
Abstract
Objective:
To evaluate the effectiveness of a tech-enabled telesonography service in an under-resourced obstetrics and gynecology (OB/Gyn) clinic.
Materials and Methods:
Quantitative data were collected for each sonographic exam to determine its efficiency and accuracy. A survey was also offered to measure patient satisfaction. Data were collected and analyzed to produce early trends following the implementation of the service.
Results:
The tech-enabled telesonography service decreased patient exam and report turnaround times in an under-resourced OB/Gyn clinic, which correlated with decreases in the time until the next appointment and the clearing of scheduling backlogs. Importantly, this efficiency was achieved without forfeiting diagnostic accuracy or patient satisfaction.
Conclusion:
This project demonstrated that the service provided reduced wait times for this under-resourced clinic without sacrificing diagnostic accuracy.
A service evaluation was performed at an independent obstetrics and gynecology (OB/Gyn) clinic in central Texas. The second-largest state by area and population, 1 Texas has struggled in recent years to provide enough health care services for their population, a problem exacerbated by the closure of 29 rural hospitals since 2005. 2 Services are especially scarce for pregnant patients as 46.5% of Texas counties are defined as maternity care deserts. 3
The study clinic was located in an urban county with full access to maternal services but was flanked by both low-access counties and maternity care deserts, 3 creating an increase in demand for services. The clinic was short-staffed, unable to fully meet patient demand, and had a 4-week wait time for a sonography appointment.
The goal in implementing and evaluating a telesonography solution (Telescan)® was to serve more patients and increase access to sonography in this under-resourced area. This study evaluated the effectiveness of the solution by measuring both quantitative and qualitative data to determine exam efficiency and accuracy, as well as patient satisfaction. Prior to conducting this service evaluation, it was agreed that prenatal care was best administered at the bedside by an expert sonographer and obstetrician and/or maternal-fetal medicine specialist. More data must be collected that demonstrate telemedicine’s noninferiority to standard, in-person prenatal care systems for both low- and high-risk patients before it is considered an ideal model. 4 However, when this level of care is not readily available, other solutions must be considered. It was hypothesized that the implementation would decrease exam and report turnaround times, which would ultimately allow the clinic to see more patients, decrease the wait time until the next appointment, and begin to clear their longstanding backlog. These outcomes, it was hypothesized, could be met without sacrificing diagnostic accuracy or creating a precipitous drop in patient satisfaction.
Materials and Methods
Overview of Telesonography
Telesonography is a telemedicine approach to providing sonography services. Defined simply, telesonography provides sonography via a telecommunications link that connects a local provider and their patients with a remote expert. Telesonography can be delivered synchronously or asynchronously. 5 Asynchronous transmission involves acquiring sonography cine clips, storing them locally, and transmitting them for analysis later. This method has been more commonly used due to its lack of dependence on sonographer availability and the convenience it provides for patient scheduling.
Conversely, synchronous transmission occurs as the exam is performed. As the patient is examined, data are transmitted to the remote expert, who can review the data, provide feedback, and request additional cine clips as necessary. This method is highly beneficial to patient care as pathology can be detected and reported immediately. This enables providers to request additional imaging and tests, escalate care, and create a treatment plan while the patient is still in the exam room. Modern applications of synchronous communication can be found in mobile point-of-care sonography devices, dedicated telesonography systems, and the implementation of a satellite care model that uses existing equipment.
The latter application, synchronous communication via a satellite care model, was the application used for this evaluation. Specifically, this study reviewed the impact of TeleScan, a cloud-based software-as-a-service solution that is compliant with the Health Insurance Portability and Accountability Act (HIPAA) and cleared by the Food and Drug Administration (FDA). TeleScan meets FDA image quality requirements (like quality regulations for sonography equipment systems) and all study images were collected via FDA-cleared equipment and meet Digital Imaging and Communications in Medicine (DICOM) standards. No images were compressed or otherwise compromised when uploaded to TeleScan.
