
Abstract
Background:
Marital status has been demonstrated to impact the outcomes of several malignancies. The prognostic role of marital status in chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) has not been determined.
Methods:
We identified 67,238 patients with CLL/SLL from the Surveillance, Epidemiology, and End Results (SEER) database. The patients were randomly divided into the training and validation cohorts. The univariate and multivariate Cox regression analyses were performed to screen the predictors for overall survival (OS) and disease-specific survival (DSS). The nomograms were developed and validated by the C-index, calibration curve, receiver-operating characteristic (ROC) curve, and decision curve analysis.
Results:
Marital status was an independent predictor of OS and DSS, with married patients having the best survival compared to single, divorced, and widowed patients. The nomograms for OS and DSS containing marital status were constructed, respectively. The C-index and ROC curve indicated that the models have favorable discrimination. The calibration curve showed good predictive accuracy. Decision curve analysis demonstrated considerable clinical net benefits. According to the points of the nomograms, patients were divided into three risk groups with distinct outcomes.
Conclusion:
Married marital status correlated with better survival in patients with CLL/SLL. The integration of marital status into validated nomograms provides a clinically accessible tool for improved risk stratification. Identifying widowed patients as a high-risk subgroup enables targeted interventions and optimized surveillance strategies in CLL/SLL management.
Plain language summary
Research shows life situations like marriage might affect cancer outcomes. We studied 67,238 chronic lymphocytic leukemia (CLL) patients from a national cancer database to understand how marriage and other social/economic factors affect survival. Patients were split into two groups for testing predictions. Using survival analysis methods, we found that married patients generally lived longer than single, divorced, or widowed patients. Other factors like age and race also affected survival. We created simple scoring tools to predict 5- and 10-year survival chances. The scoring tools showed good accuracy in predicting who might live longer, better predictions than basic methods, and practical value for doctors making treatment decisions. Patients were grouped into low, medium, and high risk categories based on their scores. Being married consistently linked to better outcomes. Our easy-to-use survival calculators could help doctors discuss prognosis with CLL patients while considering their personal circumstances.
Introduction
Chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) is a hematologic malignancy with clonal proliferation of mature B-cells. CLL/SLL affects more than 200,000 people and is associated with approximately 4410 deaths in the US annually. 1 Approximately 70% of patients with CLL/SLL are asymptomatic at initial diagnosis, and one-third never require treatment. 1 As for treatment, inhibitors of Bruton’s tyrosine kinase and B-cell lymphoma 2 have shown outstanding efficacy.2–4 Since CLL/SLL has a heterogeneous clinical course, many factors have been used to predict the time to first treatment or survival, such as β2-microglobulin, immunoglobulin heavy chain variable region mutation status, cytogenetics, and gene mutations.5–8 Recently, racial and socioeconomic disparities have been demonstrated as significant contributors to disparate outcomes in CLL/SLL. 9
Marital status is found to be correlated with the prognosis of both solid and hematologic tumors. In patients with skin malignancies such as melanoma and Merkel cell carcinoma, marital status is associated with stage, management, and survival.10–12
In acute myeloid leukemia, never-married and widowed patients have increased mortality. Similarly, patients living alone have lower survival than cohabitating patients. 13 Our previous study has demonstrated that married patients with mycosis fungoides (MF) have an earlier stage at diagnosis and longer survival compared with divorced or widowed patients. 14
In this study, we hypothesize that marital status influences CLL/SLL outcomes through multidimensional pathways, including treatment adherence, financial access to novel agents, and timely infection management via spousal support. We obtained data on patients diagnosed with CLL/SLL from the Surveillance, Epidemiology, and End Results (SEER) database and evaluated the impact of marital status on survival. Moreover, we developed and validated prognostic nomograms containing demographic, tumor, and socioeconomic characteristics.
Methodology
Data acquisition and patient selection
We extracted the data from the SEER database using the SEER*Stat software (version 8.4.3, National Cancer Institute, Bethesda, Maryland, USA). The dataset was SEER Research Data from 17 Registries based on a November 2023 submission. We included cases diagnosed with CLL/SLL (International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3) codes 9823/3) between 2000 and 2021. Exclusion criteria were as follows: (1) CLL/SLL was not the first primary malignancy; (2) cases that were diagnosed by autopsy or death certificate; (3) the marital status was unknown or separated, or having a domestic partner; (4) survival time was 0 or unknown; (5) the race record, median household income, cause of death, or rural-urban continuum code was unknown. A total of 67,238 eligible patients were included.
