
Abstract
Idiopathic atraumatic splenic rupture (ASR) is rare, especially in neonates and can result in the spontaneous hemorrhage of the organ, abdominal distension, and hemoperitoneum. This condition can be fatal without prompt diagnosis and surgical intervention. The pathophysiology of ASR is difficult to understand due to its rarity; however, retrospective reviews have found an association with neoplasm, infection, inflammatory diseases, and anticoagulant drugs. Therefore, it is essential to report this rare occurrence. This case report involves a 2-day-old neonate born to a mother with chronic hypertension, chorioamnionitis, and a carrier of cystic fibrosis. An abdominal sonogram followed by contrast-enhanced computed tomography (CT) revealed hemoperitoneum with possible active bleeding and lack of definite visualization of the spleen. During emergency laparotomy, the attempt to preserve the organ was unsuccessful, requiring splenectomy. The neonate recovered well from the procedure and was discharged on the 18th day of life.
Atraumatic splenic rupture (ASR) involves spontaneous hemorrhage of the organ without any blunt trauma to the abdomen, leading to abdominal distension, hemoperitoneum, and hypovolemic shock.1 –3 Although the occurrence of ASR is rare, it requires immediate medical intervention to avoid life-threatening conditions, including death.1 –4 The etiology of ASR is not yet fully comprehended. The retrospective analyses of patient cases of ASR relate the condition to the presence of neoplasm, infection, inflammatory diseases, and the usage of anticoagulant drugs.1 –7 The case presented involves a neonate, who was probably negatively affected by her mother’s medical conditions.
Case Report
A 2-day-old female neonate with a gestational age of 38 weeks and 2 days was born via normal vaginal delivery to a 33-year-old mother with chronic hypertension, chorioamnionitis, and a carrier of cystic fibrosis. The prenatal screenings and sonographic findings were unremarkable. The mother did not have a history of tobacco, alcohol, or drug usage. She was treated with nifedipine and labetalol, during pregnancy, for hypertension and was given antibiotics during labor. Although the neonate appeared well at delivery, she was kept in the hospital for continuous glucose monitoring due to maternal beta-blocker usage and for signs and symptoms of infection.
The infant’s serum total bilirubin (Tbili) was 9.9 mg/dL at 24 hours of life with no signs of infection or evidence of hypoglycemia. Her weight decreased by 2.3%, on the first day of life, which further deceased by 7.1%, the following day.
On the second day, additional issues were noted such as hypothermia, hypoglycemia, jaundice, pallor, lethargy, poor muscle tone, abdominal distension, tachycardia (160–180 bpm), and hypotension (73/53 mmHg). A reduced hemoglobin level (42 g/L), an increased white blood cell count (20.2 × 109/L), and increased Tbili (16 mg/dL) were also noticed. Phototherapy, glucose and antibiotics administration, and sepsis protocol were initiated. A significant event was called, and the patient was transferred to the critical care unit (CCU) for sudden hemodynamic compromise and worsening anemia of unknown origin. A transfusion of 15 mL/kg packed red blood cells over next 3 hours of admission, to the CCU, was ordered. In addition, an abdominal and neurosonogram was conducted to find any possible source of hemorrhage.
The spleen was not identified with abdominal sonography, but rather a large heterogeneous, complex collection with pronounced vascularity, measuring approximately 5.5 × 3.3 × 4.7 cm, was noted in the left upper quadrant (LUQ) (see Figure 1). A moderate to large volume of complex free fluid was also seen in all quadrants and pelvis, likely representing blood, given patient’s clinical history. Although hemoperitoneum limited the visualization of bilateral adrenal glands, the expected locations appeared within normal limits. A differential diagnosis of LUQ hematoma or abscess with hemoperitoneum was made. A contrast-enhanced computed tomography (CT) of the abdomen and pelvis was ordered for further diagnostic assessment.
