
Abstract
Objective:
This study was designed to use sonography and evaluate arteriovenous fistulas (AVFs) in dialysis patients. The aim was to determine criteria for distinguishing between patent AVFs with proper function (healthy) and unhealthy AVFs.
Materials and Methods:
This study enrolled 106 dialysis patients with an AVF. All fistulas were evaluated using spectral Doppler and grayscale sonography, assessing parameters such as draining vein diameter, distance of the venous vein from the skin surface, feeding artery diameter, presence of thrombosis, and fistula stenosis. Subsequently, Doppler criteria such as flow volume (FV) and resistance index (RI) were measured and compared between healthy and unhealthy AVFs.
Results:
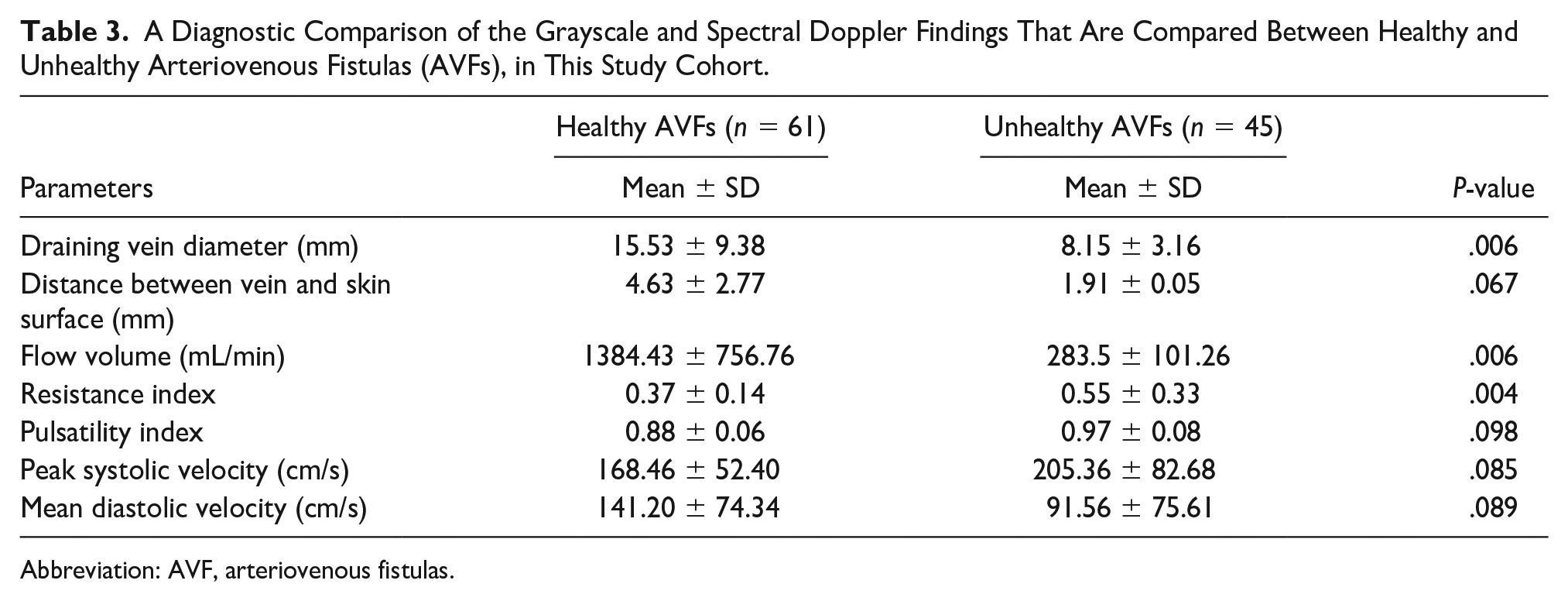
This cohort’s spectral Doppler findings demonstrated lower FV and higher RI, in unhealthy AVFs, compared to healthy ones (283.5 ± 101.26 mL/min vs 1383.43 ± 756.76 mL/min; P = .006) and (0.55 ± 0.33 vs 0.37 ± 0.14; P = .004) respectively.
Conclusion:
The spectral Doppler and grayscale sonographic imaging made it possible to evaluate AVF performance and determine its quality. In this cohort, a decreased FV, increased RI, and decreased draining vein diameter were observed in unhealthy AVFs. These results would suggest that sonographers and clinicians should pay close attention to these parameters when assessing the function of an AVF, for patients undergoing hemodialysis.
An arteriovenous fistula (AVF) is crucial in treating patients with chronic renal failure and requiring hemodialysis (HD). These AVFs are created through various surgical methods.1,2 While these fistulas are generally expected to function well, prolonged exposure to HD material can lead to injuries in their epithelial surface. 3 Moreover, the most common cause of AVF insufficiency is intravascular thrombosis resulting from stenosis.
Dysfunction of AVFs is a prevalent cause of long-term hospitalization in HD patients,4,5 and improving the lifespan of these fistulas is a primary therapeutic concern. Therefore early, and accurate diagnosis of lesions in AVFs could prevent long-term damage, enhance the lifespan of these fistulas, reduce treatment costs, and minimize morbidity associated with HD complications in patients.6 –8
Sonography has been widely recognized as a noninvasive and time-effective tool for assessing peripheral vascular anatomy since its first application by Strandness et al. to evaluate vascular lesions.9 –15 Recent studies utilizing spectral Doppler for vascular assessment have demonstrated its effectiveness, high sensitivity, and specificity, particularly in evaluating superficial vessels. The results of spectral Doppler examinations of the carotid, femoral, and lower extremity arteries have positioned spectral Doppler as a noninvasive and highly accurate diagnostic method for analyzing superficial vessels.16 –21 Various studies have also explored the role of peak systolic velocity (PSV) or systolic velocity ratio in diagnosing significant stenosis within an AVF.5,21 –24
While several studies have investigated AVF dysfunction using spectral Doppler, there needs to be more information on the sonographic criteria for determining the efficiency of AVFs.5,19 –22,24 Therefore, the aim of this study was to assess sonographic criteria for distinguishing between healthy and unhealthy AVFs, in dialysis patients.