Predictors and outcomes
The following variables were defined as predictors: age, gender, race, year of diagnosis, subsequent malignancies (defined by the total number of in situ/malignant tumors for the patient), marital status, median household income, and rural-urban (defined by the rural-urban continuum code). Age was divided into three categories by the X-tile software (version 3.6.1, Yale University, New Haven, CT, USA; Supplemental Figure 1). Years of diagnosis were divided into two categories by the year 2014, when ibrutinib was approved for CLL/SLL. The primary endpoints of the study were overall survival (OS) and disease-specific survival (DSS). SEER defines OS as the interval between diagnosis and death of any cause, and DSS as the interval between diagnosis and death of CLL/SLL.
Model development and statistical analysis
The entire cohort was randomly divided into the training and validation cohorts in a 7:3 fashion. The Mann-Whitney test and chi-square test were used to compare the differences between the training and validation cohorts. The univariate and multivariate Cox regression analyses were performed to find the predictors associated with OS and DSS in the training cohort. The nomograms for predicting OS and DSS were constructed. The C-index, calibration curve, receiver-operating characteristic (ROC) curve, and decision curve analysis (DCA) were used to evaluate the nomograms’ efficacy in the training and validation cohorts, respectively. We divided patients into three different risk groups based on the points of the nomograms and plotted the Kaplan-Meier curves for OS and DSS, respectively. All the analyses were performed by the R software (version 4.3.3, R Foundation for Statistical Computing, Vienna, Austria). p < 0.05 (two-sided) was considered statistically.
Results
Baseline characteristics
A total of 67,238 eligible patients with CLL/SLL were included. There were 47,066 patients in the training cohort and 20,172 patients in the validation cohort. The demographic, tumor, and socioeconomic characteristics of the patients are shown in Table 1. The median age was 69 years, and the male/female ratio was approximately 1.5:1. Most patients were married (42,310, 62.9%), followed by widowed (10,666, 15.9%), single (8380, 12.5%), and divorced (5882, 8.7%). There was no difference in baseline characteristics between the training and validation cohorts (Table 1).
Baseline characteristics of the patients with CLL/SLL in the training and validation cohorts.

CLL/SLL, chronic lymphocytic leukemia/small lymphocytic lymphoma; IQR, interquartile range.
In total, 29,636 (44.1%) patients died of any cause, and the median OS was 120 months. The 5- and 10-year OS rates were 71.9% (95% CI: 71.5–72.2) and 49.7% (95% CI: 49.2–50.2), respectively. Of the entire cohort, 13,068 (19.4%) patients died of CLL/SLL, and the median DSS was not reached. The 5- and 10-year DSS rates were 86.1% (95% CI: 85.8–86.4) and 73.2% (95% CI: 72.7–73.7), respectively.
Prognostic significance of marital status
The prognostic significance of marital status and other factors was studied in the training cohort. Univariate analyses revealed that the predictors, including marital status, correlated with OS and DSS (Table 2). Compared to married patients, single (hazard ratio (HR) = 1.15, 95% CI: 1.10–1.20, p < 0.001), divorced (HR = 1.17, 95% CI: 1.12–1.23, p < 0.001), and widowed (HR = 2.33, 95% CI: 2.25–2.40, p < 0.001) patients had worse OS. Single (HR = 1.17, 95% CI: 1.09–1.25, p < 0.001) and widowed (HR = 2.08, 95% CI: 1.97–2.19, p < 0.001) patients also had worse DSS than married patients. However, no significant difference in DSS was observed between divorced and married patients (p = 0.139). In the multivariate regression, marital status retained independent prognostic significance of OS and DSS (Table 3). Compared to married patients, single (OS: HR = 1.34, 95% CI: 1.28–1.40, p < 0.001, DSS: HR = 1.32, 95% CI: 1.24–1.41, p < 0.001), divorced (OS: HR = 1.37, 95% CI: 1.28–1.40, p < 0.001, DSS: HR = 1.21, 95% CI:1.12–1.31, p < 0.001), and widowed (OS: HR = 1.38, 95% CI: 1.33–1.44, p < 0.001, DSS: HR = 1.36, 95% CI: 1.28–1.44, p < 0.001) patients had worse survival. The 5-year OS and DSS rates were 76.8% (95% CI: 76.3–77.4) and 88.4% (95% CI: 88.0–88.9) in married patients, 72.0% (95% CI: 70.7–73.3) and 85.6% (95% CI: 84.6–86.7) in single patients, 71.5% (95% CI: 70.0–73.0%) and 86.5% (95% CI: 85.3–87.7) in divorced patients, and 52.2% (95% CI: 51.0–53.4) and 75.4% (95% CI: 74.3–76.6) in widowed patients (overall p < 0.001).
