
Abstract
The Morel-Lavallée lesion (MLL) is an uncommon, traumatic internal degloving injury of the soft tissues and the fascia. The MLLs are often misdiagnosed or delayed in being diagnosed due to the severity of other injuries from an accident. Sonography and/or magnetic resonance imaging may be used to confirm the diagnosis. After the MLL is diagnosed, treatment options vary from conservative options to surgical methods depending on the chronicity of the lesion. The case study presented occurs in the most common site for the injury, the hip and pelvis.
Keywords
Morel-Lavallée lesion (MLL) is a rare soft tissue shearing injury occurring after a traumatic incident. Since sonographers work in many other imaging settings other than trauma centers, general sonographers need to have awareness of MLLs and their sonographic features.
The MLL’s mechanism of injury is a shearing force that separates the subcutaneous tissue layer from the deeper fascial layer creating a potential space. These layers are traversed by blood and lymphatic vessels which are damaged and begin to fill a newly created space.1 –5 The MLLs have the potential to fill with blood, lymphatic/serous fluid, and fatty tissue.1,2 These components are easily identified with sonography which makes it an ideal imaging technique for diagnosis of this pathology.
Case Report
A 66-year-old woman was referred to the sonography department to evaluate right lateral hip pain and swelling, after a motor vehicle accident (MVA), 2 months prior. The patient’s car was hit from behind, and the patient had been hospitalized recovering from a fractured humerus, pneumothorax, and facial lacerations. After she was discharged from the hospital, the patient noticed lateral right hip swelling and pain. The patient underwent sonography of the area of pain and swelling. The sonogram demonstrated a large subcutaneous fluid collection measuring 11.4 cm in its largest dimension, with internal septations and fat globules, indicative of an MLL (see Figures 1–4). After the diagnosis, the patient was scheduled for a clinic visit to discuss treatment options. An ultrasound-guided aspiration/drainage of the right hip MLL was scheduled, followed by sclerotherapy, with doxycycline medication. The patient returned to the sonography department 5 weeks after the initial sonography for the treatment plan. The patient was consented, universal time-out completed, and the subcutaneous local anesthetic was given. Using ultrasound guidance, the needle was positioned into the fluid collection, connected to an evacuated bottle, and 120 mL of serosanguineous fluid removed (see Figure 5). The evacuated bottle and tubing were disconnected with the needle remaining in the decompressed space (see Figure 6). The doxycycline injection was administered to complete the sclerotherapy portion of the examination (see Figure 7). After the needle was removed, the entry site was covered with a compression bandage, and the area of prior swelling was wrapped with a compression bandage.
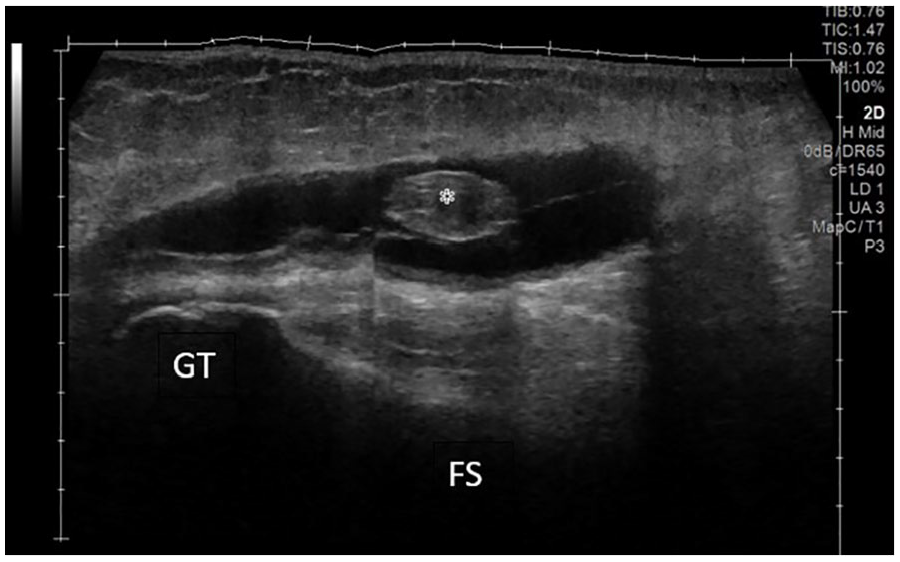
A panoramic longitudinal view of the Morel-Lavallée lesion at the area of the right lateral hip. The fluid collection contains internal septations and a fat globule (denoted with *). This area was imaged with a linear transducer. FS, femoral shaft; GT, greater trochanter of the femur.

