
Abstract
Chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL) are slow-growing cancers that affect the immune system by disrupting the normal function of B-cells. The patient symptoms associated with CLL and SLL can be vague; therefore, many cases go undiagnosed for years. Diagnostic medical sonography is an imaging technique that can determine the abnormal appearance of lymph nodes and guide medical providers in the appropriate direction when investigating a questionable case of lymphoma. This case study presents a superficial left-neck sonogram of a 65-year-old Caucasian man complaining of left supraclavicular pain and swelling. This initial sonogram was the first phase in a sequence of examinations that led to the patient’s diagnosis of CLL/SLL.
Keywords
Chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL) are the most common forms of lymphoma in adults living in Western countries. 1 Given the disease’s impact on the lymphatic system, sonography is a valuable tool for distinguishing between benign and malignant lymph nodes. Compared to a computed tomogram (CT), sonography is nonionizing, cost-effective, noninvasive, and easily reproducible, which makes it the preferred first-line imaging technique for diagnosing cervical lymphadenopathy.1 –3 Sonography can be extremely useful in the detection and evaluation of both normal and abnormal lymph nodes, as well as aid in the guidance for biopsy sampling, which is an integral stage of a cancer patient’s diagnosis. Sonographic parameters used when evaluating lymph nodes are size, margins, echogenicity, and distribution of vascular flow. 4 The cervical lymph nodes account for about 40% of the total lymph nodes in the body; therefore, the neck is a common anatomical site for lymphadenopathy. 5 Jalili et al. 3 stated that sonography is a useful method for the detection of abnormal lymph nodes, with a moderate sensitivity rate of 48.8% to 87.1%.
Case Report
A 65-year-old Caucasian man presented to an urgent care facility with left supraclavicular swelling and pain. The patient’s history included taking immunosuppressant methotrexate and prednisone for the past 6 years due to psoriatic arthritis, an autoimmune condition. He also reported a palpable left axial lymph node following a COVID vaccine administration 6 months prior, which his primary physician advised closely monitoring.
The nurse practitioner, from the urgent care facility, ordered a superficial soft-tissue sonogram of the left neck, due to the patient’s left supraclavicular swelling and pain. A LOGIQ E9 (GE Healthcare, Wauwatosa, WI) was used with an ML6-15 MHz linear array transducer. The radiology report described markedly enlarged lymph nodes in the left supraclavicular region, the nodes of clinical concern, measured 2.4 × 1.4 cm, 2.3 × 1.4 cm, and 5.4 × 3 cm. These findings were reported as consistent with marked lymphadenopathy and a differential diagnosis of infectious and neoplastic cause was suggested (see Figures 1 and 2). The patient told the sonographer, at the time of the examination, that he was experiencing additional swelling and pain in his right neck and axilla. Further sonographic exploration of the contralateral neck and axilla was then performed. These findings also demonstrated multiple enlarged lymph nodes (see Figures 3 and 4). A CT of the chest was suggested for further evaluation and surveillance.