Univariate analyses of predictors for OS and DSS in patients with CLL/SLL.

CI, confidence interval; CLL/SLL, chronic lymphocytic leukemia/small lymphocytic lymphoma; DSS, disease-specific survival; HR, hazard ratio; OS, overall survival.
Multivariate analyses of predictors for OS and DSS in patients with CLL/SLL.

CI, confidence interval; CLL/SLL, chronic lymphocytic leukemia/small lymphocytic lymphoma; DSS, disease-specific survival; HR, hazard ratio; OS, overall survival.
Development and validation of nomograms
According to the results of the multivariate regression, we created nomograms for OS and DSS to predict 5- and 10-year survival. The nomogram for OS was based on marital status, age, gender, race, year of diagnosis, subsequent malignancies, median household income, and rural-urban (Figure 1(a)). The nomogram for DSS was based on the same predictors, except for subsequent malignancies (Figure 1(b)).

Nomograms for predicting 5- and 10-year OS (a) and DSS (b) of patients with CLL/SLL.
The C-indexes of the nomogram for OS were 0.720 (95% CI: 0.717–0.724) and 0.721 (95% CI: 0.715–0.727) in the training and validation cohorts, respectively. The C-indexes of the nomogram for DSS were 0.719 (95% CI: 0.715–0.723) and 0.704 (95% CI: 0.695–0.713) in the training and validation cohorts, respectively. In the training cohort, the area under the curve (AUC) of ROC curves predicting 5- and 10-year OS were 0.750 and 0.759, respectively (Figure 2(a)). The AUC of ROC curves predicting 5- and 10-year DSS were 0.722 and 0.714, respectively (Figure 2(b)). In the validation cohort, the AUC of ROC curves predicting 5- and 10-year OS were 0.747 and 0.753, respectively (Figure 2(c)). The AUC of ROC curves predicting 5- and 10-year DSS were 0.720 and 0.713, respectively (Figure 2(d)). These results indicated that the models have favorable discrimination. Calibration curves showed good concordance between the predicted 5- and 10-year OS and DSS with the actual survival in both the training and validation cohorts (Figure 3(a)–(d)). DCA demonstrated considerable clinical net benefits for the 5- and 10-year survival prediction (Figure 4(a)–(d)).

Receiver-operating characteristic curves of the nomograms predicting 5- and 10-year OS and DSS in the training cohort: (a) OS, (b) DSS and validation cohort: (c) OS, (d) DSS.
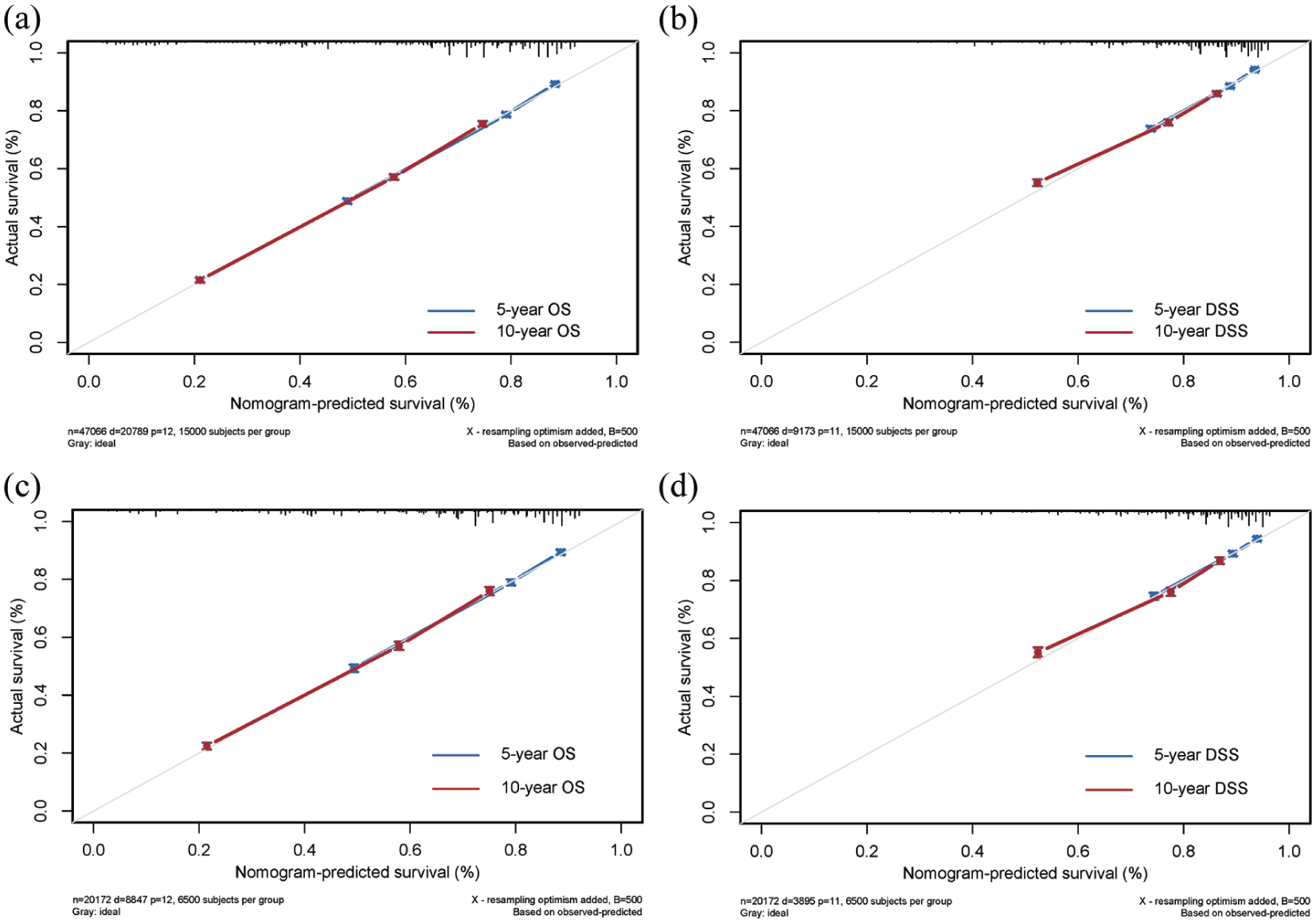