A transverse sonographic view of the Morel-Lavallée lesion at the area of the right lateral hip. The fluid collection is shown with internal septations and fat globule (denoted with *). This area was imaged with a curvilinear transducer.
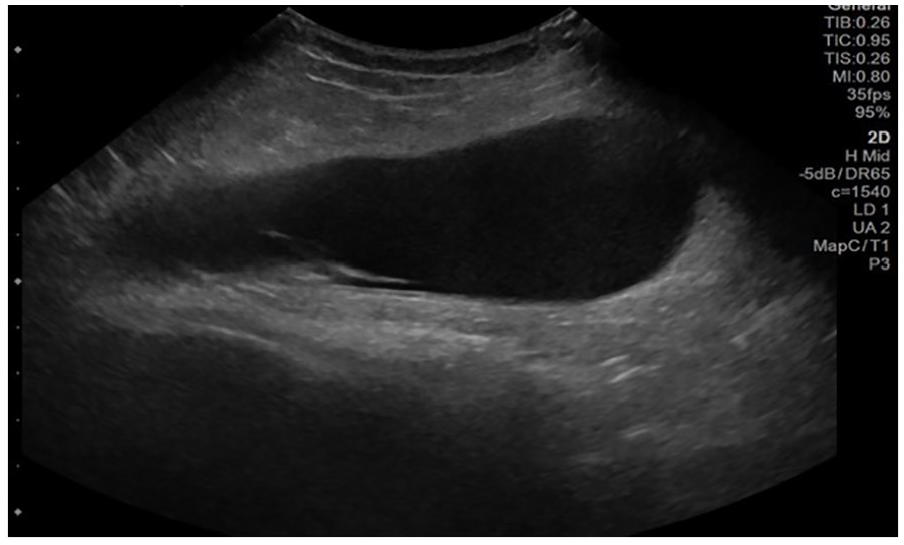
A longitudinal view of the Morel-Lavallée lesion at the area of the right lateral hip. In this view, the fluid collection continues to demonstrate internal septations. This area was imaged with a curvilinear transducer.
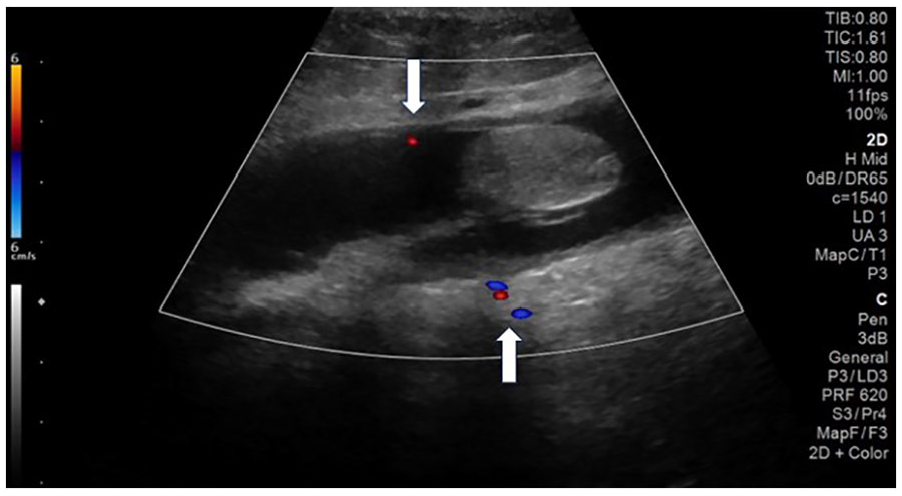
A longitudinal view of the Morel-Lavallée lesion at the area of the right lateral hip. Color Doppler was used to demonstrate blood vessels both anterior and posterior to the lesion (see white arrows). This area was imaged with a linear transducer and a trapezoid field of view.
