
Abstract
Point-of-care ultrasonography (POCUS) is a key tool in critical care, including obstetric patients in intensive care units (ICUs). Point-of-care ultrasonography can aid in pregnancy diagnosis, fetal assessment, and detection of complications. This case study is based on a 39-year-old pregnant woman, admitted to critical care for preeclampsia. After cesarean delivery, the patient experienced decreased hematocrit levels, renal dysfunction, and uterine tenderness. The POCUS demonstrated uterine atony (inability of the uterus to contract after childbirth), leading to exploratory surgery that confirmed a Couvelaire uterus (CU). Hysterectomy was performed, and histology showed necrosis and bleeding. Couvelaire uterus is a rare complication of placental abruption, caused by placental vascular damage and uterine bleeding. Conservative management and uterine contraction-stimulating drugs are typically used to treat CU. In this case, POCUS provided real-time data for the diagnosis of this obstetric emergency and perhaps other conditions. This report underscores the significance of surveillance and prompt intervention to prevent adverse outcomes for both mothers and infants.
In recent years, ultrasonography has become one of the most widely accepted devices by health care professionals in the field of critical care.1,2 The utility of this method also extends to patients admitted to the intensive care unit (ICU) due to obstetric pathologies, 3 allowing for the diagnosis of pregnancy during focused assessment with sonography in trauma and the assessment of fetal vitality and viability.4,5 Point-of-care ultrasonography (POCUS) is a real-time bedside sonographic evaluation used to quickly diagnose and treat patients. It is an extension of the physical examination and a supplementary diagnostic tool for physicians. Unlike a traditional sonogram, POCUS is a fast, focused examination that can reach a diagnostic or therapeutic goal. Recently, POCUS has been applied in obstetric critical care. It can also be used to rule out the presence of ectopic pregnancy or free fluid in the Douglas pouch, proving to be highly valuable in the evaluation of pregnant or postpartum patients with hemodynamic instability.2,6 This case report is centered on the use of POCUS and how this led to the diagnosis of Couvelaire uterus (CU).
Case Report
A 39-year-old woman, with a medical history of obesity, left adnexal simple cyst, gestational diabetes, and 36 weeks pregnant, was admitted to the emergency department with preeclampsia. An urgent surgical approach was deemed necessary, leading to a cesarean (C) section in conjunction with left adnexectomy and right tubal ligation.
The patient was admitted to the ICU in the immediate postoperative period for surveillance and was alert and afebrile, with a heart rate of 70/bpm, blood pressure of 100/70 mm Hg, respiratory rate of 12/min, and hemoglobin level of 12.3 g/100 mL. The total leukocyte and platelet count, as well as liver function and coagulation test results, were within the normal range.
During the early stages of her hospitalization, the patient presented with a decrease in urinary output, experienced an increase in blood creatinine levels from 0.7 to 1.2 mg/dL, along with a 15-point reduction in hematocrit (from 12.30 to 7.3 g/100 mL), without any genital bleeding. Furthermore, the patient presented with increased tenderness of the hypogastric region.
Point-of-care ultrasonography was performed in grayscale with both longitudinal and transverse views, which revealed the presence of a heterogeneous lesion with areas of different echogenicity in the uterine parenchyma, along with a small fluid collection in the Douglas pouch (See Figure 1), highly suggestive of uterine atony. After this finding, as no pharmacological response was observed with a 20 IU continuous oxytocin infusion over 24 h, an exploratory laparotomy was conducted. During the procedure, the uterus displayed a dark, purplish mottled appearance, leading to an intraoperative diagnosis of CU (See Figure 2). Subsequently, hysterectomy was performed, and the collected sample underwent pathological examination.