Calibration curves of the nomograms predicting 5- and 10-year OS and DSS in the training cohort: (a) OS, (b) DSS and validation cohort: (c) OS, (d) DSS.

Decision curve analysis of the nomograms predicting 5- and 10-year OS and DSS in the training cohort: (a) OS, (b) DSS and validation cohort: (c) OS, (d) DSS.
Risk stratification based on nomograms
Based on the nomograms predicting OS and DSS, we calculated the optimal cutoff values of total points using X-tile software and divided the patients into three risk groups (Supplemental Figure 2). In the training cohort, the 5-year OS and DSS rates were 86.3% (95% CI: 85.9–86.8) and 93.5% (95% CI: 93.2–93.9) in the low-risk group, 67.7% (95% CI: 66.8–68.5) and 83.0% (95% CI: 82.4–83.6) in the intermediate-risk group, and 36.4% (95% CI: 35.3–37.5) and 65.8% (95% CI: 64.4–67.2) in the high-risk group (p < 0.001, Figure 5(a) and (b)). The validation cohort had similar results, as the 5-year OS and DSS rates were 86.4% (95% CI: 85.7–87.1) and 94.1% (95% CI: 93.5–94.7) in the low-risk group, 68.1% (95% CI: 66.8–69.3) and 85.8% (95% CI: 85.0–86.6) in the intermediate-risk group, and 36.2% (95% CI: 34.5–38.0) and 66.2% (95% CI: 64.3–68.3) in the high-risk group (p < 0.001, Figure 5(c) and (d)).

Survival curves of different risk groups classified by the nomograms in the training cohort: (a) OS, (b) DSS and validation cohort: (c) OS, (d) DSS.
Discussion
While marital status broadly predicts survival across diseases as a socioeconomic proxy, its prognostic value in CLL/SLL, a disease with distinct management challenges, was unconfirmed. By analyzing patients with CLL/SLL from the SEER database, we found that unmarried marital status (single, divorced, and widowed) was an independent adverse predictor for OS and DSS in CLL/SLL. In addition, we demonstrated that other socioeconomic factors were prognostic in patients with CLL/SLL. Based on marital status and other socioeconomic, demographic, and tumor characteristics, we developed prognostic nomograms and validated these nomograms internally. The C-index, ROC curves, calibration curves, and DCA showed robust discrimination and favorable clinical utility of the models for predicting the survival of patients with CLL/SLL. In addition, patients were divided into different groups with distinct outcomes according to the nomograms. Our study provided a novel prognostic tool consisting of socioeconomic factors for patients with CLL/SLL.