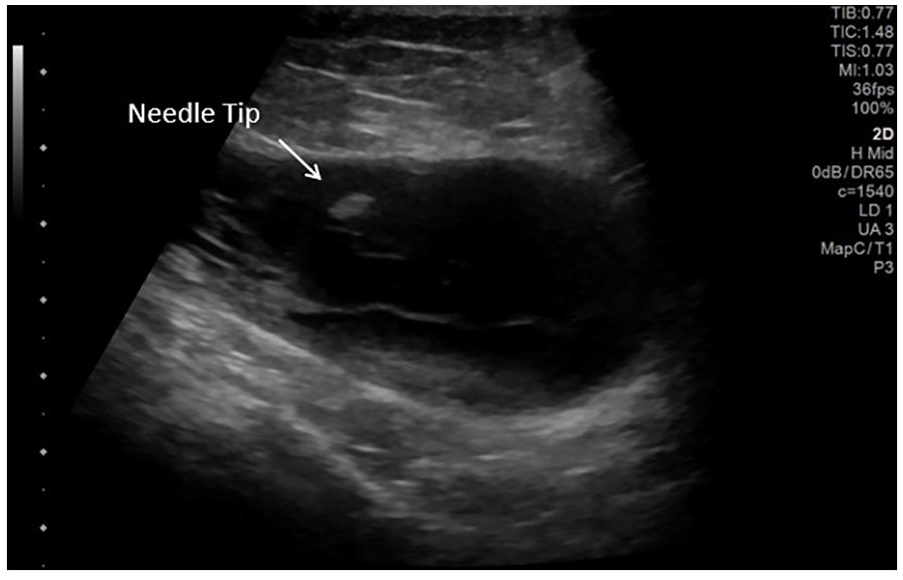
A longitudinal view of the Morel-Lavallée lesion with needle tip in the fluid collection. This area was imaged with a linear transducer with a trapezoid field of view. (The echogenic needle tip is denoted by the white arrow).
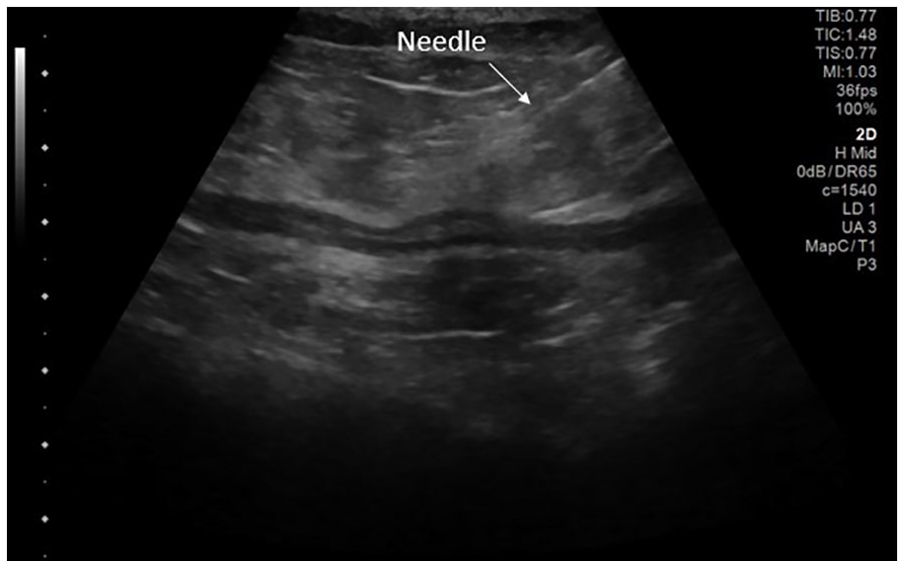
A longitudinal image of decompressed Morel-Lavallée lesion, with the needle remaining in the cavity. This area was imaged with a linear transducer with a trapezoid field of view (The echogenic needle is denoted by a white arrow).