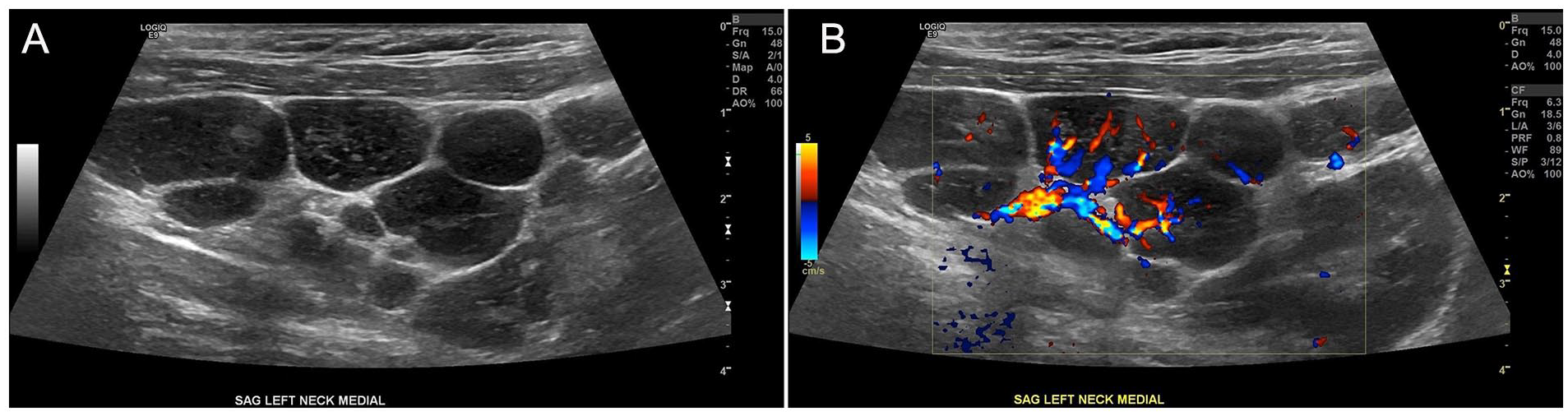
Sagittal sonographic view of lymph nodes in the left neck (A) without and (B) with color Doppler.
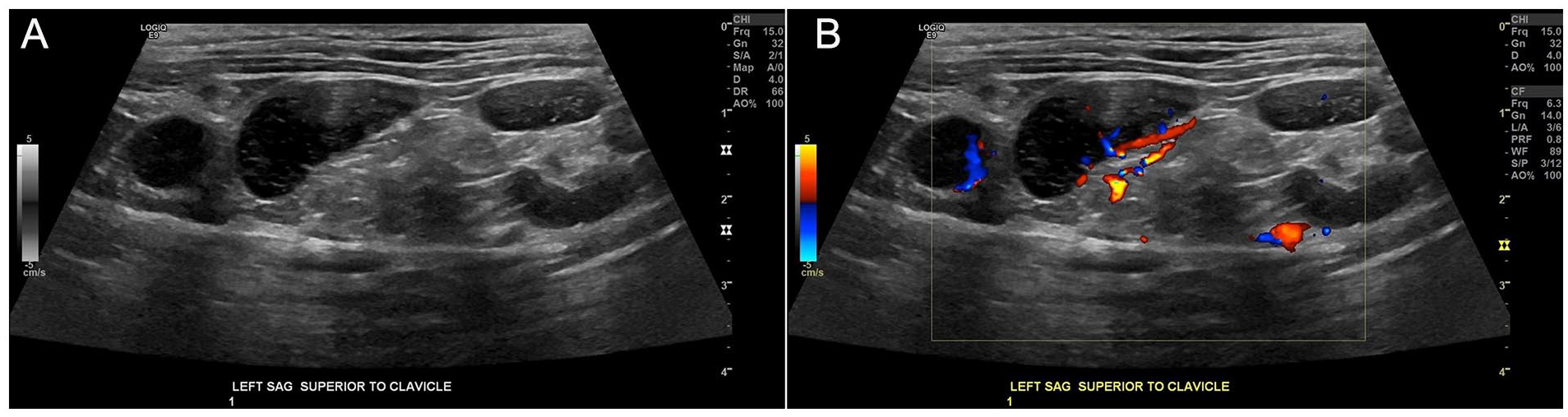
Sagittal sonographic view of lymph nodes in the left supraclavicular region (A) without and (B) with color Doppler.
