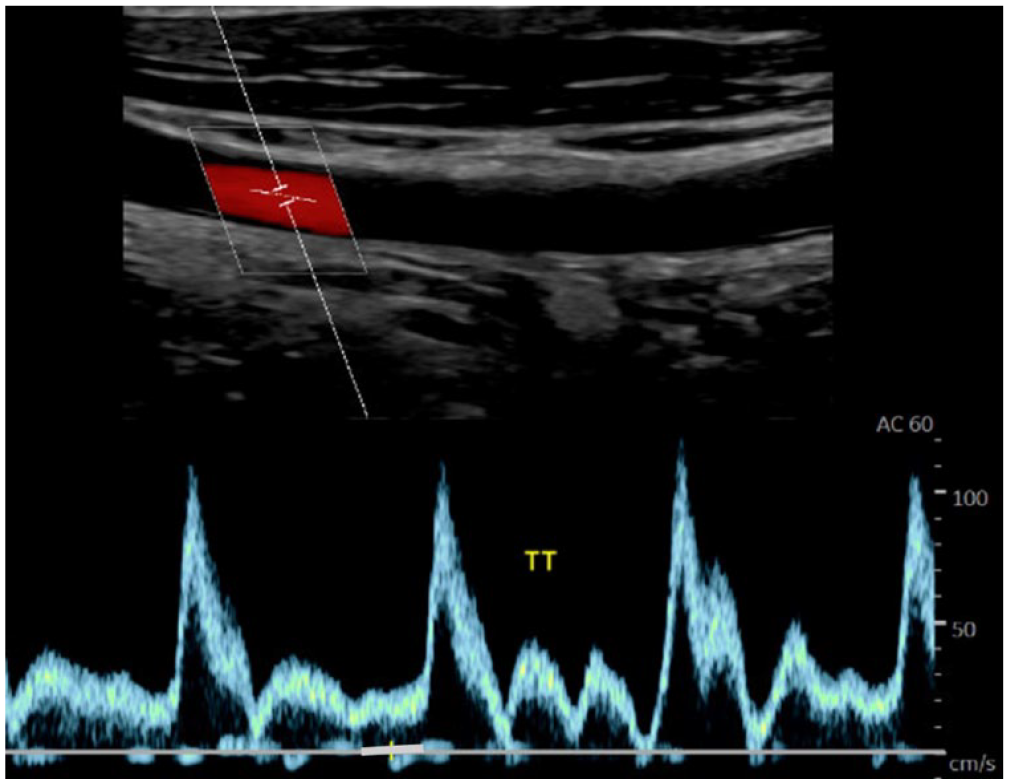
A triplex sonographic image taken at the mid ECA and a resulting spectral Doppler waveform that demonstrated the temporal tap (TT) observed in diastole.
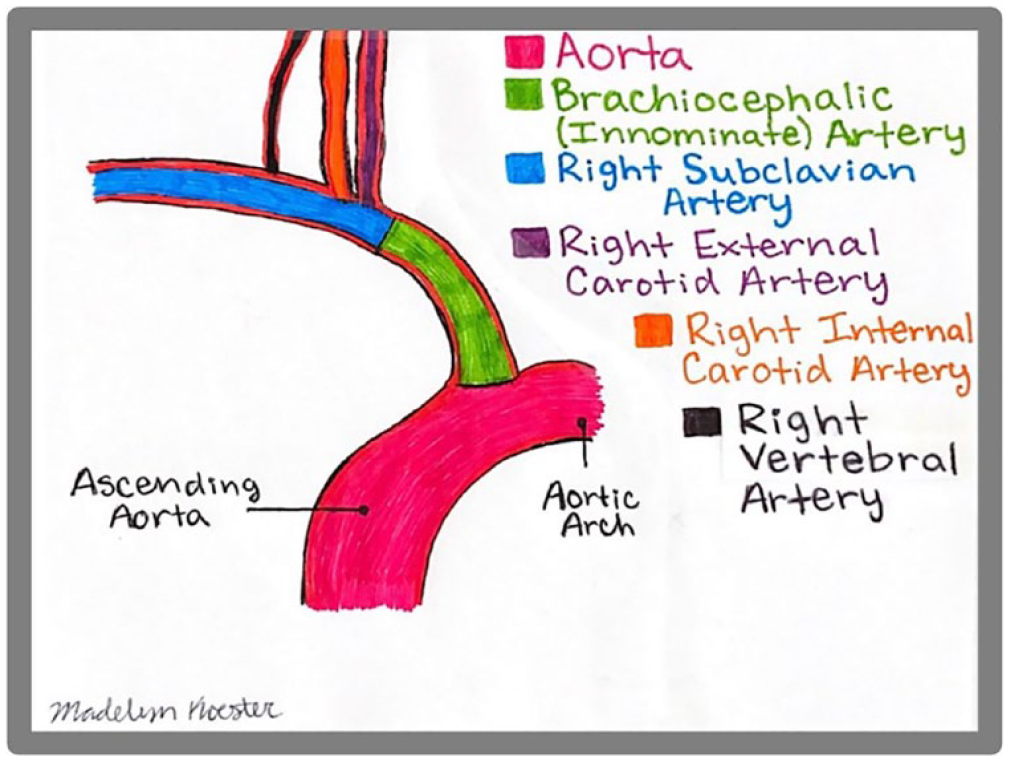
Diagram is provided to illustrate the right ECA and right ICA originating from the right subclavian artery. The ECA has a more proximal origin and the ICA a more distal origin from the subclavian artery.