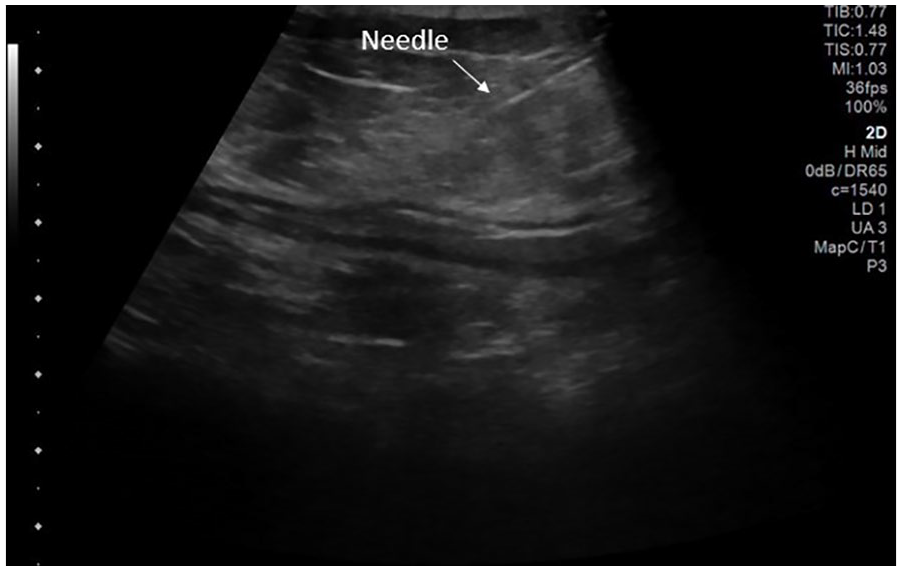
A longitudinal image of the decompressed Morel-Lavallée lesion with doxycycline injected for sclerotherapy. This area was imaged with a linear transducer with a trapezoid field of view (The echogenic needle is denoted by a white arrow).
Two months after the percutaneous drainage of the MLL with doxycycline injection, the patient presented for a surgical consult, for right lateral hip swelling. It was noted by the patient and family that the swelling appeared to have decreased in size from the initial sonogram. For imaging evaluation of the area, the surgeon ordered a computed tomogram of the pelvis without contrast, which demonstrated a 6.4-cm suspected proteinaceous right lateral hip fluid collection and macroscopic fat globules (see Figure 8). With the current diagnostic finding, the patient continued to await surgical treatment of the MLL, in the hopes of a positive outcome and resolution of her right lateral hip swelling.

A coronal computed tomographic image of the pelvis that demonstrated the reoccurrence of the Morel-Lavallée lesion. A fluid collection is denoted by a single white arrow and the fat globules within the collection are identified with a double white arrow.
