
Abstract
In cases of traumatic death, precise injury evaluation is crucial for both legal and medical reasons. In the modern era, many scholarly articles recommend postmortem computed tomography (PMCT) instead of routine postmortem practices. This case report compares the findings of PMCT with those of conventional autopsy methods for assessing blunt traumatic injuries. In this case, we received the body of a 16-year-old male who died due to a road traffic accident. Before performing a routine postmortem examination, we performed CT imaging to compare the findings with those of routine procedures. This report highlights the significance of the conventional postmortem approach in identifying soft tissue and bony injuries that are undetectable by imaging techniques. While CT imaging offers noninvasive visualization of injuries, manual examination remains essential for identifying specific injuries, particularly those affecting soft tissues. The combination of CT imaging and conventional autopsy procedures strengthens the precision and dependability of forensic evaluations in cases of traumatic death, especially in intricate situations involving multiple wounds. Recognizing the advantages and constraints of these methods is vital for advancing forensic inquiries and improving legal outcomes in medical contexts.
Introduction
In the event of traumatic death, precisely identifying the cause and characteristics of injuries is essential for both legal and medical reasons. Autopsies are instrumental in this process as they offer in-depth information about the nature and severity of injuries sustained by individuals, which can be crucial for legal inquiries. 1 Postmortem imaging, particularly computed tomography (PMCT), can offer crucial insights to guide conventional autopsies. This approach enables forensic pathologists to concentrate on specific regions of interest, potentially shortening the duration of the autopsy process. PMCT is especially adept at revealing bone injuries, detecting foreign objects, and identifying gas distributions within the body. These capabilities make it particularly beneficial in examining cases involving physical trauma, such as those resulting from car crashes or firearm-related incidents.2,3 While conventional autopsy is generally considered the most reliable method for postmortem examination, preliminary findings suggest that PMCT could potentially improve the ability to visualize internal injuries and aid in the forensic investigation of trauma-related deaths. 4 However, there are limitations to the effectiveness of PMCT. It is less successful in detecting soft tissue injuries and can produce false-positive and false-negative results for intracranial and intraperitoneal hemorrhages. 5 Therefore, the claim of PMCT’s superiority in traumatic death cases is not conclusively supported and should be considered within the context of its specific advantages and limitations. 6 In this case report, we aimed to assess the advantages and disadvantages of postmortem imaging compared with conventional autopsy techniques for evaluating injuries caused by road traffic accidents. Our objective is to gain a better understanding of the strengths and limitations of these methods.
Case report
A 16-year-old male’s body was received for a postmortem examination, and his death was reportedly caused by a road traffic accident. On external examination, abraded bruises were noted over the left side of the cheek and chin. On the left side, a laceration of the ear auricle measuring 2 × 1 cm with complete transection and a laceration measuring 5 × 3 cm exposing the underlying bone were noted behind the left ear auricle involving the parietal-temporal area (Figure 1). An area of abrasion measuring 5 × 3 cm was present over the lower right side of the chest at the level of the anterior axillary line, involving the surface areas of the seventh and eighth ribs. Before dissection and internal examination of the body, an NCCT/PMCT scan (noncontrast thin contagious helical MDCT section) of the head, chest, and abdomen was performed using the GE Optima 128 slice CT scanner. The results revealed an ear laceration with a linear displaced fracture of the right parietal bone extending to the mastoid part of the temporal bone (Figure 2). The radiologist also found a right pneumothorax associated with a displaced fracture on the right side of the ninth rib (Figure 3). Mild free fluid was noted over the right pleural cavity with an average HU density of 40–45, suggesting a hemothorax. Abdominal examination revealed mild-to-moderate free fluid in the hepatorenal space and posteroinferior part of the spleen with an average HU density of 50–60, suggestive of hemoperitoneum. Multiple air foci were observed over the right lobe of the liver (Figure 4). PMCT was conducted by a professor and a resident from the Radiology Department. After completion of the PMCT, dissection of the body was performed as part of the conventional autopsy. After dissecting the scalp tissue, we found a linear displaced fracture over the right side of the skull involving the temporoparietal region. Upon skin and subcutaneous tissue removal, no extravasation of blood was noted over the anterior chest wall, except for the anterior axillary line over the seventh to ninth ribs (Figure 5). All the ribs were fractured underneath. Water was poured between the skin and chest wall on both sides, and an intercostal space was punctured under the water level to check for air bubbles and rule out pneumothorax, while the right side showed a positive result (Video 1). This procedure is a routine practice in traumatic death cases. After opening the chest cage and abdominal wall, we found 150 ml of blood in the right pleural cavity and 1600 ml in the peritoneal cavity. The intima of the descending aorta showed multiple transverse partial-thickness tears at the T6-7 vertebrae (Figure 6). The fractured ribs produced lacerations over the diaphragm and extended to the right lobe of the liver. This caused two transverse lacerations, measuring 7 × 1 × 1 cm and 3 × 2 × 1 cm, over the anterior surface of the right lobe (Figure 7). We noticed total separation of the liver at the falciform ligament, which led to detachment of the left lobe from the right lobe and resting behind the stomach (Figure 8). As per postmortem surgeons’ opinion, the cause of death was sustained injury to the liver, leading to hypovolemic shock.