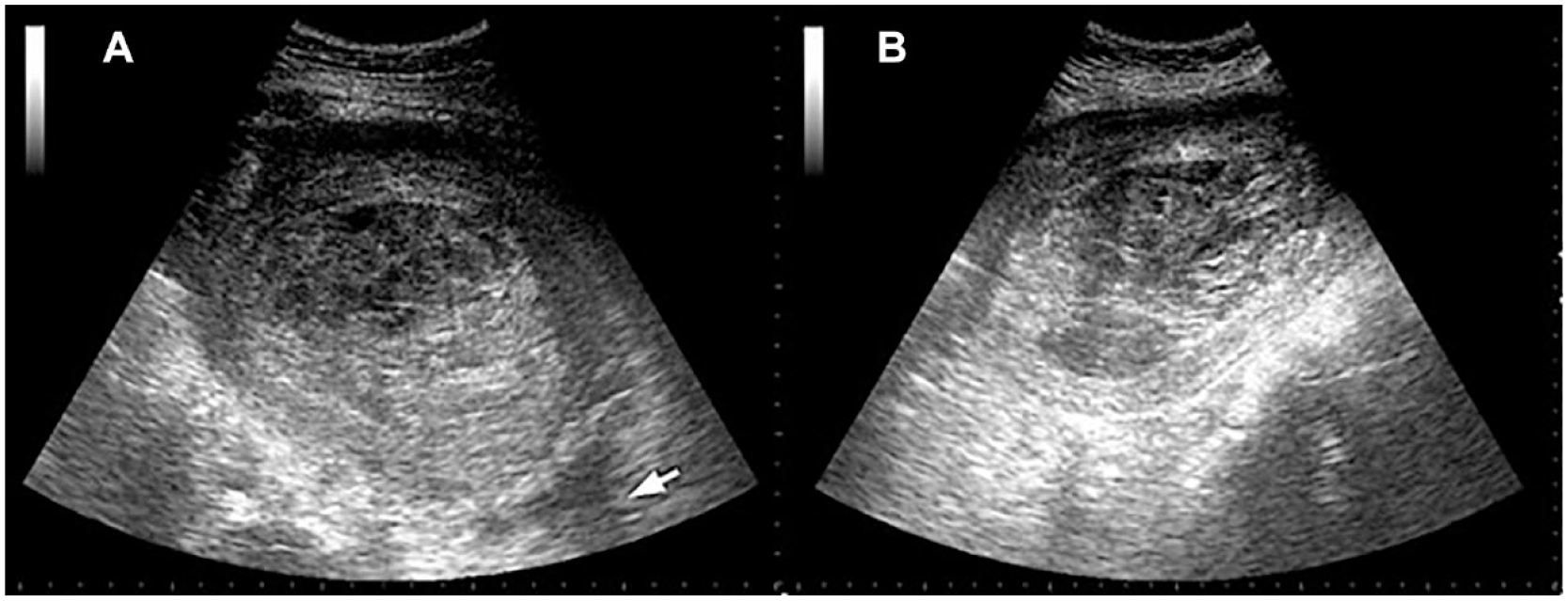
Sonographic transverse (A) and longitudinal (B) views are provided of an enlarged uterus with the urinary bladder not visible. Inside, areas with different echogenicity and fluid collection in the Douglas pouch (arrow). The placenta is not observed inside the uterus, because the point-of-care ultrasonography (POCUS) was performed post-Cesarean section.

An image is provided of the surgical sample extracted. The uterus has a dark purplish mottled appearance due to blood extravasation in the myometrium.
In the pathological analysis of the samples (See Figure 3), necrotic regions affecting the perimetrium and infiltrating the myometrium were observed in both specimens. In addition, extensive areas of isolated myometrial necrosis were observed, and the cervix displayed near-complete necrosis. In the histological sections of the uterus, areas of significant hemorrhage, necrosis, and polymorphonuclear infiltration were evident, primarily affecting the outer third of the myometrium and extending to the serosa. Significant hemorrhage was also observed in the cervix and adnexa, with these muscular fibers being devitalized and with a marked compromise in functional capacity (See Figure 4). Four days later, the patient was discharged from the ICU to continue her recovery in the general medical ward.