Discussion
The MLL is a rare pathology that was first described in the mid 1800s. 2 It occurs after a traumatic incident (MVAs, falls, sports injuries, and seat belt injuries) 2 where the subcutaneous soft tissues are separated from the deeper fascial layer creating a potential cavity. These layers contain vasculature that is disrupted and fills the space with fluid and fat.2,4,5
As with this case study, the most common site for this closed internal degloving injury is the trochanteric area of the hip. 3 It accounts for more than 60% of MLLs. 6 The reason for the susceptibility of the lateral hip area is the soft tissues are especially mobile compared with the deep fascial layers and have ample blood supply which aids in the creation of an MLL.2,3 Even though it is commonly seen in the hip, this pathology can occur in other areas including the lower back, knee, upper extremity, and posterior cranium.2,4
Patients present with signs and symptoms of swelling, pain, and occasionally bruising after trauma.4,6 Due to the severity of other injuries from the trauma, MLLs can have a delayed diagnosis or misdiagnosis.3,6 Kottmeir et al reported that MLLs are diagnostically missed up to 44% of the time. 1 Furthermore, up to 33% cases have delayed signs and symptoms due to a gradual progression of swelling. 6 This gradual progression underscores the importance for general sonographers’ to be aware and document this pathology, so as not to delay diagnosis and treatment.
Delayed diagnosis and treatment of MLLs can cause an inflammatory response in the soft tissues and form a fibrous capsule around the fluid.1,4,6 This capsule is thought to inhibit the absorption of the fluid and aids in the re-accumulation of fluid after percutaneous drainage as was seen with the present case.1,2,4,6
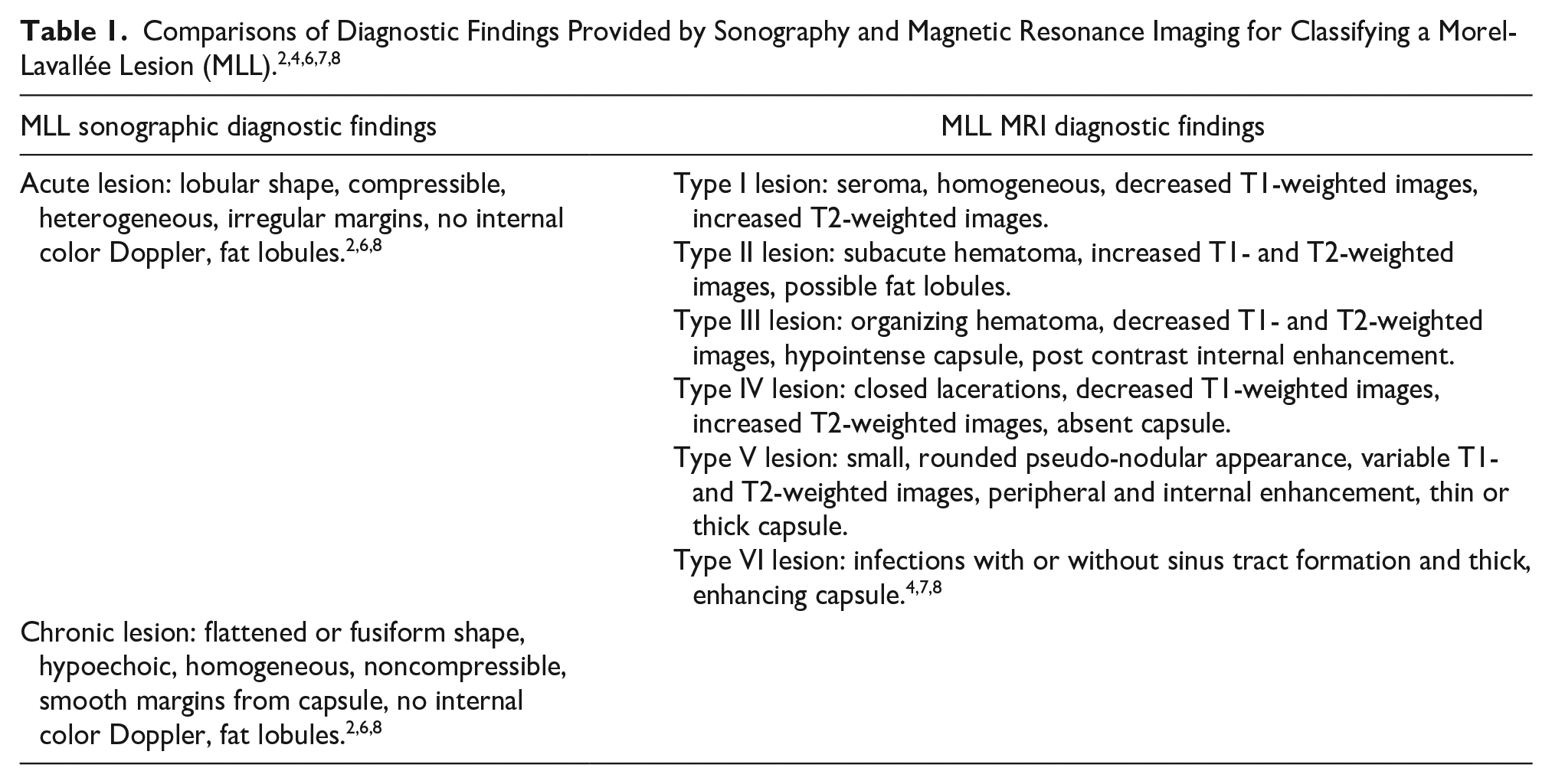
During the sonography examination, the location of the swelling is evaluated, and the lesion is characterized. The lesion’s location can be identified between subcutaneous and fascial layers, and it may demonstrate heterogeneity, irregular borders, absent color Doppler flow, and can be compressible in the acute phase.2,3,4,5,6 The MLLs will also have echogenic fat globules in the lesion which differentiates it from bursitis or hematoma.2,4,5 With sonography, chronic lesions appear more hypoechoic and have well-defined, smooth borders from the fibrous capsule.2,3 The acute and chronic sonographic findings of MLLs are summarized in Table 1.