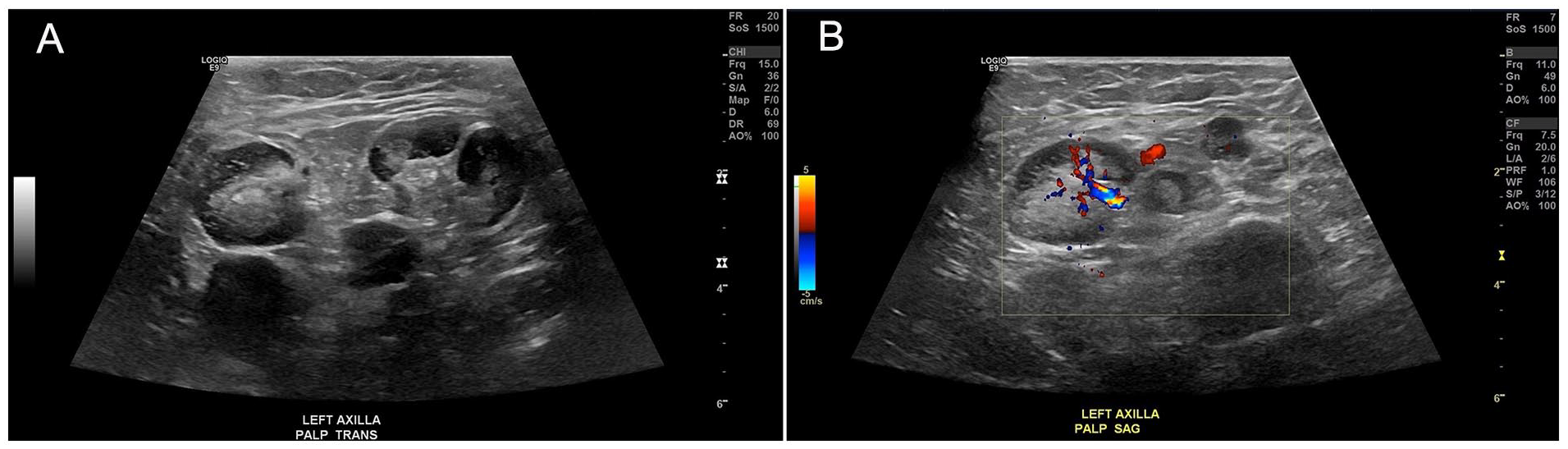
Sonographic transverse and sagittal views of the left axilla and the lymph nodes (A) without and (B) with color Doppler.
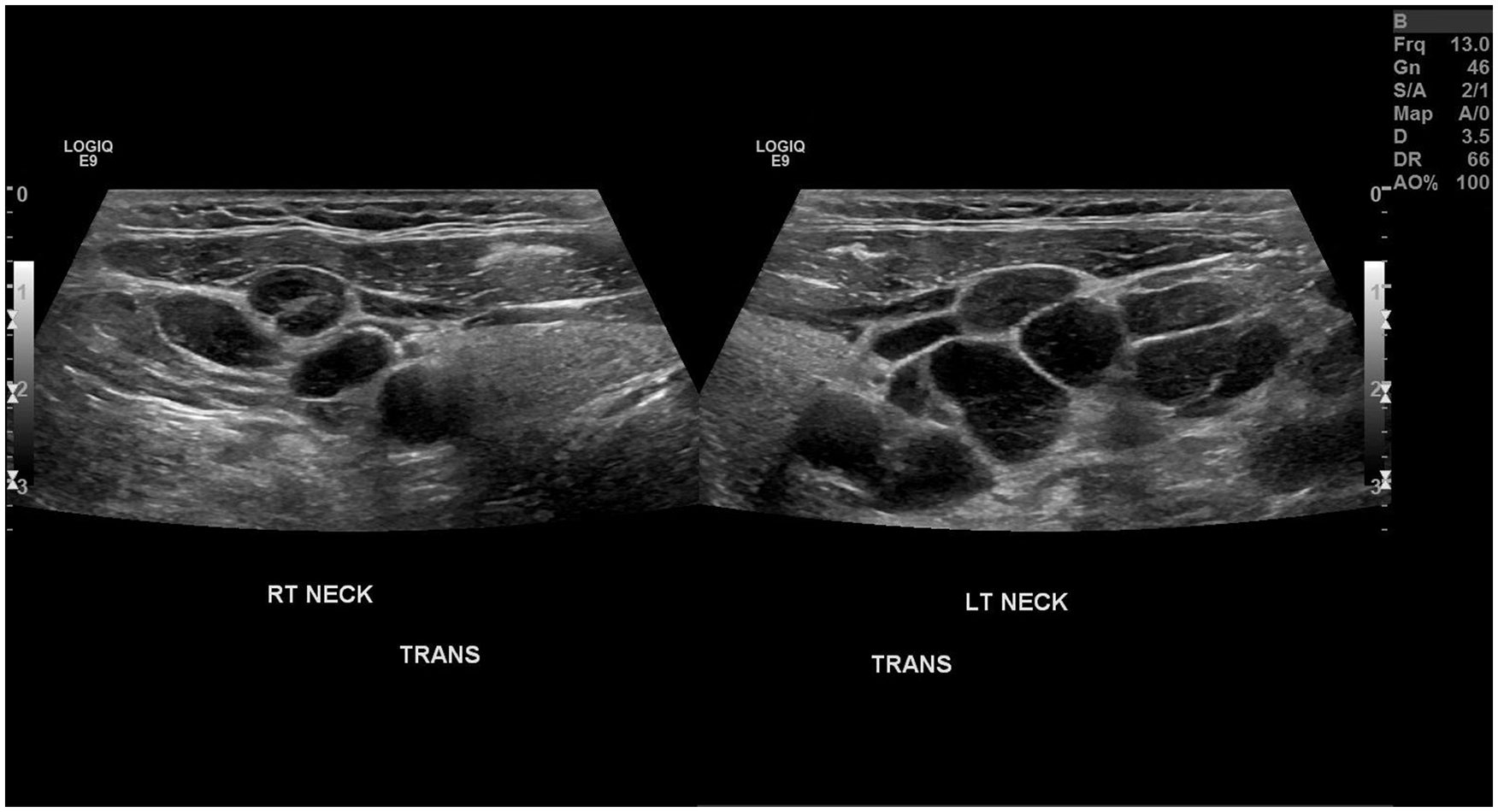
Dual transverse sonographic views demonstrating a comparison of the right and left neck.
A week later, the patient underwent a chest CT without contrast. The radiology report described extensive lymphadenopathy including the bilateral axillary, superior mediastinal, and retroperitoneal regions (see Figures 5 and 6). Limited CT imaging slices through the upper abdomen also revealed borderline splenic enlargement, measuring up to 13 cm. The overall impression suggested the possibility of lymphoma versus lymphocytic leukemia; therefore, biopsy was recommended.

Computed tomographic coronal image that demonstrates bilateral enlarged axillary lymph nodes. (Indicated by white arrows).
