
Abstract
Lung lobectomy can cause a cerebral infarction due to thrombus formation in the pulmonary vein (PV). While contrast-enhanced computed tomography (CT) has commonly been used to detect thrombi, the utility of transesophageal echocardiography (TEE) for thrombus visualization, in the PV stump, is less known. Herein, a series of cases are provided, in which TEE was able to detect a thrombus in the PV stump, as an embolic source of a cerebral infarction. Transesophageal echocardiography is a powerful imaging technique for evaluating thrombi mobility and properties, which are impossible with enhanced CT. Thus, TEE can contribute to identifying the cause of stroke when the embolic source is unknown.
Lung lobectomy can cause a cerebral infarction, due to thrombus formation in the pulmonary vein (PV) stump and is considered a novel source of embolism and stroke. 1 In previous published reports, contrast-enhanced computed tomography (CT) has been commonly used to detect thrombi. Interestingly, stroke neurologists may not realize that transesophageal echocardiography (TEE) can be used to visualize thrombi in the PV stump. To raise awareness, a series of patient cases are provided, in which TEE was used to detect a thrombus in the PV stump, as an embolic source of cerebral infarction. Although TEE has not received much attention as a diagnostic method, it can be useful in the detection of thrombus at the PV stump.
Case Series
Five hundred and eighteen patients (mean age, 78.0 years; 55.6% men) with cerebral infarction were admitted to major medical center (Nagano, Japan) between April 2021 and September 2022. Three patients were selected and TEE was able to detect a thrombus in the PV stump as an embolic source of cerebral infarction. Of these three, two were included in an earlier study designed for a different purpose. 2
Patient Case 1
An 85-year-old man underwent a left lower lung lobectomy for lung adenocarcinoma, using a thoracoscope. The patient recovered post-surgically without complications, and no evidence of new atrial fibrillation was observed. Three days after the operation, the patient developed sudden left hemiplegia. A magnetic resonance imaging (MRI) examination revealed a new cortical cerebral infarction in the right anterior cerebral artery. A general diagnostic search did not reveal the cause of the embolism. Contrast-enhanced CT showed a contrast deficit in the left lower PV stump (See Figure 1A), which was shown to be caused by a thrombus on TEE (See Figure 1B, Supplemental Video 1). The patient was diagnosed with cerebral infarction due to a thrombus that developed in the PV stump.
