
Abstract
Objective
Although rare, late-diagnosed atraumatic splenic rupture (ASR) may result in mortality. We investigated the occurrence of ASR cases at our centre over the previous six years.
Methods
This was a retrospective, cross-sectional study that included all patients who underwent emergency splenectomy due to ASR between January 01, 2015, and January 01, 2021.
Results
Of the 203 patients who underwent splenectomy, 15 met our criteria for ASR. Median age was 55 years (34–90), and 10 (67%) patients were male. Most common pre-existing diseases were diabetes mellitus (6, 40%) and heart valve disease (5, 33%). Ten (67%) patients had splenic rupture due to splenic infarction and abscess. There were two (13%) cases with diffuse large B cell lymphoma (DLBCL) and two (13%) cases with lung cancer and spleen metastasis. Median length of hospital stay was 6 days (2–24) and three (20%) patients died in hospital.
Conclusions
Male sex, previous splenic infarctions, haematological malignancies, lung cancer spleen metastases, underlying cardiovascular disease and diabetes mellitus may increase the risk for ASR. Further prospective controlled studies are needed to confirm our results.
Introduction
The most common indication for emergency splenectomy is trauma to the spleen whether external (blunt or penetrating) or iatrogenic. 1 Atraumatic splenic rupture (ASR) is a rare condition. 2 In a histologically proven normal spleen, ASR is called a spontaneous rupture or true spontaneous rupture, whereas, in a diseased spleen, ASR is described as a pathological rupture.2–6 The main causes of ASR are neoplastic, haematological, inflammatory, infectious, mechanical, treatment-related, and idiopathic disorders.2–7 Late diagnosed ASR may result in significant mortality. For example, in a systematic review, ASR-related mortality rate was estimated to be 12%. 7 However, reference to this condition in emergency medicine literature and electronic sources is minimal. 7 Therefore, this rare and serious condition may be overlooked by emergency physicians.
Diagnostic and therapeutic methods for the optimal management of splenic injury have improved over recent years. 8 Therefore, we decided to investigate the occurrence of ASR cases at our centre over the previous six years. By providing these data, we hope to improve our emergency physicians’ knowledge of this rare and life-threatening condition.
Methods
This retrospective study was conducted at the University of Samsun, Samsun Training and Research Hospital, Samsun, Turkey. The study followed guidelines outlined in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement. 9 The study was approved by the Institutional Review Board (IRB) of Samsun Training and Research Hospital (GOKA/2021/11/1) and written/verbal consent was not required because it was a retrospective study.
Hospital records were reviewed for all consecutive, adult patients who had undergone emergency splenectomy between January 01, 2015, and January 01, 2021. To avoid the potential risk of bias, one researcher extracted all data, and a second researcher independently checked data extraction forms for accuracy and detail. Patients included in the study were at least 18 years of age and had experienced emergency service admission with hypovolemic shock or acute abdominal pain related to the spleen diagnosed by an imaging test (i.e., ultrasound or computerized tomography [CT]). In addition, they had undergone a splenectomy within 24 hours of admission. Patients who had undergone emergency splenectomy related to trauma (i.e., external or iatrogenic), and those who had undergone angioembolisation, or had been closely followed without intervention, were excluded from the study.
Demographic information (i.e., age, sex, body mass index [BMI], Charlson Comorbidity İndex [CCI], blood pressure [BP] aetiology) and laboratory tests results recorded on admission were extracted from the patients’ medical records. Based on the CCI score, the severity of comorbidity was categorized into three grades: mild (1–2); moderate (3–4); severe (≥5).
Clinical variables recorded post-surgery included: Clavien-Dindo Classification (CDC); intensive care unit (ICU) stay; length of hospital stay; complications; hospital mortality. The CDC index is used in the classification of surgical complications. 10 It has seven grades (I, II, IIIa, IIIb, IVa, IVb and V) that range from mild (1) to death (V). The total number of red blood cell (RBC) transfusions (i.e., preoperative, during the operation and postoperative) were also recorded. Patient data were evaluated for their characteristics and no formal statistical analysis was applied.
Results
Of the 203 patients (83 elective, 120 emergency) who underwent splenectomy between 01 January 2015, and 01 January 2021 at our centre, 15 cases met our criteria for ASR. Demographic details on admission are shown in Table 1. Median age was 55 years (range 34–90), and 10 (67%) patients were male. With the exception of one patient, all patients experienced abdominal pain. The most common concomitant medical conditions were diabetes mellitus (6 patients, 40%) and heart valve disease (5 patients, 33%). Eight (47%) patients had more than one comorbid disease. With regard to CCI scores, eight patients were assessed as mild (1–2), three as moderate (3–4) and four as severe (≥5). According to BMI, one patient was underweight (17 kg/m2), three were normal weight (18.5–24.9 kg/m2), six were overweight (25–29.9 kg/m2) and five were obese (≥30 kg/m2).