Macroscopic samples are provided that demonstrate extensive areas of necrosis surrounding the perimetrium and invading the myometrium, isolated areas of necrosis in the myometrium, and significant necrosis in the cervix.
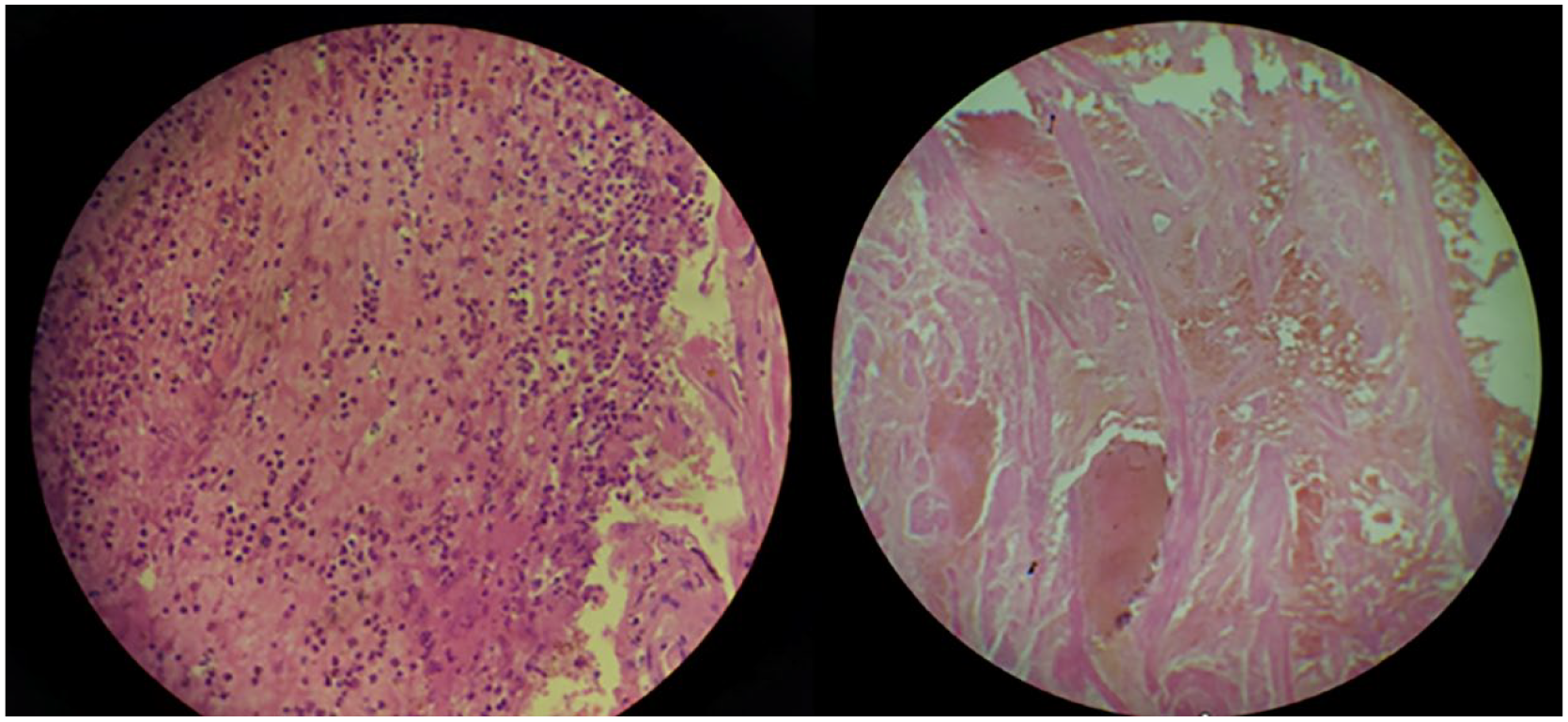
Images of the microscope images demonstrate erythrocyte infiltration in the myometrium. It is also important to note devitalized of the muscle fibers.