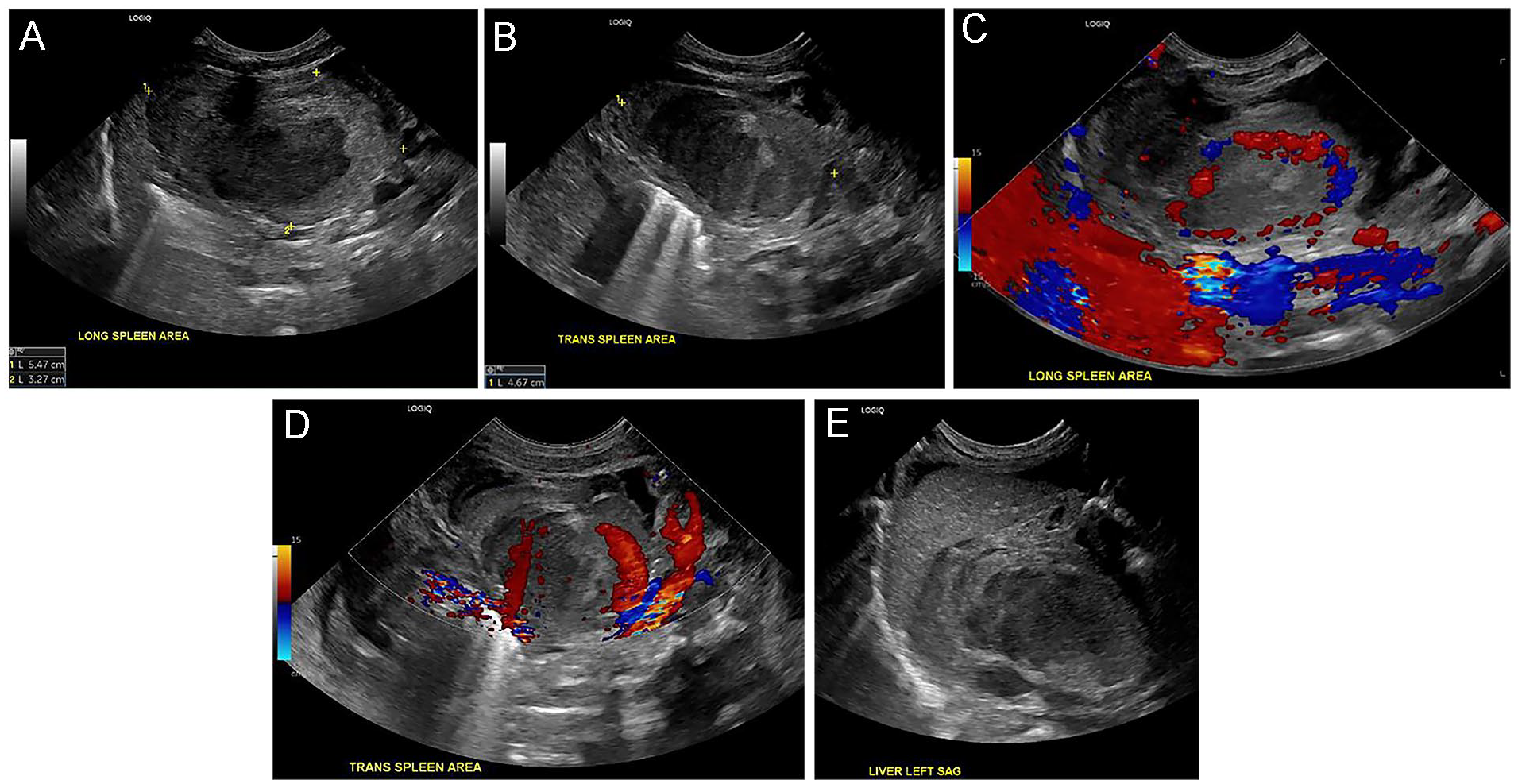
Grayscale sonographic images of a large hematoma in (A) the sagittal plane and (B) the transverse plane. Color Doppler (C and D) depicts hyperemic flow, in the sagittal and the transverse planes, respectively. The hematoma was seen posterior to the left lobe of the liver (E).
The neurosonogram identified increased echogenicity within the bilateral thalamic region (left greater than right), and subtle, patchy areas of increased echogenicity within the bilateral periventricular white matter, including the left parietooccipital region (see Figure 2). Also, a mild loss of gray-white matter differentiation was visualized bilaterally along the midline. The constellation of findings indicated possible ischemic and/or infectious parenchymal involvement in this neonate, given the history of maternal infection. A magnetic resonance imaging (MRI) study was recommended for further assessment, if clinically indicated.