Patient demographics and baseline characteristics on admission.
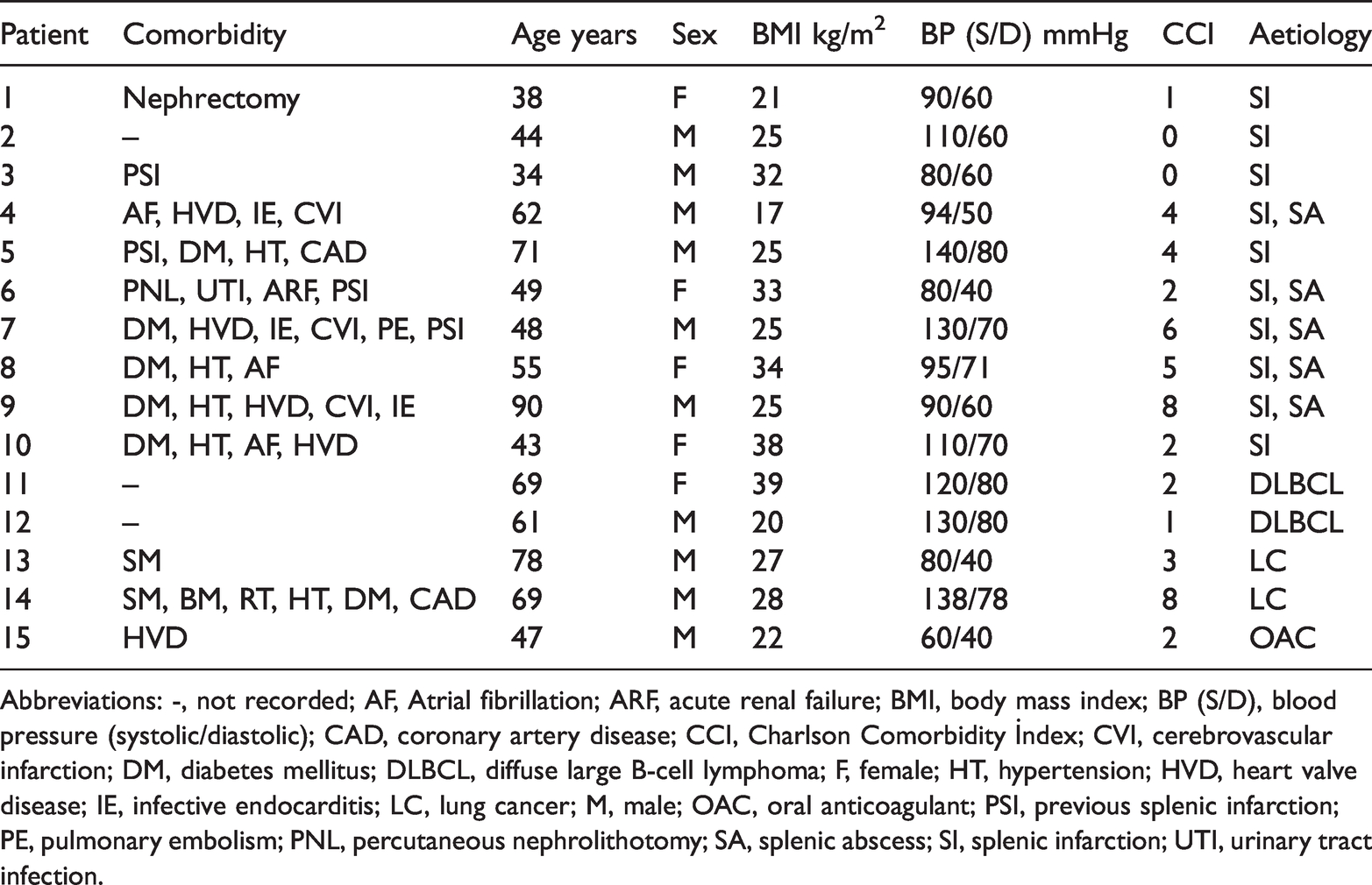
Abbreviations: -, not recorded; AF, Atrial fibrillation; ARF, acute renal failure; BMI, body mass index; BP (S/D), blood pressure (systolic/diastolic); CAD, coronary artery disease; CCI, Charlson Comorbidity İndex; CVI, cerebrovascular infarction; DM, diabetes mellitus; DLBCL, diffuse large B-cell lymphoma; F, female; HT, hypertension; HVD, heart valve disease; IE, infective endocarditis; LC, lung cancer; M, male; OAC, oral anticoagulant; PSI, previous splenic infarction; PE, pulmonary embolism; PNL, percutaneous nephrolithotomy; SA, splenic abscess; SI, splenic infarction; UTI, urinary tract infection.