A Voluson S8 (GE Medical, Waukesha, WI) with a 2D curvilinear transducer was used to obtain the cine clips throughout the study. Exams were performed by health care workers certified through a proprietary program that includes learning modules and hands-on practice. The goal of the training is to teach the basic mechanics of handling a transducer and utilizing the TeleScan software to obtain cine clips. The local health care worker acquiring cine clips may be a sonographer, if one is available, but may also be another health care staff member, such as a medical assistant. This model aligns with recent calls to use these versatile professionals to the fullest extent permitted by law. 6 During the exam, TeleScan facilitates cine clip capture to ensure necessary views for exams are obtained. TeleScan performed growth scans, biophysical profiles, and a nuchal translucency exam during the study period.
The cine clips were uploaded to a secure cloud platform where a certified maternal-fetal medicine sonographer provided diagnostic assessment, according to American Institute of Ultrasound in Medicine (AIUM) guidelines. Every sonographer involved was a graduate of an accredited Diagnostic Medical Sonography program, carried an active registry in both OB/Gyn and fetal echocardiography, through the American Registry for Diagnostic Medical Sonography (ARDMS), and had two or more years of experience in maternal fetal medicine. In addition, they are certified in Nuchal Translucency and Nasal Bone through The Fetal Medicine Foundation or Nuchal Translucency Quality Review Program, as well as Cervical Length Education and Review (CLEAR), provided by the Perinatal Quality Foundation. The sonographers were all TeleScan-certified through a proprietary program that included learning modules, practice in a demo environment, workflow and software proficiency assessments during clinic hours, and ongoing training for each subsequent software release.
The sonographers involved worked with the TeleScan software to review the cine clips, provide annotations and measurements, and compile a preliminary diagnostic report for the provider to review.
The provider accessed the report through the TeleScan software, and could modify the report, remeasure structures, add their conclusions, and sign the final report before relaying results to the patient.
If, at any point during the examination, the sonographers faced an abnormal finding, they escalated the issue via the provider’s predetermined channels, similar to the procedures followed by the onsite sonographers. In addition, local health care workers capturing the cine clips were specifically trained to refrain from providing observations and were not charged with communicating results to the patient. Not dissimilar to sonographers working in many traditional roles, the health care worker instructed patients to follow-up with their provider for exam results.
Data Collection
Data were gathered during a 6-month period from December 2022 to May 2023. The sonography studies completed during this timeframe included one first-trimester exam, 12 second-trimester exams, and 447 third-trimester exams.
Quantitative exam data were gathered through time stamps and reports in the TeleScan software. Indicators of specific interest included patient volume, appointment duration, report turnaround time, and time until next appointment. Percentage of fetal structures measured and comparison of estimated fetal weight were also considered when evaluating the impact of a new service model on diagnostic accuracy.
Qualitative data were gathered via an online survey, provided in both English and Spanish. The survey was accessed by a QR code on a patient pamphlet which was distributed before each telesonography exam. Patients were given verbal instructions that completion of the survey indicated consent for their anonymized data to be used. Indicators of specific interest included a patient’s perception of their own ease during the appointment and their likelihood of recommending the telesonography model to others.
Both quantitative and qualitative data were analyzed in aggregate to produce early trends following the telesonography implementation.