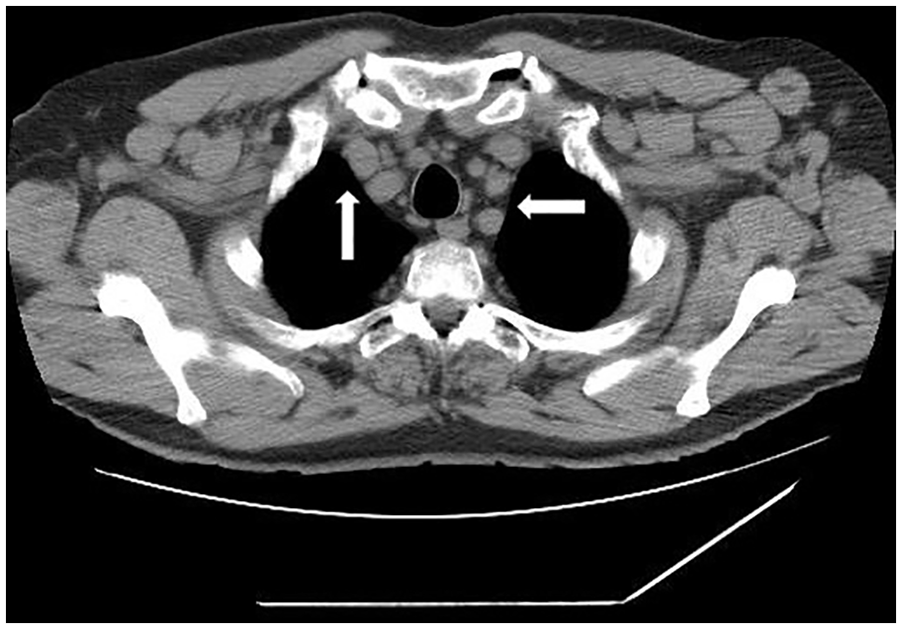
Computed tomographic axial image that demonstrates bilaterally enlarged axillary lymph nodes (Indicated by white arrows).
About 1 week later, the patient presented to the interventional radiology suite for an ultrasound-guided left neck biopsy. A targeted sonogram evaluation of the left neck was performed to localize the left cervical lymphadenopathy and to choose the appropriate needle entry and trajectory. The biopsy site was then prepped, with sterile technique, and the skin/subcutaneous tissues were anesthetized with lidocaine. Under sonography guidance, a 17-gauge double wall needle with trocar was advanced into a lymph node. An 18-gauge core biopsy device was inserted through the double-wall guidance, and a 2-cm core biopsy was obtained. This process was repeated for a total of 6 core biopsy samples. A postprocedure sonogram evaluation of the biopsy was performed. Based on the oncologist’s report, the histopathology findings revealed the samples were consistent with CLL and SLL.
The oncologist discussed the diagnosis, prognosis, and treatment options of CLL/SLL with the patient. Due to the toxicity effects associated with medications used to manage lymphoma, some of which can be life-threatening, it was decided that the risk factors of these options outweigh the benefits. It was chosen to monitor the patient’s condition carefully and pause active management.
Discussion
Chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL) are slow-growing cancers that affect lymphocytes and are one of the most common types of adult leukemia/lymphoma in Western countries. 1 More specifically, these cancers develop in abnormal B cell lymphocytes, which serve as functional units of the immune system that produce antibodies. CLL and SLL are considered different manifestations of the same entity because both diseases have identical histological patterns, the only difference between them being the location the cancer primarily occurs. The disease is classified as CLL when cancer cells are mainly in the blood and bone marrow, and SLL when the cancer cells are primarily in the lymph nodes. Clinically, patients with SLL exhibit tissue infiltration by CLL cells, which manifests as lymphadenopathy, hepatosplenomegaly, and other sites of extranodal lymph node invasion. 6
The epidemiology of the combined entity CLL/SLL shows increased rates of incidence in specific groups. Dores et al. found that the incidence of CLL/SLL was 90% higher among males. When evaluating the significance of race, 25% and 77% lower incidence rates were found among African-Americans and Asian/Pacific Islanders, respectively, when compared to Caucasians. 7 The occurrence of the disease also increases more steeply with advancing age and in immunocompromised patients. 8 Autoimmune conditions have been defined as a risk factor for the development of lymphoma, and the use of immunosuppressive medications is thought to play a significant role. 9
The clinical course of CLL/SLL can differ greatly between patients. While some can live for many years, others may experience rapid disease progression and death within 2 to 3 years after diagnosis. Richter’s syndrome, an aggressive transformation of CLL/SLL, is especially concerning and has a median survival rate of less than 1 year. 10 Symptoms of CLL/SLL are vague and may present differently depending on the location of the disease in the body at the time of diagnosis. Symptoms are indistinct and include hepatosplenomegaly, autoimmune cytopenias, peripheral lymphadenopathy, weight loss, frequent infections, anemia, fatigue, bruising easily, and night sweats. However, CLL/SLL are slow-growing cancers and many patients do not present with obvious symptoms of the disease. Up to 25% of patients with the disease can be asymptomatic; therefore, many of those affected may live for years without a diagnosis or knowledge of their condition. 6