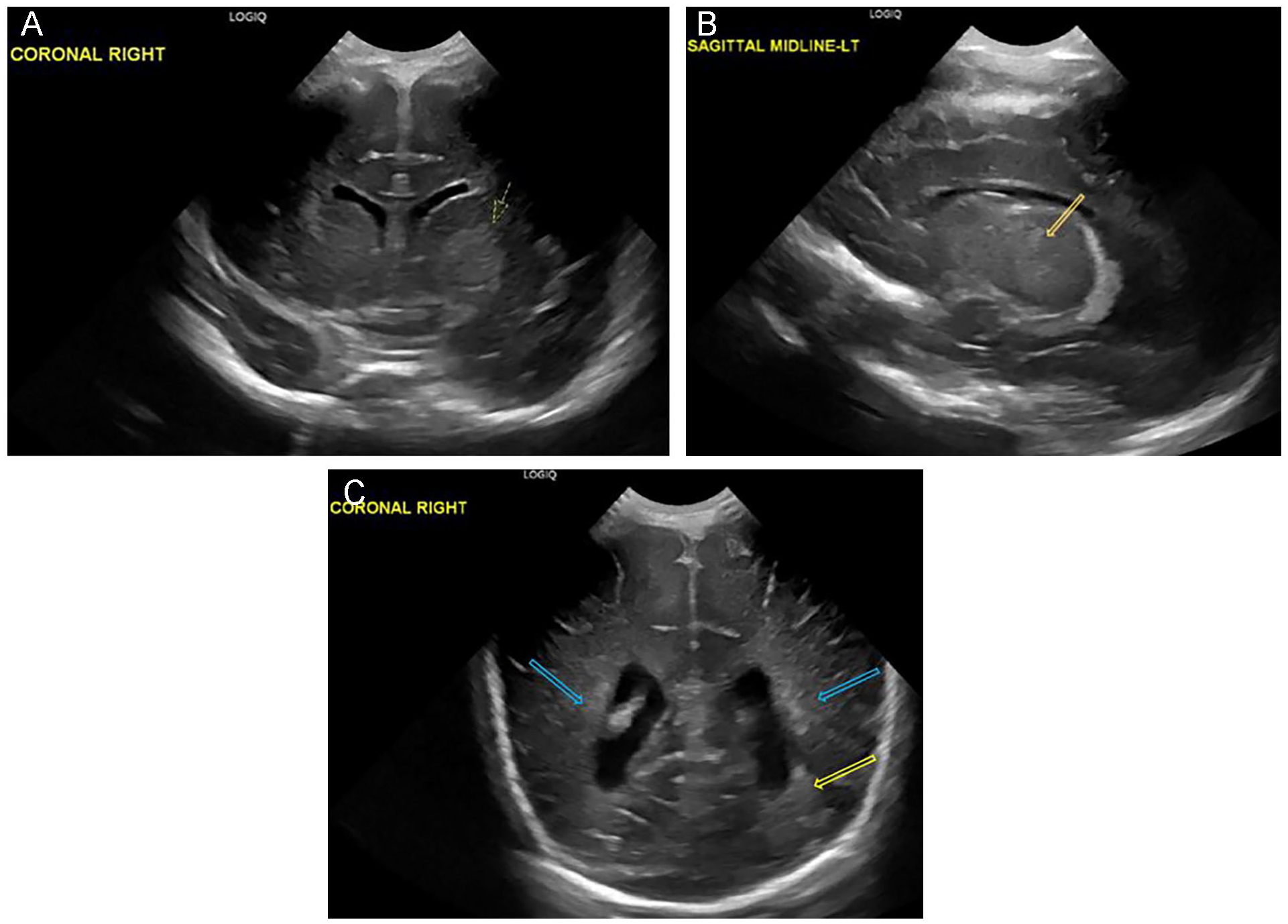
Grayscale sonographic images of the 2-day-old neonatal brain, depicting increased echogenicity within the left thalamus, in the coronal plane (A) and the sagittal plane (B). Subtle, patchy areas of increased echogenicity within the bilateral periventricular white matter (blue arrows) and the left parietooccipital region (yellow arrow) (C).