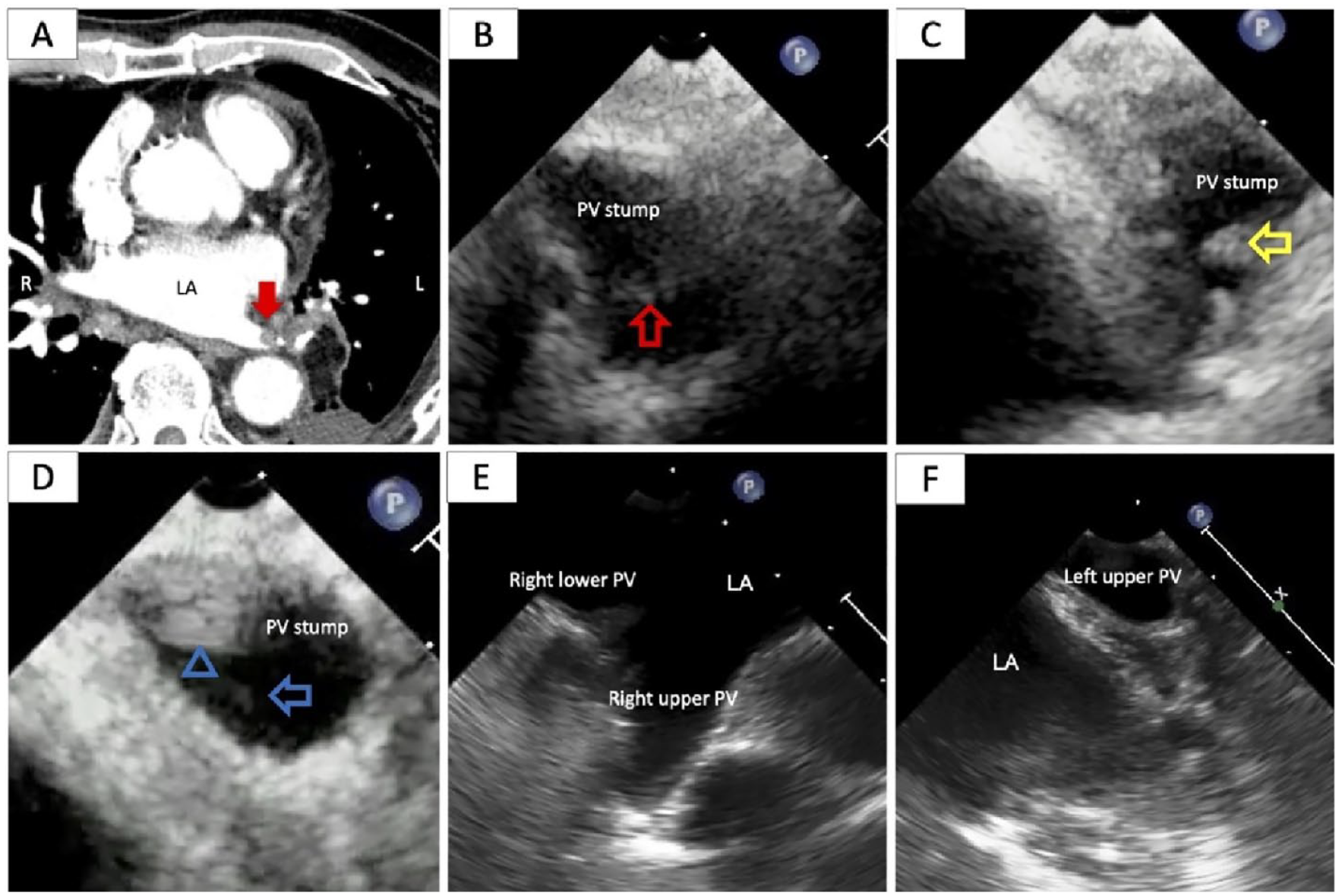
(A) Contrast-enhanced computed tomography (CT) showing a thrombus in the stump of the left lower pulmonary vein (PV) (Note solid red arrow). (B) Transesophageal echocardiography (TEE) demonstrating a thrombus identical to that seen on CT (Note open red arrow). (C) TEE revealed multiple highly mobile and unstable thrombi (Note open yellow arrows). (D) TEE identified a hyperechoic structure, which was the same thrombus seen on CT, at the PV stump (Note open blue arrowhead). Moreover, a low-intensity mobile was connected to a stable thrombus (Note open blue arrow). (E and F) Normal left and right pulmonary veins (PVs) in a patient without lung lobectomy. The PVs’ location, traceable from the left atrium, may change following lung lobectomy; this change is easily discernible after confirming the positional relationship via postoperative CT.
Patient Case 2
A 77-year-old woman had undergone right lower lung lobectomy for a lung adenocarcinoma, 3 years previously. She developed apathy 1 week prior to her hospital admission and a striatocapsular infarction was observed on MRI. Contrast-enhanced CT revealed no PV stump structures. There was no evidence of a thrombus in the left atrial appendage, and its flow velocity was 103.0 cm/s on TEE. Moreover, multiple structures were suspected to be a thrombus and highly mobile on TEE (Figure 1C, Supplemental Video 2). The flow velocity in the PV stump was 49.0 cm/s.
Patient Case 3
A 78-year-old man had undergone left upper lung lobectomy for a lung adenocarcinoma, 6 months previously. He was transported to the hospital with sudden right hemiplegia and drooling. The MRI examination revealed a left cortical cerebral infarction. Contrast-enhanced CT of the chest demonstrated a contrast deficit, suspected to be a thrombus, in the left upper PV stump. The TEE examination showed a stable thrombus and a mobile thrombus, which could not be detected on CT. It was believed to have originated from the stable thrombus (Figure 1D, Supplemental Video 3).
