
Abstract
A case study a patient who was emergently evaluated with an intraoperative transesophageal echocardiography after suffering a gunshot wound to the back is provided. This diagnostic examination revealed a left atrium to aorta fistula, due to the path of the bullet through the body. Immediate postoperative imaging with computed tomography revealed that the bullet had embolized to the left femoral artery from which it was later surgically removed. This rare clinical phenomenon of bullet embolization, involving the heart and associated vasculature, is reviewed.
Keywords
Patients with acute cardiovascular pathology due to trauma are frequently unstable and therefore challenging to diagnostically image. Intraoperative transesophageal echocardiography (TEE) is invaluable in such patients and can be performed expeditiously once the patient has been anesthetized and intubated. This case study is provided of a patient whose diagnosis and management were guided by the results of the intraoperative TEE.
Case Report
A 26-year-old man was brought to the emergency department (ED) after suffering a single gunshot wound to the back. The patient was noted to have a prominent jugular venous distention and was tachycardic in the ED (145 bpm), with a blood pressure of 110/100 mm Hg. There was decreased inspiration, in the bilateral lung fields, due to bilateral flutter valves that had been placed by Emergency Medical Services, at the site of the shooting. Chest tubes were placed bilaterally in the ED and a subcutaneous emphysema was also noted. Pulses were recorded as 1+ in the bilateral upper and lower extremities, and this was attributed to acute blood loss anemia. The patient’s skin and conjunctivae were noted to be very pale upon his presentation. His initial hematocrit was 28%, and serial values were obtained, which were 27% and 26%, respectively. Therefore, the patient was transfused with 2 units of packed red blood cells in the ED. While in the ED, he underwent a Focused Assessment with Sonography in Trauma (FAST) examination. The FAST examination originated as sonographic investigation to identify free intraperitoneal or pericardial fluid in patients who had suffered blunt trauma. The scope of the FAST examination has grown to potentially identify other sequelae such as hemoperitoneum, pneumothorax, hemothorax, hemopericardium with or without tamponade, hypovolemia, and fractures. 1 This current patient’s FAST demonstrated a large pericardial effusion; therefore, he was brought emergently to the operating room for a pericardial window. An intraoperative TEE revealed a left atrial to aortic fistula and a resulting sinus of Valsalva pseudoaneurysm (see Figure 1 and Online Supplemental Videos 1 and 2).
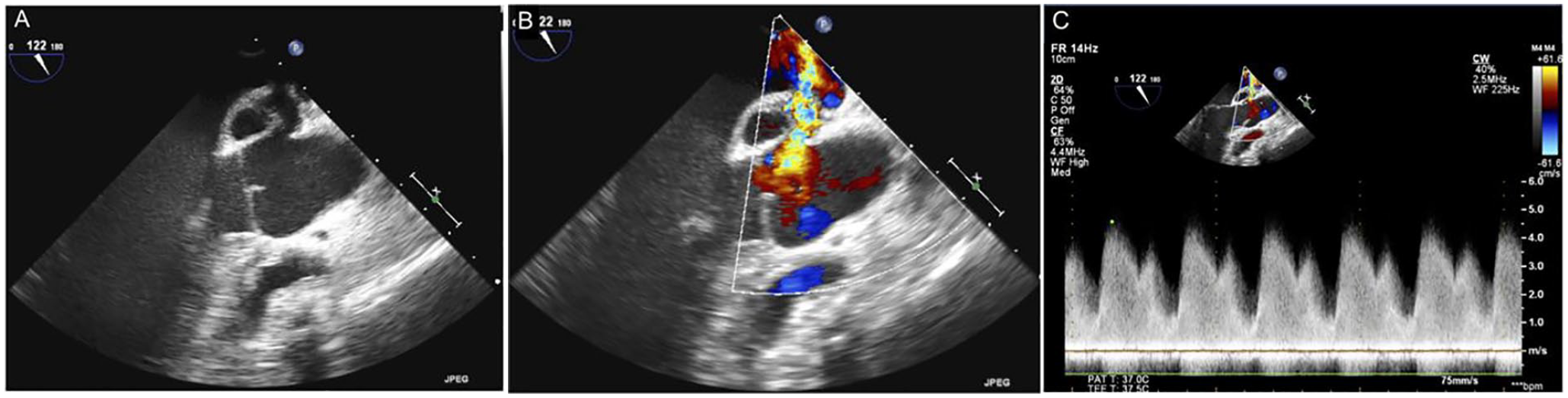
Transesophageal echocardiographic image of left atrium to aorta fistula (a sinus of Valsalva pseudoaneurysm is located along the fistulous tract) in 2D (A) and with color (B) and spectral Doppler (C).