High density tissue with irregular contour and shape was visualized on the CT, anterior to the left kidney, likely representing splenic tissue (see Figure 3). A blush of contrast was seen within the mesentery, adjacent to the branches of the superior mesenteric artery and next to the splenic tissue, which was thought to be a possible active splenic extravasation, given the organ’s irregular contour and hyperattenuating tissue. Large volume of high-density fluid was also seen throughout the abdomen, likely representing hemoperitoneum, which had increased in size from the previous sonogram. Bilateral adrenal glands appeared normal. With a concern for splenic rupture or laceration, surgical consultation was recommended.
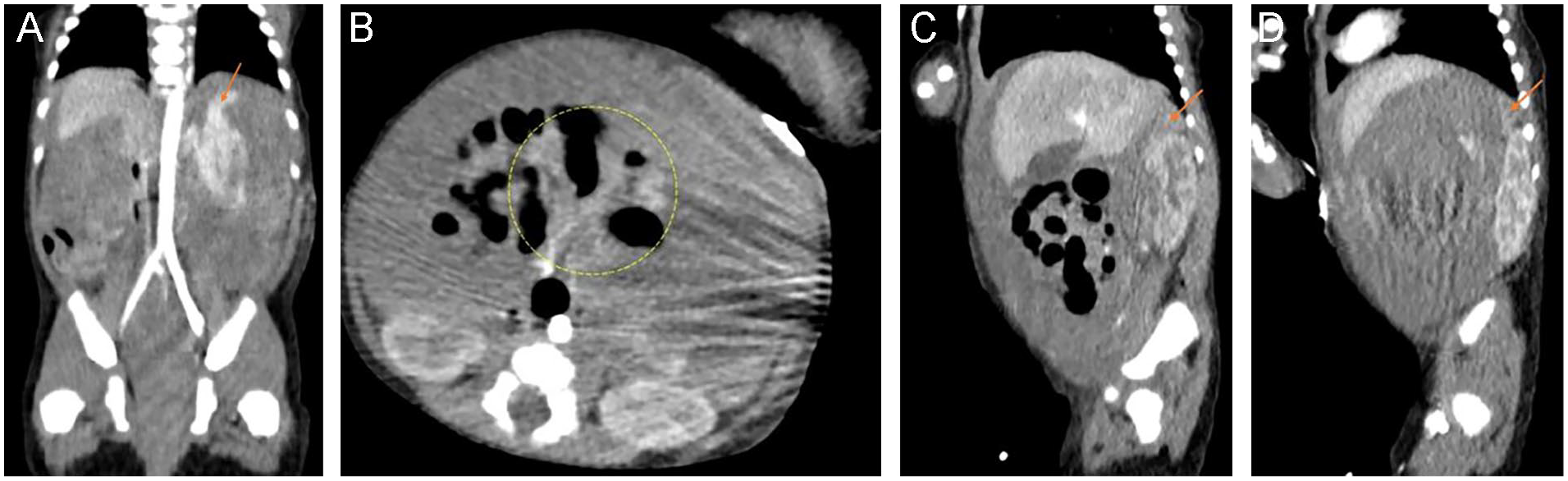
Contrast-enhanced computed tomography images of the abdomen and pelvis in the 2-day-old neonate, depicting possible splenic tissue (arrow) in the coronal plane (A), a blush of contrast (yellow circle) within the mesentery, next to the splenic tissue (B), and normal appearing right and left adrenal glands, respectively (arrows), in the sagittal plane (C and D).
On the third day of life, an emergency laparotomy was planned, due to a potentially active hemorrhage and known hemoperitoneum. As the abdomen was surgically entered, during the intervention, an immediate rush of hemoperitoneum was seen. Each quadrant of the abdomen was packed, followed by careful systematic evaluation. There was minimal bleeding in the lower quadrants, right upper quadrant, and the pelvis. When the packing on the LUQ was removed, ongoing bleeding was visualized in that area. The spleen was found to be encased by a large clot. After removal of the clot, a tear in the splenic capsule was revealed. The attempt to preserve the organ was unsuccessful, with the patient requiring continuous transfusion and becoming transiently hypotensive. A splenectomy was performed in piecemeal fashion that stopped the bleeding. The patient tolerated the procedure well and was taken to the intensive care unit in stable condition.