Thirteen (87%) patients had elevated WBC levels and 14 (93%) patients had haemoglobin values below the normal range (Table 2). Two (13%) patients had low platelet counts and five (33%) had values greater than normal range. Two (13%) patients had elevated AST levels and a further two (13%) had elevated ALT levels. However, apart from two (13%) patients who had marginally low values, all patients had total bilirubin levels within the normal limits. Twelve (80%) patients had lactate levels >1.6 mmol/l. CRP levels were measured in seven patients and all had elevated values.
Laboratory test results on admission and RBC transfusions.

Abbreviations: -, not recorded; WBC, white blood cells; Hb, haemoglobin; AST, aspartate aminotransferase; ALT, alanine aminotransferase; CRP, C-reactive protein; RBC, red blood cell.
Numbers in bold are outside normal range.
*RBC transfusions occurred preoperatively, during the operation and postoperatively.
Indication for surgery in 10 (67%) patients (Numbers 1–10) was splenic rupture due to splenic infarction; five of these patients had splenic abscess (Table 1). We determined that the abscesses were related to previous splenic infarctions. Of these patients, nine (90%) had elevated WBC counts and five (50%) had elevated platelets. (Table 2). CT images from a patient with splenic rupture due to previous splenic infarction are presented in Figures 1a and b.

Contrast enhanced coronal (a) and axial (b) abdominal computed tomography (CT) scans from one patient showing splenic infarct and associated splenic rupture (white arrows).
Two (13%) patients were diagnosed with diffuse large B cell lymphoma (DLBCL) postoperatively by histological assessment. Figure 2 shows an enlarged spleen and splenic rupture from one of the patients with DLBCL. Another two (13%) patients were diagnosed postoperatively with splenic metastasis of lung cancer. The CT image of one of these patients is presented in Figure 3. Both patients were brought to our emergency department in haemorrhagic shock; one patient was receiving concurrent radiotherapy.

Computed tomography (CT) scan of the abdomen of a patient who was diagnosed postoperatively with diffuse large B cell lymphoma (DLBCL). The scan shows splenic rupture of the abnormal spleen (white arrow).

Abdominal computed tomography (CT) scan showing splenic rupture (white arrow) with spleen metastases due to lung cancer.
Only one patient (Patient 15) had a histologically normal spleen apart from the rupture. This patient had undergone an aortic and mitral valve replacement and was receiving oral anticoagulant therapy (warfarin, 10 mg once daily). All of the remaining patients had a diseased spleen and so may be classed as pathological ruptures.
Ten (67%) patients had haemorrhagic shock and five (33%) were hemodynamically unstable and all 15 patients required RBC transfusions (range 2–5). Median length of hospital stay was 6 days (range 2–24) and median ICU stay was 2 days (range 0–20) (Table 3). Seven (47%) patients had no complications following the surgery. Of the eight (53%) patients that had complications, four experienced a cerebrovascular infarction and there were single cases of femoral artery embolism, acute pancreatitis, mesenteric ischaemia, or gastroparesis. The CDC grades for these patients were as follows: one patient was grade I (i.e., any deviation from the normal postoperative course); three were grade II (i.e., requiring pharmacological treatment); one grade IIIb (i.e., intervention under general anaesthesia); three grade V (death). 10
Patient outcomes following atraumatic emergency splenectomy.

*Classification of surgical complications in 7 grades (I, II, IIIa, IIIb, IVa, IVb and V) ranging from mild (1) to death (V).
Abbreviations: –, not recorded; ICU, intensive care unit; FAE, Femoral artery embolism; CVI, cerebrovascular infarction.
Of the three (20%) patients who died in hospital, two had been diagnosed with splenic infarction and died due to cerebrovascular infarction in the postoperative period. The remaining patient died due to mesenteric ischemia on the second day following surgery.