Results
During the study, the service was provided to an average of 9 to 10 patients per day (see Figure 1), which aligns well with AIUM Practice Principles. 7
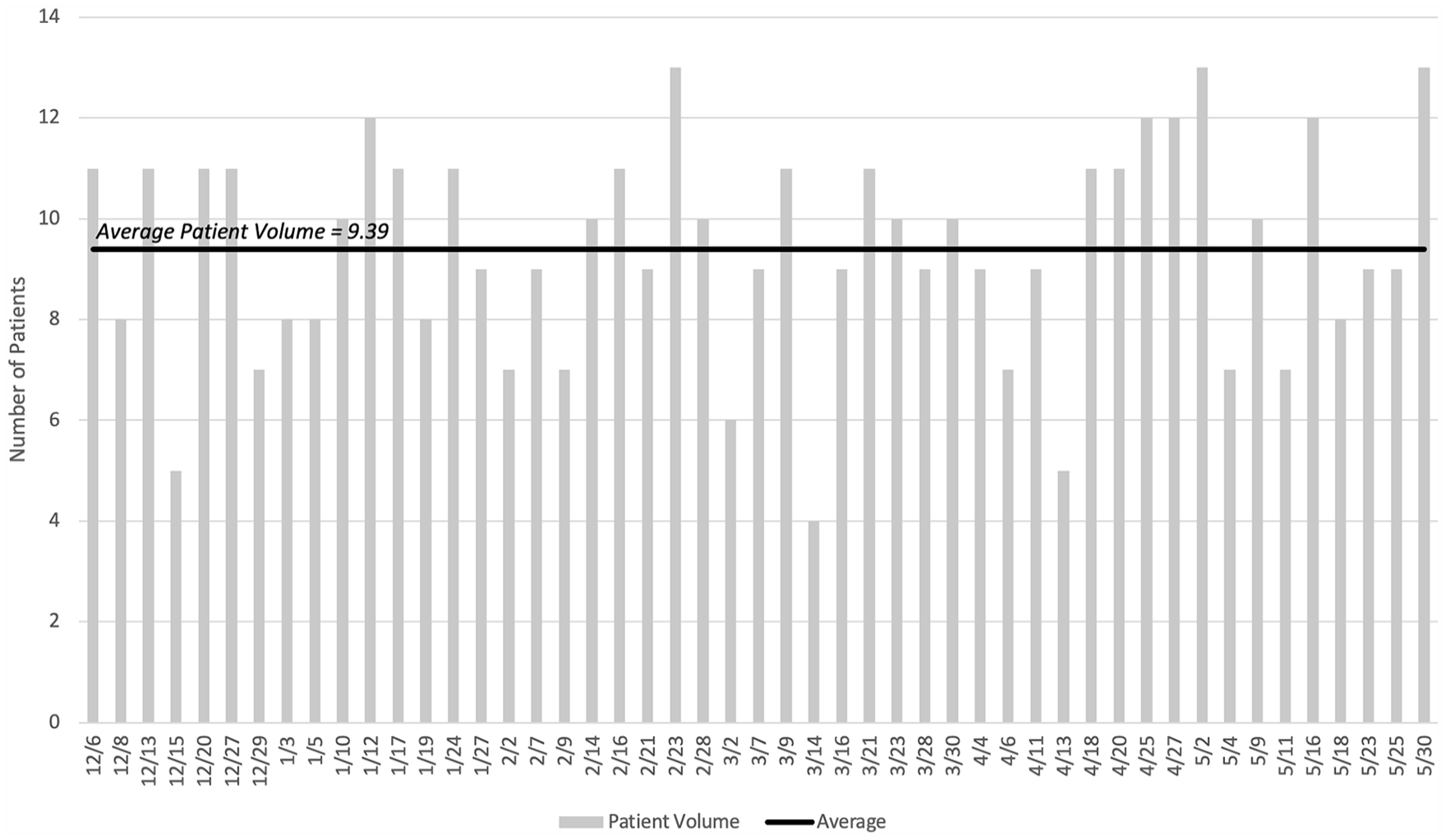
The daily patient volume in the study clinic during the length of data collection.
Time stamps within the TeleScan software demonstrated the length of time needed to capture the required cine clips, which 13 minutes on average. This average did not account for variability in exam type or the experience of the health care worker capturing cine clips, so while a direct comparison to industry averages is not conducted within this study, it is recommended to review the benchmarking data provided by the Association for Maternal-Fetal Medicine Management, 8 to provide context.
The facility reported that the service also reduced their report turnaround time by 61%, taking an average of 20.8 minutes to complete preliminary diagnostic reports, according to the TeleScan time stamps (see Figure 2).