The repair of this was deferred pending transfer of the patient to a nearby institution for cardiac surgery. Postoperatively, but prior to transfer, because of the lack of an exit wound, the patient underwent a computed tomography (CT) which revealed the presence of the bullet in the left femoral artery (see Figure 2).
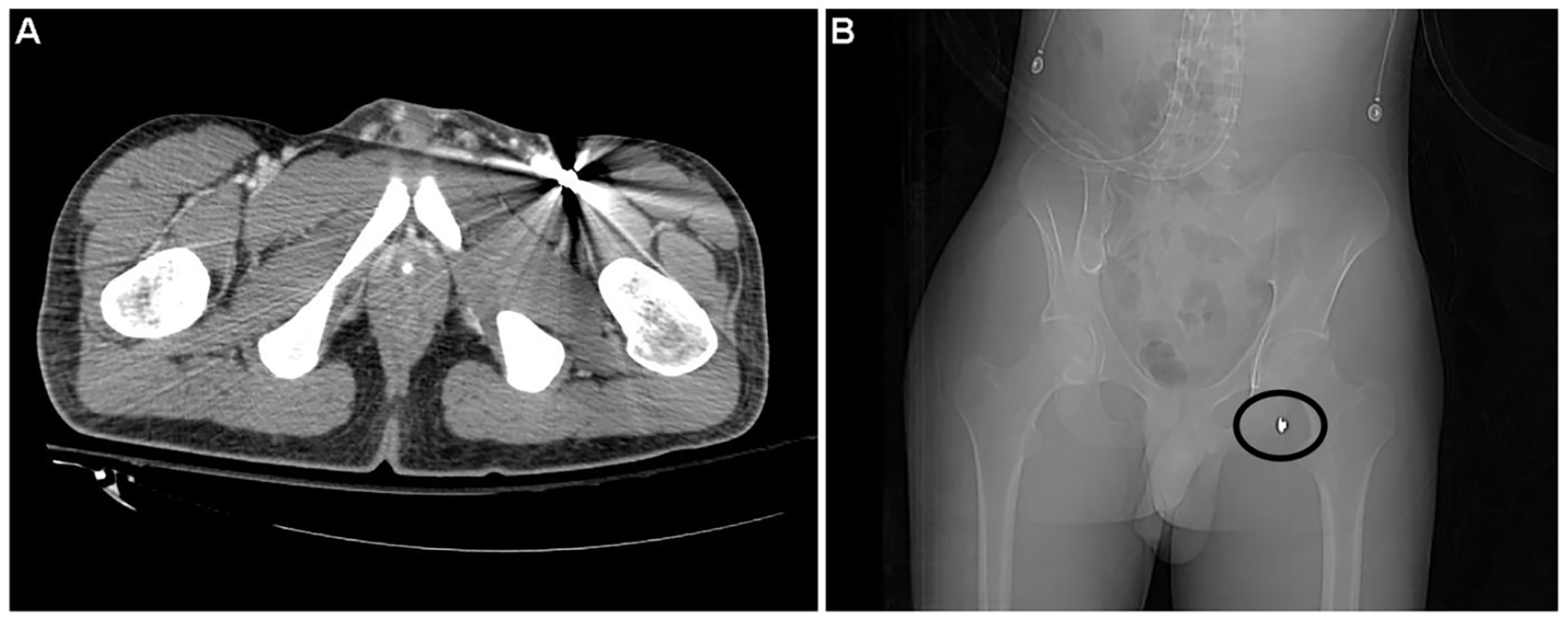
A computed tomographic image that demonstrated a bullet in the left femoral artery in a cross-sectional view (A, bright area on right side with artifact) and on the scout radiographic image (B, circled).