Discussion
Couvelaire uterus, also referred to as uteroplacental apoplexy, is a rare phenomenon occurring in approximately 5% of cases involving placental abruption.7 –11 This condition, initially described by the French obstetrician Alexandre Couvelaire in 1911, occurs when vascularization of the placenta sustains damage, leading to hemorrhage that separates the basal decidua from the placenta and penetrates deep into the uterine musculature. 12 In some instances, it may extend further to involve the uterine serosa, parametrium,8 –10,13 –15 and, on rare occasions, reach the peritoneal cavity.8,9,11
Consequently, macroscopic manifestations of CU become evident, characterized by ecchymosis, presenting a spectrum of colors ranging from violet to black.8 –15 Uterine contractility is often preserved, especially after amniotomy and decompression, to facilitate constriction of spiral arteries.8,12,13 Couvelaire uterus may experience a decline in contractile function; however, it typically exhibits spontaneous resolution or responds well to intravenous oxytocin treatment.8,10,15,16 Importantly, CU diagnosis should not automatically lead to a recommendation for hysterectomy, and such an approach should be discouraged.8 –10,12
The standard course of action is conservative management unless specific conditions arise, such as the loss of uterine contractility, unresponsiveness to oxytocin or other uterine contraction-inducing medications, emergence of an acute abdominal condition, or the presence of coagulopathy in the patient.12,15 Couvelaire uterus is often under-diagnosed and under-reported. Although the precise cause remains largely unknown, it has been linked to various factors, including placental abruption, placenta previa, amniotic fluid embolism, preeclampsia, coagulopathy, and uterine rupture resulting from a transverse fetal presentation.8,16
Point-of-care ultrasonography provides real-time information crucial for monitoring and diagnosing a broad spectrum of medical conditions. A growing body of evidence highlights the positive outcomes associated with the integration of POCUS into medical education at various levels. This accumulating evidence suggests the potential for POCUS to evolve into an indispensable tool for health care professionals. 17 The quality of POCUS assessments is highly dependent on operator competence, emphasizing the importance of enhancing education and training in this area. 3 Numerous case reports, in the field of obstetrics, have highlighted the effectiveness of POCUS in the diagnosis and assessment of pregnancy-related complications. These include situations involving maternal abdominal hemorrhage in the case of uterine rupture. 2 Furthermore, research has shown that transabdominal sonography can play a crucial role in revealing retroplacental hemorrhage, even in the absence of vaginal bleeding, but when accompanied by fetal bradycardia. This allows physicians to make urgent decisions, such as the option to terminate pregnancy, performing C section, to reduce the risk of intrauterine fetal death or hypoxic brain injury resulting from delayed diagnosis. 18
In these situations, it is crucial to be vigilant for placental abruption, even in the absence of vaginal bleeding or if the ultrasound does not show recent detachments. Failing to diagnose it promptly can greatly increase the chances of fetal death in utero or the risk of brain injury due to oxygen deprivation. 11
Conclusion
In conclusion, ultrasonography is used for many purposes in general practice, obstetrical and abdominal examinations being most frequent. This case report highlights the unpredictable nature of these medical situations and stresses the significance of continuous monitoring and timely decision-making. Achievement of these competencies requires educational resources and structured training programs in the field of obstetrics. This approach can help prevent negative outcomes for both the mother and fetus. Acquiring these competencies necessitates access to educational resources and participation in well-organized training programs, as part of obstetrics training. Nevertheless, this case demonstrates the practical bedside potential as POCUS becomes more prevalent in obstetrics.
Footnotes
Ethics Approval
As the study involved a single case and did not involve protected health information, data analysis, or hypothesis testing, ethical approval was not required.
Informed Consent
Informed consent was not obtained because all case data were de-identified and/or aggregated and followed the ethics committee or IRB guidelines.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.