On the seventh day, an MRI was ordered to follow the results of the neurosonogram, which had demonstrated concerns for ischemia. Multiple foci of restricted diffusion were visualized within the bilateral periventricular white matter, compatible with ischemic foci (see Figure 4). Small hemorrhagic focus was also visualized within the left choroid plexus. There was no obvious signal abnormality within the basal ganglia to suggest profound hypoxic–ischemic insult. Bilateral ventricles were mildly prominent, compared to the prior sonogram, without significant ventriculomegaly.
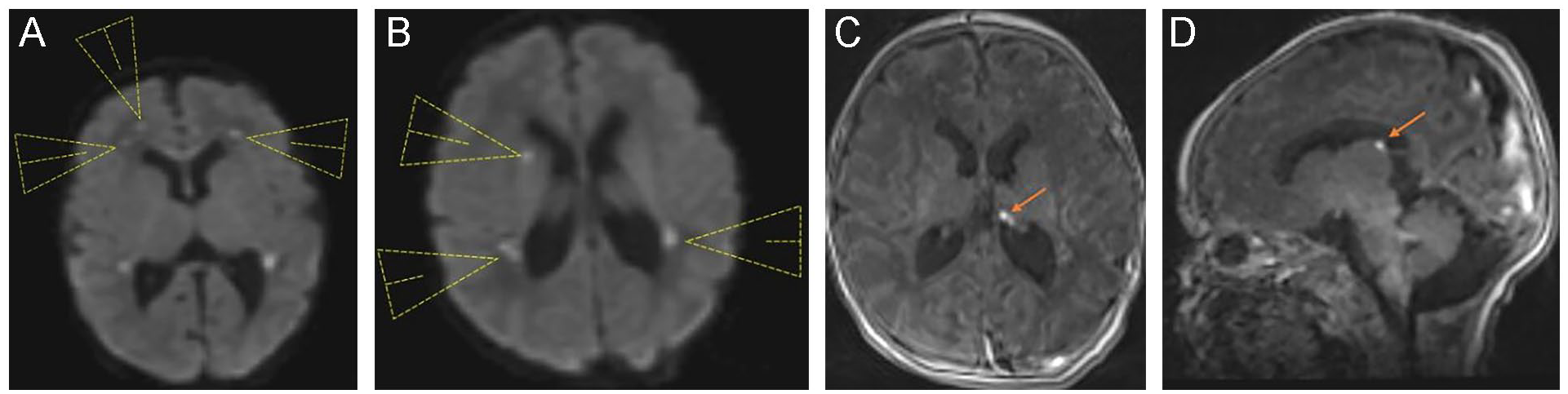
Diffusion weighted magnetic resonance imaging (MRI) of the 7-day-old neonatal brain, depicting multiple ischemic foci (arrow heads) within the bilateral periventricular white matter (A and B). MRI images showing a small focus of hemorrhage (arrow) within the left choroid plexus, in the coronal plane (C) and in the sagittal plane (D).
The infant was administered antibiotics and had an uneventful recovery. By the 17th day, appropriate weight gain per os (by mouth) was observed, and the patient was discharged from the hospital on day 18. The infant’s 3-week follow-up visit (3 days after the discharge) and 2-month and 6-month office visits were unremarkable with appropriate feedings and bowel movements.
Discussion
The spleen is the largest lymphatic organ and has both hematopoietic and immunologic functions. It is not a considered to be a vital organ. In its absence, other organs, such as the liver, can adapt to provide the same functions. The spleen is densely vascular and is encased in a weak connective tissue capsule that provides protective cushion to the organ.
Splenic surgery typically is a result of a traumatic event to the organ. 1 Splenic rupture or laceration may lead to intra-abdominal bleeding, causing life-threatening conditions and requiring surgical intervention. On occasion, as described in this case report, spontaneous hemorrhage of the spleen may occur. Atraumatic splenic rupture is a rare condition, but it can happen at any stage of life.1 –7 Due to its rarity, the pathogenesis of ASR is not well understood. Therefore, it is encouraged that ASR cases should be reported to gain further insight into the condition.