There was no evidence of atherosclerotic plaque within the observed portions of the right ICA and the right ECA. Following the examination on the right, the left carotid system was sonographically evaluated. The patient’s left side had a CCA that bifurcated into the ECA and ICA, representing typical anatomy. The left carotid system demonstrated atherosclerotic plaque scattered throughout. In addition, bilateral vertebral arteries were imaged with normal, antegrade flow.
The radiologist report confirmed that there was variant right carotid system anatomy with separate, direct origins of the ECA and ICA from the subclavian artery. There was no bilateral hemodynamically significant stenosis observed at that time, but there was minimal scattered atherosclerotic plaque throughout the left carotid system. The radiologist report also recommended that a computed tomographic angiogram (CTA) be completed. The CTA was recommended as a means of further evaluation and to confirm the anatomical variant. At the time of this report, the patient has not completed the CTA.
Discussion
Embryology
During embryologic development, the cardiovascular organs begin to develop as early as the third week of gestation. 5 Any deviation from normal development can lead to an anomalous orientation of anatomy. The occurrence of congenital anatomical variations is directly related to the biological processes that occur during development. The cause of anatomical variations may be due to genetic or environmental factors, or the combination of both. 6 Although anatomical variations are a deviation from what is considered normal anatomy, these variations typically do not affect physiological functions. In the case of an absent CCA specifically, the anomalous orientation usually does not result in any associated signs or symptoms. 1
Case Study Compared to Those Reported in the Literature
There are various anatomical variations that can occur in conjunction with bilateral or unilateral CCA absence. In the greatest number of right CCA aplasia cases, the ECA typically arises from the innominate artery and the ICA arises from the right subclavian artery, or they both originate from the innominate artery. 6 There have been no reports in literature of the ECA and ICA both originating from the right subclavian artery when there is an absence of the right CCA. In this case study, the ECA originated more proximally, and the ICA originated more distally, which corresponds to findings reported in other case studies. Compared to cases that have been reported in the literature, which included multimodality imaging, this case is unique in that the diagnosis was only based on the sonogram and in large part due to the patient not completing the recommended CTA.
Plaque Formation and the Absence of Normal Vessel Bifurcations
With regard to atherosclerotic plaque, the carotid bifurcation is one of the most common pathologic sites. 7 Plaque formation can cause the vessel lumen to become narrowed, and narrowing can lead to stroke, or even death. 7 The carotid bifurcation is one of the most common sites for the development of atherosclerotic plaque due to shear stress decrease and resultant flow recirculation and stagnation. 8 Arterial wall shear stress is directly affected by blood flow velocity, viscosity, and arterial radius. 8 At the carotid bifurcation: velocity and arterial radius decrease, resulting in shear stress decrease. With low shear stress, vascular endothelial permeability increases and infiltration of monocytes into the arterial wall leads to the migration of smooth muscle cells into the subintimal layer, which induces local atherosclerosis. 8 As demonstrated in this case study, the patient had an anomalous orientation of their right carotid system, resulting in an absence of a normal right carotid bifurcation. The patient’s left carotid vascular system had a normal carotid bifurcation. The patient had no atherosclerotic plaque in his right carotid system, but the patient’s anatomically normal left carotid system demonstrated scattered atherosclerotic plaque. In some but not all reported cases of absent CCA, there have been documented atherosclerotic plaque found in the ICA and/or the ECA, on the affected side. In cases with these CCA anomalies, the relationship between the absence of a bifurcation and the prevalence of plaque development, deserves further study. Does the lack of a carotid bulb and bifurcation decrease the risk for development of atherosclerotic plaque in these patients? This diagnostic concern has not been studied, and due to the small number of cases reported, this remains a mystery.
Conclusion
The absence of a CCA is a rare, but an interesting anomaly. Positive, confirmed cases of an absent CCA are usually found incidentally. Patients commonly do not have associated signs or symptoms, and there are currently no gender or side preferences. This case report outlined a patient with an absent right CCA with the right ECA and right ICA with direct, separate origins from the right subclavian artery. In addition, the patient had a normal left carotid vascular system. Although confirmed risks have not been associated with an absent CCA, likely due to a lack of evidence, it is still important to consider the relationship between absent common carotid bifurcations and the risk for developing atherosclerotic plaque.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because the case study pertained to required coursework at the University of Kansas Medical Center and contained no identifying materials or information.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).