In this study, we demonstrated that marital status was a robust predictor for the survival of patients with CLL/SLL, with married patients exhibiting significantly better outcomes. Building upon Cohen’s Social Support Theory, 15 we propose that the observed survival advantage operates through three disease-specific pathways: (1) Instrumental support via spousal care coordination enhances adherence to medical care.16,17 It should be noted that sustained medication adherence is even more important for disease control in CLL/SLL in the era of novel agents 18 ; (2) emotional support buffers psychological distress known to trigger immune dysregulation, 19 particularly relevant given >10% of CLL patients experience moderate-severe depression, and marital status was correlated with depression. 20 It was reported that emotional support from caregivers contributes to better outcomes following hematopoietic stem cell transplantation 21 ; (3) structural support through combined financial stability and insurance optimization enables access to high-cost therapies, while sustaining healthier lifestyles.22–25 These factors may also help explain the independent prognostic contributions of income and rural-urban disparities observed in our study. Future studies should develop integrated models quantifying the joint effects of marriage and other demographic factors.
Marital status has been demonstrated to be a prognostic factor for different types of cancers, including hematological malignancies. In a recent study, marital status was demonstrated to be a prognostic factor for primary lymphoma of the male genital tract. 26 According to the study by Zhang et al., married patients with mantle cell lymphoma have better OS and DSS than unmarried patients. 27 A study from our group also showed that married status was associated with an earlier stage and better outcomes in patients with MF. 14 These studies highlighted the importance of marital status in the prognostication of patients with hematological malignancies.
The most commonly used prognostic model for CLL/SLL is the CLL International Prognostic Index (CLL-IPI), which includes age, stage, β2-microglobulin, immunoglobulin heavy chain variable region (IGHV) mutational status, and TP53 status. CLL-IPI is robust in predicting survival for CLL patients receiving chemoimmunotherapy. 6 However, in the era of novel agents, the impact of CLL-IPI in predicting OS appears to be not significant.6,28 Efforts have been made to construct new prognostic models based on multiple technologies, such as whole-genome sequencing, flow cytometry immunophenotyping, and optical genome mapping.29–31 However, these models did not include socioeconomic factors. In this study, we demonstrated that marital status and several other socioeconomic factors have significant impacts on survival in CLL patients. Furthermore, a nomogram based on these socioeconomic factors could efficiently predict the outcomes of patients with CLL. These findings suggest the incorporation of socioeconomic factors into prognostic tools for CLL in the future.
Our study has several clinical implications. Our findings suggested that the survival of unmarried CLL patients needed to be improved. Therefore, more social support from the healthcare system or the community needs to be provided to unmarried patients. And psychological intervention may be useful. Similarly, for the high-risk patients based on the prognostic nomogram, more social support and psychological intervention may be helpful to improve the outcomes. Enrollment of these patients into clinical trials could be potentially useful due to the free access to the medications and more regular follow-up.
Our study has several limitations. Treatments were not included in the analysis as we could not access the treatment information. External validation was not performed in this study. Moreover, as clinical stages and molecular features were not available, we did not include these important parameters in the prognostic nomogram. In addition, a priori power analysis for sample size calculation was not conducted due to the retrospective utilization of the SEER database. Further prospective and multicenter studies are needed to verify our results. And it is better to include clinical stages and molecular features to refine the current prognostic nomogram in the future.
Conclusion
In conclusion, we emphasize the prognostic significance of marital status in patients with CLL/SLL. By combining marital status with other demographic and socioeconomic factors, we construct clinically feasible nomograms that are robust in predicting the survival of patients with CLL/SLL. Further prospective studies are warranted to validate the prognostic role of marital status for patients with CLL/SLL.
Supplemental Material
sj-doc-1-tah-10.1177_20406207251379683 – Supplemental material for Prognostic impacts of marital status and other socioeconomic factors in patients with chronic lymphocytic leukemia: an analysis of SEER database
Supplemental material, sj-doc-1-tah-10.1177_20406207251379683 for Prognostic impacts of marital status and other socioeconomic factors in patients with chronic lymphocytic leukemia: an analysis of SEER database by Jing Zhang, Ping Liu, Yilian Yang, Yeqin Sha, Lei Fan, Jianyong Li and Yi Miao in Therapeutic Advances in Hematology
Supplemental Material
sj-docx-2-tah-10.1177_20406207251379683 – Supplemental material for Prognostic impacts of marital status and other socioeconomic factors in patients with chronic lymphocytic leukemia: an analysis of SEER database
Supplemental material, sj-docx-2-tah-10.1177_20406207251379683 for Prognostic impacts of marital status and other socioeconomic factors in patients with chronic lymphocytic leukemia: an analysis of SEER database by Jing Zhang, Ping Liu, Yilian Yang, Yeqin Sha, Lei Fan, Jianyong Li and Yi Miao in Therapeutic Advances in Hematology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.