Atraumatic splenic rupture is idiopathic and presumed to be caused by many factors, including malignancy, infection, systemic or local inflammation, and anticoagulant drug usage.1 –7 The presentation of ASR may involve the pentad of abdominal distension, hypovolemic shock, anemia, active bleeding, and hemoperitoneum. Although abdominal distension may be a clinical sign and noted during a physical exam, diagnostic imaging is most helpful to investigate the last two symptoms. Evidence of hypovolemic shock and anemia can be observed clinically and confirmed through laboratory findings. Other signs and symptoms of ASR may also include abdominal pain possibly radiating to the shoulder, LUQ pain or tenderness, nausea, weakness, intestinal obstruction, fluctuations in alertness, and peritonitis.1,3,5,6 Despite the variability in the presentation of this condition, ASR should always be suspected when abdominal distension or pain is accompanied by hypotension and/or anemia, as this has been described in the literature. 6 The present case study highlights these concerns.
Some of the differential diagnoses of ASR may include necrotizing enterocolitis and solid organ hemorrhage, including the adrenal gland and liver. 2 Due to the absence of trauma to abdomen, ASR may involve delayed or missed diagnosis and treatment, resulting in fatal outcomes. 6 ASR is associated with about 12% of mortality rate. 6 Thus, like its traumatic counterpart, ASR also requires urgent medical attention to avoid negative patient outcome. 3 Splenectomy appears to be the most common treatment method for ASR. 3 In contrast, traumatic rupture may involve either operative or nonoperative management (such as embolization or close monitoring with repeat abdominal imaging), depending on the severity of the damage to the organ and the patient’s condition. 3
The neonate, in the present case study, had a normal delivery but had possible complications due to the mother’s chorioamnionitis. A Greek experimental study reviewed the consequences of chorioamnionitis on developing human fetal spleen and found no significant effect during the first trimester. However, a drop in the number of needed proteins and compromised hematopoietic capability and depletion of the spleen was observed during the second and the third trimesters, along with reduced number of B and T lymphocytes during the third trimester. 8 It was also reported that chorioamnionitis can aid in developing systemic inflammatory responses in fetuses, affecting multiple organs, such as the spleen, heart, lungs, kidneys, brain, and eyes. 8
This neonatal patient was kept under close observation in the hospital, which resulted in a favorable outcome. Tracking the clinical and laboratory findings that began to deteriorate on the second day resulted in a search for the source of a hemorrhage, using abdominal sonography. Although definitive splenic tissue was not visualized, this study identified the LUQ heterogeneous collection with hyperemic flow, along with hemoperitoneum. Due to the complex nature of this presentation resembling other differentials, a CT was ordered that aided in the diagnosis and prompt intervention. Both sonography and CT are the diagnostic imaging techniques used to diagnose ASR.1 –3,5,7 Sonography is helpful in determining hemoperitoneum and any large complex collection in the abdomen with or without active bleeding and is perhaps the initial preferred imaging technique, especially in newborns and children, due to its noninvasive nature.
A study that analyzed eight patient cases of ASR found the sensitivity of sonography and contrast-enhanced CT as 57% and 86%, respectively, and the accuracy of CT in diagnosing the condition as almost 100%. 1 According to a report of a newborn’s ASR, the pediatric surgeons were not aware of the possibility of spontaneous hemorrhage of the organ. 2 Hence, based on the sonographic study that revealed left suprarenal hematoma, they assumed adrenal hemorrhage and opted for nonoperative management. 2 With worsening condition overnight, a CT was ordered that confirmed intraperitoneal hemorrhage an dislocation of the spleen. Even with delayed treatment, the infant was able to survive with the removal of the damaged organ.
Conclusion
This neonatal patient case of ASR signifies how quickly the condition can deteriorate, and how prompt diagnosis and treatment are vital to saving life. It is essential to be aware that spontaneous rupture of the spleen can happen at any stage of life. Along with collecting the patient history for any possible causal association to this condition, clinical and laboratory findings for abdominal pain or distension, hypovolemic shock, and anemia are key takeaways to order for radiologic imaging to look for a source of hemorrhage. A prompt diagnosis, based on the results of diagnostic imaging, will likely require a prompt surgical intervention, to insure a favorable patient outcome.
Footnotes
Acknowledgements
The author wishes to thank Katheryn Johnson, BS, RDMS, and Dr. Benjamin D. Smith, Department of Pediatric Radiology, of UNC Medical Center, Chapel Hill for their help and support.
Ethics Approval
Ethical approval was not sought for the present study because only anonymous information was used in the case report, and the institution provided deidentified images to be used for the publication.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.