Treatment options vary on the chronicity of the MLL. If an MLL is untreated, it has the potential to become infected and lead to skin necrosis. 4 Due to potential complications, it is important for the correct treatment plan to be chosen. If the lesion is diagnosed in the beginning stages without the fibrous capsule, conservative treatment methods may be used including compression, nonsteroidal anti-inflammatory drugs, and physical therapy.2,4,6 If a capsule has already formed, the treatment options change and may range from interventional percutaneous drainages with or without sclerotherapy and compression to open surgical excision.2 –4,6 In the present case, the percutaneous drainage with doxycycline of the MLL is unsuccessful, and a surgical consult was provided to establish future surgical treatment.
There are multiple imaging techniques for diagnosing an MLL and the most common are sonography and magnetic resonance imaging (MRI). The MRI is considered as the diagnostic gold standard for imaging this pathology and the surrounding soft tissues. The MRI gives more detailed information about the location between the different fascial layers, and it has its own classification system of MLLs developed and proposed by Mellado and Bencardino.2 –4,6 The MRI classification system, summarized in Table 1, is based on several criteria including the lesion’s shape, MRI signal characteristics, MRI signal enhancement, and capsule presence or absence.4,7 From the criteria, six types of lesions are described in the literature ranging from seroma-like to infected with or without sinus tract.4,7
Although MRI is the preferred imaging technique, it is expensive and can be less accessible. 2 In contrast, sonography is more cost-effective and easily provided to a trauma patient, due to its portability. Sonography can be used in any phase of care but especially during the acute phase when a patient may be unable to obtain an MRI. 3 With sonography, the challenge is an inherent operator dependence especially in the lack of knowledge of musculoskeletal pathologies.
Conclusion
An MLL is an uncommon pathology that results from a traumatic incident. It requires a quick accurate diagnosis, but the diagnosis is often delayed or overlooked, due to the focus on more severe injuries acquired during an accident. With the delayed diagnosis, treatment options vary on their effectiveness, and the outcomes for the patient may be less desirable. With the advantages of sonography and an experienced sonographer and radiologist, the diagnosis may be made quickly and improve a patient’s long-term outcomes.
Footnotes
Ethics Approval
Ethical approval was not sought for the present study since it did not comprise of a research study. The case study presented is for educational purposes only.
Informed Consent
Written informed consent was obtained from all subjects before the study.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.