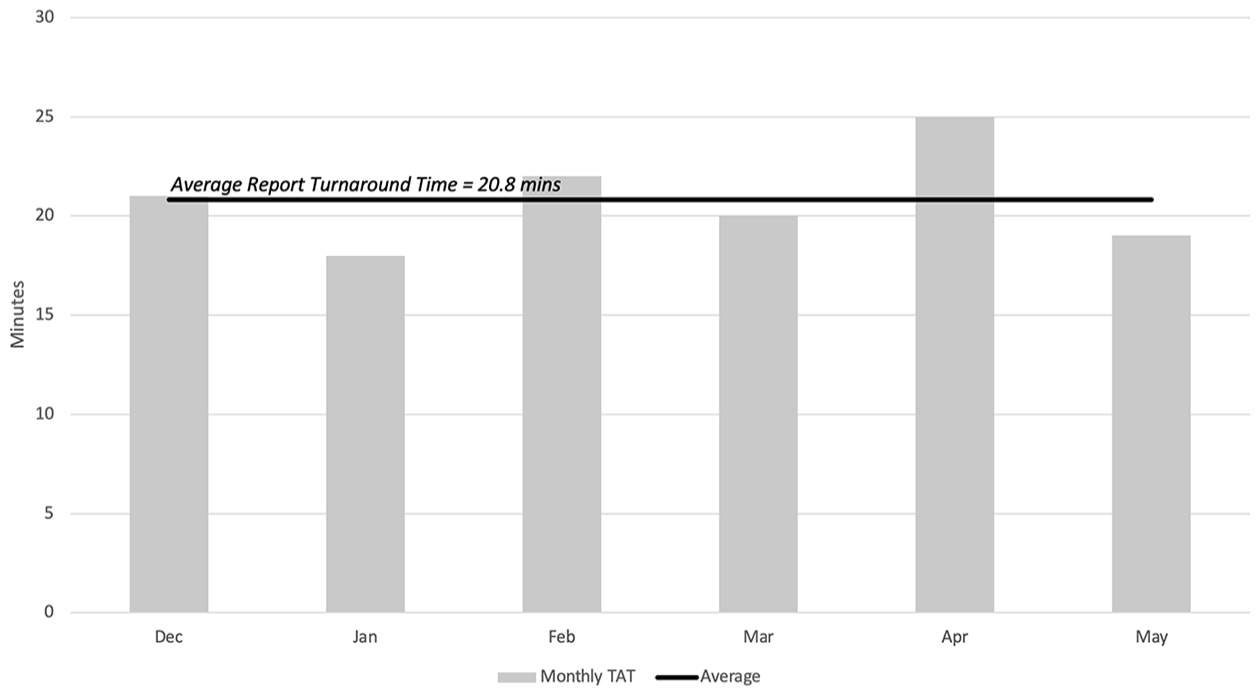
The average preliminary diagnostic report turnaround time (TAT), segregated by the month the study was conducted.
A more detailed look at the data revealed that while report turnaround times could vary by up to 94 minutes, based on the patient, daily averages showed more consistency, varying by only 21 minutes (see Figure 3). Interestingly, there was no correlation between the number of patients seen and the daily average for report turnaround times.
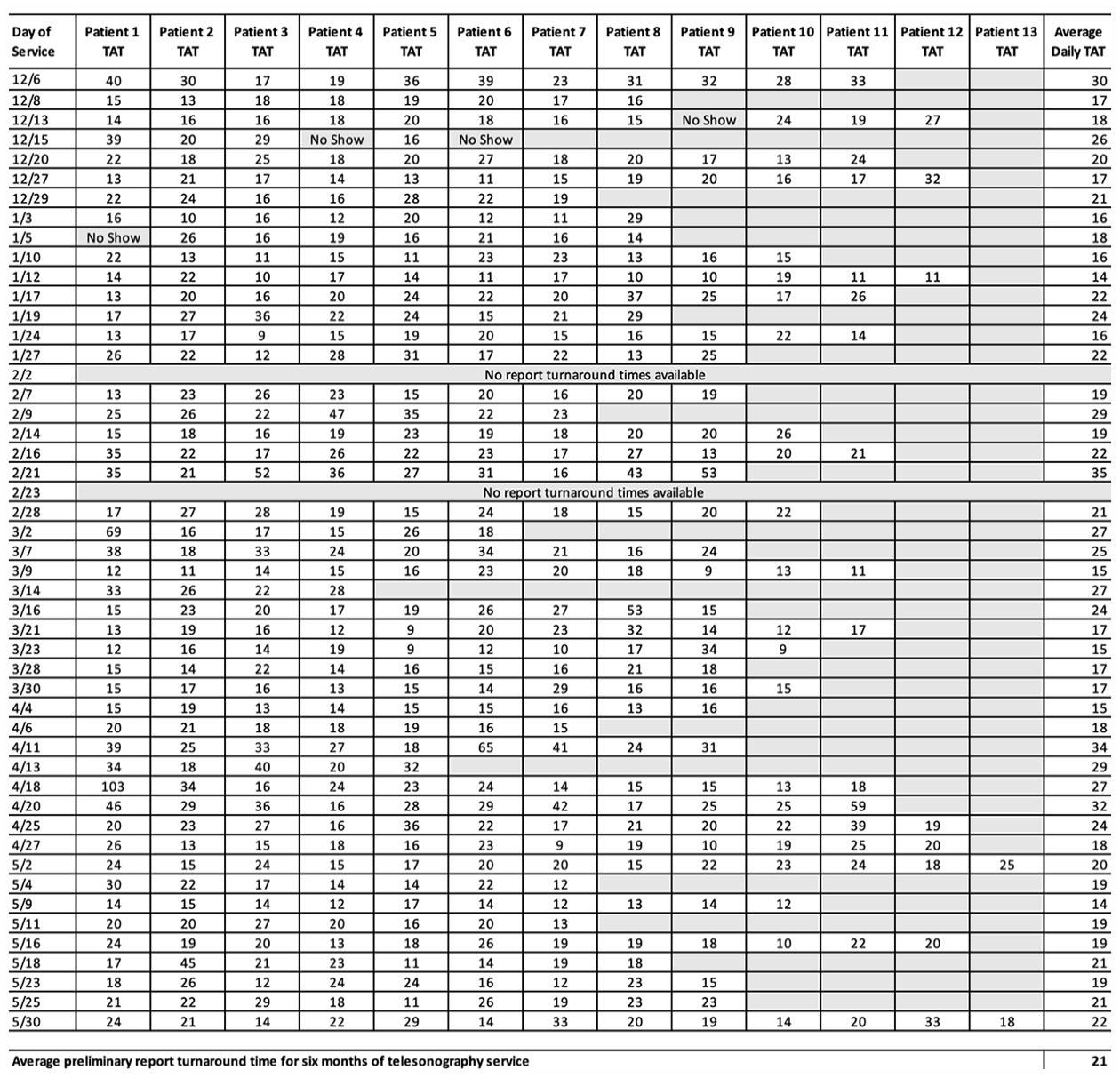
The preliminary diagnostic report turnaround time (TAT), based on the patient examined.
The result of these gains in efficiency was a 50% reduction in wait times until the next available appointment, as reported by the health care facility. The previous wait time was 4 weeks. After 3 months of TeleScan implementation and service, the wait time until the next appointment had diminished to less than 2 weeks.
Accuracy Indicators
Throughout the duration of the study, TeleScan provided visualization of critical anatomical structures in both the first and second trimesters with 100% reliability. Fetal sonography studies performed in the late third trimester are often limited due to acoustic attenuation and fetal positioning; 9 however, the service provided visualization of critical structures with greater than 90% reliability.
Fetal biometry measurements obtained using TeleScan adhere to the practice parameters established by the AIUM. During the study, the head circumference, biparietal diameter, abdominal circumference, and femur length measurements were used to calculate estimated fetal weight. 10 Estimated fetal weight (EFW) measurements performed through TeleScan were then compared to EFW measurements taken by an onsite sonographer. The TeleScan measurement was consistently within one to three ounces of the onsite evaluation for pregnancies between 20 and 36 weeks. At 20 weeks’ gestation, a one-ounce difference was recorded, accounting for a 9% difference. In the third trimester, remotely recorded EFWs were within 2% to 4% of onsite measurements. These results indicated high diagnostic accuracy well within the accepted range of up to 20% in either direction. 11
Patient Satisfaction Indicators
Patient surveys administered after each exam included two close-ended questions and one open-ended question:
Close-ended question #1: Would you recommend this care (ultrasound) team to a close family member or friend?
Close-ended question #2: Did the care (ultrasound) team put you at ease during your appointment?