Discussion
No prior reports have described TEE as a powerful diagnostic technique for detecting thrombi in PV stumps. Recently, the usage of TEE has been evaluated in non-cardiac surgery. 3 The TEE can be used to evaluate thrombi in PV stumps after lung lobectomy. Moreover, the mobility and properties of the thrombus and the flow velocity in the PV may be evaluated, which is not possible using enhanced CT.
The PV stump after lung lobectomy can be a site of thrombus formation, which increases the risks for embolism and cerebral infarction, particularly within the first 7 days following surgery. 1 The presence of a venous stump contributes to blood stagnation and creates turbulence. 4 Perioperative hypercoagulability and structural changes can result in thrombus formation and cause cerebral infarction. However, thrombus formation in the PV stump is inadequately recognized by clinicians concerned with stroke. In previous reports of cerebral infarction associated with PV stumps, contrast-enhanced CT, rather than TEE, was used to detect the PV stump thrombus. The search for thrombi in the left atrial appendage is often performed before ablation therapy for atrial fibrillation. A meta-analysis showed that contrast-enhanced CT can detect thrombi in the left atrial appendage. 5 However, mixing artifacts from opacified and non-opacified blood in the PV stump may falsely mimic structures such as thrombi. Recently, the number of reports on PV imaging and examination has increased, driven in part by the growing prevalence of ablation procedures. The TEE is frequently used before and after ablation for evaluating thrombi in the left atrial appendage before the procedure and for PV stenosis after the operation. The method of TEE imaging for PV has already been established, although the distance from the esophagus and the presence of bronchi can prevent visualization.6,7 Previous TEE guidelines have not included a description of PV; however, the latest guidelines included the routine inspection of PVs based on the American Society of Echocardiography/Society of Cardiovascular Anesthesiologists’ standard 28 views. 7 Despite the distance from the esophagus (where the TEE was inserted) to the PV, and although postoperative changes could cause positional changes, the PV was observed in all patient cases described in this report.
The benefits of TEE include the ability to evaluate the presence, mobility, characteristics, and morphology of the thrombus, which may not be possible with CT. However, TEE can be painful, and patients may sometimes require sedation. In contrast, the radiation associated with cardiac multislice CT is of concern, with an estimated effective dose of 6.4–14.8 mSv per study. 8 The various side effects of radiographic contrast media range from mild inconvenience to life-threatening emergencies. 9 PV stump examination should be performed with an overall good concordance between the two diagnostic imaging techniques.
Ten to twenty-five percent of cases of cerebral infarction are referred to as embolic stroke of undetermined source.10,11 It is suspected that some cases of embolic stroke of undetermined source can be attributed to a PV stump thrombus. The TEE is a powerful diagnostic method for detecting thrombi in the PV stump, and clinicians should screen for these thrombi in post-lung lobectomy cases using TEE. After lobectomy, the incidence of a PV thrombus may be unknown or the thrombus may be underdiagnosed, particularly in asymptomatic patients who do not undergo postoperative TEE or CT.
The American College of Radiology has evidence-based criteria stating that TEE is not appropriate for detecting pulmonary embolisms in the pulmonary artery and do not mention the PV stump. 12 The ability to influence those criteria is limited by the low-level evidence provided by this case series and its retrospective nature. Therefore, higher level evidence is needed, and larger prospective studies should be conducted to further validate these diagnostic findings.
Conclusion
Transesophageal echocardiography may be a powerful diagnostic examination tool for detecting and screening for PV stump thrombi, after lung lobectomy. Additional clinical research is needed to validate this diagnostic application.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not sought for the present study because The Nagano Municipal Hospital ethics committee approved the study protocol in accordance with the Ethical Guidelines for Medical and Health Research involving human subjects in Japan.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.