The clinical staging of CLL/SLL is based on investigating lymph nodes, liver, and spleen, as well as laboratory findings. Massive splenomegaly is a sign of active disease. 11 According to the Ann Arbor classification, 80% to 90% of patients with CLL/SLL usually present with stage IV disease and involvement of extranodal sites is common, with the bone marrow being the most common site. 6 The disease has been reported to infiltrate various organs outside of the hematopoietic and nodal system, such as the gastrointestinal tract, lungs, liver, orbit, genitourinary system, and thyroid gland. 6 Sonography and CT are useful in the investigation of how enlarged lymph nodes are and if the spleen is also affected due to increased size. These imaging techniques complement one another and can confirm the locations of other affected areas in the body. The ACR Appropriateness Criteria suggests using sonography to differentiate between metastatic and benign neck masses and is considered an option for initial imaging. The advantages of sonography include the ability to be performed at the point of care and to expedite sampling; however, sonography can be limiting for a comprehensive evaluation of the deep spaces in the neck and for larger lesions. Contrast-enhanced CT is also recommended, and it has the advantage of superior spatial resolution. It allows for precise localization of the palpable finding and can locate the presence and distribution of abnormal lymph nodes and can refine the differential as a reactive or malignant process. 12
The treatment landscape of CLL and SLL has significantly changed over the years with advancements in medication therapy. Chemoimmunotherapy was previously the standard of care; however, the development of Bruton’s tyrosine kinase (BTK) inhibitors has now become the standard therapeutic option for CLL/SLL. 13 B cells function within the immune system by producing proteins called antibodies to neutralize the threat of a pathogen, or foreign substance. Since CLL/SLL develops in abnormal B cells of the immune system, the affected B cells cannot function properly. When CLL/SLL disrupts the B cell receptor, it causes the normal signaling pathway to malfunction, resulting in uncontrolled B cell reproduction. Bruton’s tyrosine kinase inhibitors disrupt the pathway of abnormal B-cells, preventing cell division and inducing cell death. 14 Although this treatment for CLL/SLL has the standard method of therapy, there are increased risks associated with the use of BTK inhibitors. Major cardiovascular side effects include atrial fibrillation, increased risk of bleeding, and hypertension. The choice to treat CLL/SLL with a BTK inhibitor requires a comprehensive discussion with the patient considering the benefits and risks, considering patient preference. 15
Conclusion
This case study of CLL/SLL is a suitable representation of the disease because of the patient’s clinical features. An older, Caucasian man, diagnosed with a pre-existing autoimmune disorder, and taking immunosuppressants for years, are all risk factors when considering CLL and SLL. When examining a suspicious case of leukemia or lymphoma using sonography, it is important to assess specific characteristics of unusual lymph nodes. These include their size, shape, echogenicity, and vascularity. In addition, given the disease’s impact on the spleen, size is a significant factor in diagnosing CLL/SLL. Since CLL/SLL often goes undiagnosed for years, due to its vague presentation of symptoms, sonography proved a useful role in the diagnosis of this case, due to the quick accessibility at the urgent care facility and the ability to thoroughly investigate the areas of concern. Sonography served as the primary technique in the sequence of events that lead to this patient’s diagnosis. From the sonographer obtaining a thorough exam of all areas of concern to guiding a biopsy needle into a lymph node, sonography was instrumental in this patient’s diagnosis and treatment.
Footnotes
Ethics Approval
Ethical approval was not sought for this study because as a case report, this is not considered research, and it does not include interaction with human subjects.
Informed Consent
Informed consent was not sought for this study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.