Open-ended question: Comments
The survey did not have a high response rate. However, the limited results are included, as an early indication of what is achievable. Thirteen responses were collected during the time of the study. Close-ended question #1 received a 69% “yes” response rate, indicating high satisfaction with the telesonography exam experience. Four patients (31%) indicated “no,” and provided comments indicating that telesonography felt distant compared to onsite sonography because it did not provide a personalized, connective experience. They indicated a desire for more visualization of the baby during the appointment and more exam images to take home.
Close-ended question #2 received a 92% “yes” response rate, indicating very high satisfaction with telesonography care teams. Patients who indicated “yes” reported that the care team was nice, kind, caring, awesome, super friendly, and accommodating.
Discussion
As demonstrated by the results of this service evaluation, TeleScan was able to decrease sonography exam and report turnaround times, which correlated with decreases in the time until the next appointment and the clearing of longstanding patient appointment backlogs. TeleScan accuracy indicators matched traditional, onsite capabilities and while patients may certainly prefer to have the sonographer at their bedside, the majority indicated they would still recommend the telesonography service model and were at ease during the exam.
More research is needed to determine how these trends hold or change over time for this clinical location. Future research regarding the effectiveness of telesonography should include geographically and demographically diverse locations as well as varying levels of telesonography utilization. In addition, studies that report on a longer timeframe will be key to determining how early trends continue or change as telesonography becomes an established mode of care and how telesonography impacts the continuum of care and access to prenatal services.
Limitations
This was a service evaluation and used a pre-experimental research design. The threats to internal and external validity make is impossible to generalize beyond the cohort of patients that received this service. The service was also limited in its scope to a single clinic and a 6-month timeframe postimplementation of a telesonography solution. During this timeframe, only one patient in the first trimester and 12 in the second trimester were examined, therefore data on the efficacy and efficiency of first and second trimester telesonography exams was limited. In addition, the patient survey garnered only 13 responses, which was too small a sample size to draw conclusions from but provided an important view into patient perceptions of the service model.
Furthermore, TeleScan was designed for obstetric sonography and was limited to singleton pregnancies. There are also limitations when imaging patients with an increased body mass index (BMI). Like traditional sonography, falling visualization rates in high BMI patients were noted. This was due to the depth of insonation required for high-contrast imaging and a higher rate of dropout due to absorption of sonography energy by abdominal adipose tissue. 12
Conclusion
This product evaluation of a tech-enabled telesonography solution, in an under-resourced clinic, demonstrated the service had the ability to decrease examination time and increase report turnaround speed. These gains correlated with a decrease in the time until the next available appointment and were achieved without sacrificing patient satisfaction and diagnostic accuracy, as indicated by EFW results and visualization of critical structures. These results may suggest that telesonography could be an effective tool in increasing access to sonography services for underserved counties and maternal care deserts.
Footnotes
Acknowledgements
The authors would like to acknowledge the following people for their contributions to this study: Melissa Mercado, RDMS (OB/GYN, FE); Katherine O’Brien, RDMS (AB, OB/GYN), RDCS (FE); Molly Siemens, RDMS (AB, OB/GYN, FE), RVT (VT); Sonia Graham, RDMS (OB/GYN, FE); Grace Nelms, RDMS (ABD, OB/GYN), RVT; Shyanne Rightmer, RDMS (OB/GYN), RVT; Kelsey Hughes, RT(s), RVT, RDMS (AB); (OB/GYN); Chelsey Willey, RDMS (OB/GYN, AB); Whitney Robinson, RDMS (AB, OB/GYN), RDCS (FE); Alexandra Knott, RDMS (AB, OB/GYN), RDCS (FE), RVT; Courtney Deal, RDMS (AB, OB/GYN), RVT; Samantha Hilton, ARDMS (AB, OB/GYN), RDCS (FE), NT; Jenna Rushing, RDMS (AB, OB/GYN); Amanda Ladd; and Juliette Wyatt.
Ethics Approval
Ethical approval was not sought for the present study because all data was deidentified and aggregated.
Informed Consent
Patients were given verbal instructions that completion of the survey indicated consent for their anonymized data to be used.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors are employed by BB Imaging, the parent company of TeleScan.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.