The bullet was presumed to have decelerated sufficiently as it passed through the left atrium and into the aorta (from posterior to anterior, perhaps during systole) such that it did not pass completely through the aorta, but instead was transported distally. The patient underwent median sternotomy with cardiopulmonary bypass. The surgeons found a linear 1 cm tear in the noncoronary sinus which they closed primarily with a suture. After opening Sondergaard’s groove, the entrance point of the bullet was found in the posterior left atrium, which they closed with interrupted sutures. Anteriorly, the “exit wound” from the left atrium was found through the dome of the left atrium and into the coronary sinus. This area was debrided of a small amount of clot and fibrinous material and was closed with interrupted, pledgeted sutures. The left atrium and ascending aorta were both closed in layers. Despite concern that there may have been damage to the valve itself, upon direct inspection the leaflets were unaffected and there was no aortic regurgitation. After repair of the thoracic injuries, the bullet was removed from the femoral artery by a vascular surgery team. Postoperatively, a lower extremity arterial duplex examination demonstrated flow throughout the left lower extremity, but serial physical examination and operative examinations of the lower extremity confirmed extensive ischemic injury, and the patient required a below-the-knee amputation. It was felt that sufficient ischemic damage had occurred prior to the embolectomy such that despite adequate blood flow following the bullet’s removal, the limb became unsalvageable. The patient recovered from his injuries and surgeries uneventfully otherwise.
Serial TEEs were performed both during the remainder of his hospitalization and on an outpatient basis, and further interventions were not required.
Discussion
Vascular embolization of bullets or bullet fragments is a rare complication of a gunshot wound. Estimates of the rates of bullet embolization have ranged from 0.3% to 1.1% in combat settings.2,3 Embolization via the vasculature to the heart, from the heart to more distal sites, and embolization via vessel to vessel have all been described.4–6 The loss of kinetic energy resulting in a bullet entering but not exiting a vascular lumen has been hypothesized to occur more frequently in civilian gunshot victims than in military combat settings due to the generally lower velocity of civilian weapons. 5 In addition, the use of body armor in combat is also thought to be related to a decline in such injuries.7,8 Complications such as tamponade are possible when cardiac chambers are violated, and hypotension, anemia, and shock are reported to be very common in patients presenting with vascular embolization. 9 Of particular interest in this case is that the bullet lodged in the left femoral artery. Aoun et al 10 noted that embolization to the left lower extremity is actually more common than to the right. This is thought to be secondary to the smaller aortic common iliac take-off angle and larger left radius of curvature (in essence a “straighter shot” to go left), which was described in a study of 26 cadavers aged 18–91 years at the time of their death by Shah and colleagues. 11
Many have advised that in the evaluation and management of gunshot patients with vascular injury, if entry and exit wounds are not both discovered, the possibility of bullet embolization should be considered, and appropriate imaging should be performed.5,10,12 Expert consensus guidelines also confirm the central role that FAST examinations and chest radiographs play in the early care of thoracic penetrating trauma victims. 12
Multiple imaging techniques have been used to locate projectiles, including sonography (vascular and cardiac echocardiography), routine radiographs, fluoroscopy, and tomographic techniques, such as CT.13–15 In most cases, expert consensus suggests that the projectiles should be expeditiously removed, although there are certain circumstances in which conservative management has been advocated. In particular, emboli to the pulmonary arteries are one such example. Kortbeek et al 16 reported on 32 cases of pulmonary artery bullet embolism who were managed with observation. Another group reviewed 102 cases of venous bullet emboli and as a result of their review advocated for extraction of such emboli discovered early (within 6 weeks), but that selective observation may be appropriate for asymptomatic individuals whose emboli are discovered later. 17 Others have specifically advocated extraction for intracardiac emboli due to risk such as endocarditis, thrombus formation, and valve dysfunction. 18 The treatment of the area where the bullet enters the vascular system depends, of course, on the organ or organs involved (e.g., the heart, aorta) and may require cardiac and vascular surgical coordination. When the aorta is damaged by either penetrating or blunt injury, a thoracic endovascular aortic repair (TEVAR) has been successfully employed.19,20 Given the rarity of the condition, as well as the wide variety of possible sites of injury and embolization, it seems clear that many management decisions need to be made on a case-by-case basis. Of note, many of the published series include patients managed prior to the advent of sophisticated interventional radiologic techniques, making open surgery their only option for removal. When bullet removal is indicated, modern management includes open surgical, percutaneous, and combined methods of retrieval.13,14,21
Conclusion
As noted by Kuo et al, 19 who reported a case of femoral arterial bullet embolism from the aortic arch, more than 70% of arterial bullet embolization results from penetration of the left-sided cardiac chambers, 22 as in the current case. It is also noted that penetrating trauma to the thoracic aorta is fatal in well over 90% of cases. 23 This makes the survival of the patient described in this case study highly unusual. The case also illustrates the value of intraoperative TEE in the diagnosis and management of unstable trauma patients. This is especially true for those patients who are brought directly to the operating room from the ED, without time for additional imaging. It also emphasizes the value of multimodality imaging in the ongoing management of injuries caused by bullets or other projectiles. This is particularly important when there may or may not be retained material that could have embolized.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.