Laceration of the ear with underneath fracture.

PMCT image of ear laceration and fracture of the skull.

PMCT image of rib fracture.

PMCT image of the liver with the presence of multiple air foci.

Fracture of ribs.

Intimal tear of descending aorta.

Lacerations over the right lobe of the liver.

Separation of the right and left lobe of the liver.
Discussion
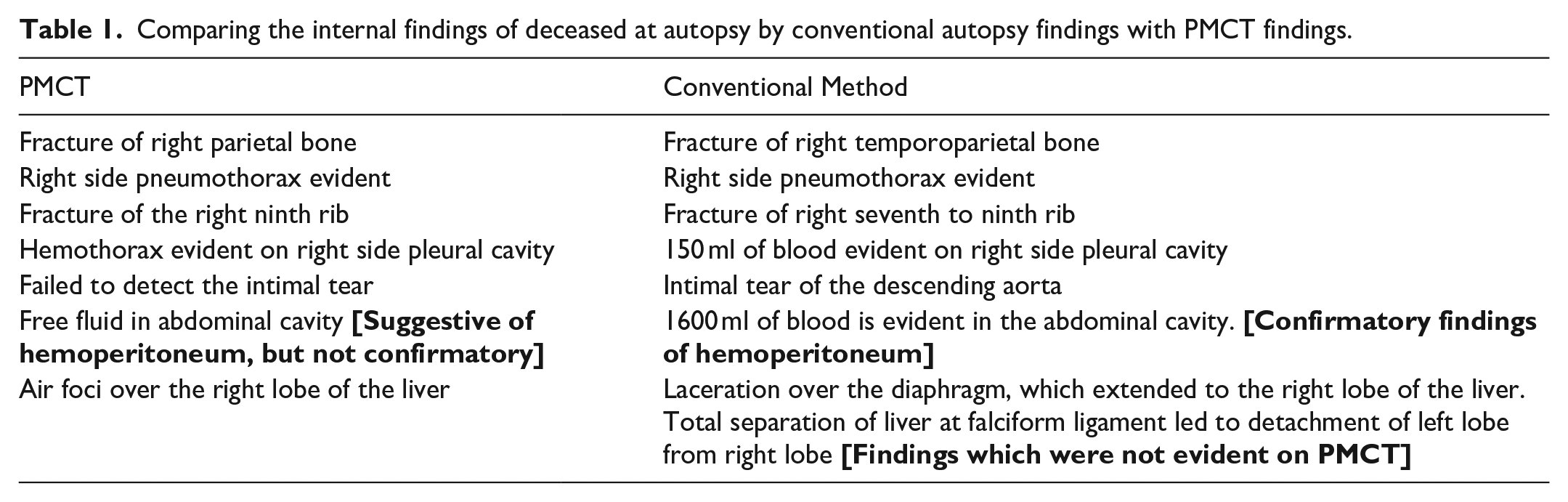
PMCT demonstrates limited effectiveness in distinguishing between soft tissue injuries and identifying vascular abnormalities, particularly when examining deaths from natural causes. Notably, while PMCT excels at detecting bone-related injuries, it is less effective than traditional autopsy methods in identifying findings related to organs, soft tissues, and blood vessels, especially when it comes to minor injuries.7–9 Raj VK, et al.’s research suggest that whole-body PMCT followed by regionwise CT may be a more effective method for acquiring PMCT and detecting soft tissue injury findings with greater precision. They also suggested that PMCT could determine the cause of death more scientifically than traditional autopsy. 10 Kruc et al. revealed that PMCT is a highly effective method for diagnosing skull and other bone fractures, particularly gunshot wounds, compared to routine autopsy. However, a conventional autopsy is better suited for detecting minor injuries to organs and soft tissues and fractures on the base of the skull. 11 Similarly, in this case, PMCT failed to detect soft tissue injuries, such as aortic intimal tears, diaphragmatic laceration, separation of the liver lobe, amount of blood in the peritoneal cavity, and fracture of the seventh rib on the right side, even though it was conducted using a high-end CT instrument and two senior radiologists were involved (Table 1). According to Re et al., PMCT is generally superior to conventional autopsy for detecting pneumothorax or gas embolism. 7 However, in the present case, the authors found pneumothorax over the right side of the chest cavity on PMCT, which was successfully demonstrated on conventional autopsy. Although the expenses and accessibility of CT scanners and personnel are the primary constraints of PMCT screening before the conventional autopsy, it is essential to recognize that not all forensic departments possess their own CT scan setup. 