Discussion
With the exception of trauma-related cases, splenectomy is rarely performed as an emergency procedure. In addition, true spontaneous rupture of a normal spleen is extremely rare.2,5,6 The diagnostic criteria for spontaneous splenic rupture have been defined as; no history of trauma; no evidence of disease in other organs that are known to affect the spleen adversely; no proof of adhesions or scarring of the spleen; the spleen should be normal on histological examination. 2 However, we believe that many investigators misinterpret the rupture of a diseased spleen as a spontaneous rupture. In this present study, none of our patients had a true spontaneous splenic rupture. All our patients had underlying diseases. Only one patient had a histologically normal spleen, apart from the signs of rupture. This patient had undergone an aortic and mitral valve replacement and was receiving anticoagulant therapy.
The symptoms of ASR vary but the presence of abdominal pain has been frequently reported. 11 In our study, only one patient did not experience abdominal pain. However, abdominal pain may be a symptom of other conditions such as, biliary tract disease, perforated peptic ulcer, acute pancreatitis, ruptured aortic aneurysm, and myocardial infarction. ASR has been reported to occur more frequently in men.4,7,12 Indeed, there was a 2: 1 male: female predominance in a systematic review that included data from 845 patients with ASR. 7 Likewise, we found most of the patients with ASR were male (67%).
The most common reason for atraumatic emergency splenectomy in this study was splenic rupture due to splenic infarction and abscesses (67% patients). We determined that all rupture splenic abscesses were related to previous splenic infarctions. Interestingly, a review of data from 613 cases of splenic rupture, found only six patients had splenic rupture caused by splenic infarction. 13 Splenic infarction occurs when occlusion of the splenic vascular supply leads to tissue ischemia and necrosis. It can arise from either arterial or venous occlusion and thromboembolism is the most common cause.14–17 Thromboembolism can be caused by a wide variety of underlying diseases and the prognosis is mostly related to these diseases. 15 In the present study, all patients with splenic infarction had one or more risk factors for thromboembolism (i.e., heart valve replacement, diabetes mellitus, hypertension, or coronary artery disease). Similar to other studies, we found 33% of patients who developed a splenic rupture due to splenic infarction had previous heart valve surgery.14,18 Therefore, a possible explanation for the difference in findings between our study and previous studies may be related to differences in the number of cardiac diseases and cardiac invasive interventions. 13 In addition, the difference may be related to recent and improved diagnostic and treatment methods at our centre.
Previous studies have reported that splenic infarction is a rare cause of spontaneous rupture and may lead to massive haemoperitoneum.19,20 Therefore, with its potential for complications such as rupture or abscess, splenic infarction should be included in the differential diagnosis whenever evaluating a patient with acute abdominal pain and haemorrhagic shock. We found 67% of our cases had haemorrhagic shock and 33% cases were hemodynamically unstable. Indeed, all patients required RBC transfusions because of haemodynamic instability.
Patients with haematologic malignancies (i.e., DLBCL) accounted for 13% of our cases. In agreement with our findings, pathological splenic rupture has been reported previously in patients with haematological malignancies such as leukaemia and lymphoma.3,4,7,14,21 In another 13% patients, we identified splenic rupture was caused by splenic metastasis of lung cancer. In a systematic review of data from 613 cases of splenic rupture, only four cases were caused by lung cancer. 13 Therefore, although extremely rare, splenic metastasis of lung cancer should be considered within the differential diagnosis of a splenic rupture. It has been suggested that patients’ survival following ASR is probably correlated with the course of the underlying disease. 6 In agreement with these findings, we observed a high mortality rate (20%) and it was related to the patients’ concomitant diseases.
Our study had limitations. For instance, it was a retrospective and data were obtained from electronic medical records and so results may have been influenced by interpretation biases. In addition, it was a non-comparative, cross sectional study and no formal statistical analysis was applied. Therefore, further prospective, controlled studies are required to confirm our findings.
In conclusion, data collected from our hospital records over recent years, showed that there was a high incidence of splenectomy for atraumatic reasons. Male sex, previous splenic infarctions, haematological malignancies, lung cancer spleen metastases, underlying diseases (e.g., cardiovascular disease, diabetes mellitus) may increase the risk for ASR. In particular, ASR should be suspected when acute abdominal pain and signs of hemodynamic instability occur in a background of splenic infarctions, haematological disorders, malignancies, and/or therapeutic anticoagulation. We believe our current findings are important for emergency physicians, gastroenterologists, and surgeons, because although rare, late-diagnosed ASR may result in mortality.