7 However, numerous Indian authors have promoted the use of PMCT in cases of traumatic death rather than the conventional approach. On the other hand, as of 2023, the Indian government’s healthcare spending amounted to 2.6% of the nation’s gross domestic product, significantly lower than the allocations made by other developing nations.10,12 For nations with constrained healthcare budgets, such as India where only 2.6% of GDP is allocated to healthcare, prioritizing essential medical services may be more crucial than investing in advanced forensic technologies. In resource-scarce environments, basic healthcare provisions might offer greater value for money compared to costly PMCT equipment.
Comparing the internal findings of deceased at autopsy by conventional autopsy findings with PMCT findings.
Conclusion
This case report compares the findings obtained using PMCT with those obtained through traditional autopsy, highlighting the significance of the conventional technique in relation to PMCT. Despite PMCT's failure to detect soft tissue injuries and fractures, multiple literature mentioned that it offers a higher sensitivity than the conventional technique. According to the authors, it is advisable not to abandon practical and suitable older methods or approaches to pursue technological progress.
Footnotes
Acknowledgements
None.
Authors contributions
Dr Arijit Datta was very keen and focused on conceptualizing ideas in the study design, interpreting the data, and reviewing the manuscript. Dr Darshan Galoria contributed to data analysis, drafting, and reviewing portions of the manuscript. Dr Sridhar Dave contributed to the radiographic image interpretation, drafting, and manuscript review. Dr Preeti Tiwari was instrumental in reviewing the manuscript. Dr Srushti Shukla was instrumental in literature review and drafting. Dr Viral Patel contributed to the radiographic image interpretation and manuscript review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from Institutional Ethical Committee-2, Bhaikaka University, Karamsad, Anand, Gujarat [DHR Reg No- EC/NEW/INST/2021/592 and OHRP Reg No-IRB00014178] and Approval number-IEC/BU/2024/Cr. 26/185/2024 dated 20/05/2024
Informed Consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.