Materials and Methods
Patient Recruitment
This case-control study was conducted at a teaching hospital in Tabriz between May 2017 and August 2021. The study received approval from the hospital’s ethics committee. The inclusion criteria were such that HD patients with an AVF and a history of dialysis, for at least 2 years, were recruited. The exclusion criteria were set to exclude patients over 75 or under 15 years of age, patients with cardiovascular disease, any autoimmune disease with potential vascular involvement, patients with arteriovenous graft (AVG), and those unable to cooperate during sonography. After obtaining informed consent from all patients, the participants were divided into two groups based on their last sonogram and clinical examination, which were documented in their medical records. The patient control group comprised participants with a patent fistula, which exhibited proper vascular function. In contrast, the comparison group consisted of patients with unhealthy AVFs, including fistulas with thrombosis, stenosis, aneurysm formation, and steal syndrome.
Sonographic Protocol
All AVFs were thoroughly evaluated using sonography conducted by a diagnostic radiologist with 19 years of clinical experience in vascular sonography. The patients were anonymized such that the radiologist did not know the patient’s AVF condition, whether it was a patent, a healthy fistula, or unhealthy. A WS80A ultrasound equipment system (Samsung Medison Co., Ltd., South Korea) with a linear array transducer (5–10 MHz) was utilized to evaluate all the patients’ AVFs. The patients’ measurements were also corroborated using a Zonare ultrasound equipment system (Zonare Medical Systems, Inc., Beijing, China) and a linear array transducer (3–8 MHz), to ensure diagnostic and measurement accuracy. Grayscale sonographic parameters were assessed, including the draining vein diameter, draining vein distance from the skin surface, feeding artery diameter, thrombosis, stenosis, and the presence of an aneurysm. Spectral Doppler was used to measure criteria such as flow volume (FV), resistive indices (RI), and pulsatility indices (PI), at the brachial and radial arteries (inflow arteries), proximal to the anastomosis site, longitudinally in all patients. Equipment software automatically calculated the FV after measuring the arterial inner diameter, placing a sample volume covering the entire luminal cross-section, using a Doppler angle ≤60°, and defining the cardiac cycle time. Three measurements were conducted using this method, and the average for FV, RI, PI, peak systolic velocity (PSV), and the mean diastolic velocity was recorded as the final measurement 24,25 (see Figures 1 and 2).
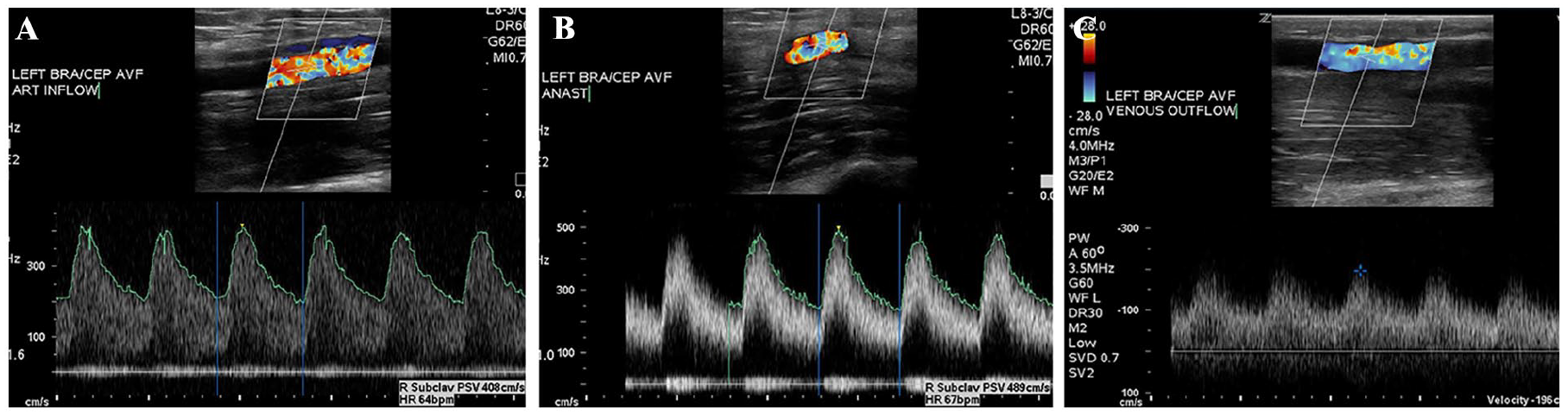
A sonogram of the left upper extremity brachial-cephalic fistula is provided and utilizes color and spectral Doppler in a patient with a patent arteriovenous fistula (AVF). (A) The sonogram demonstrates the arterial part of the brachial-cephalic AVF and shows that the arterial inflow within the left brachial artery, which measured 408 cm/s. (B) The sonogram demonstrates that the flow volume within the anastomosis, which measured 489 cm/s. (C) The sonogram captures the venous outflow, which measured 196 cm/s.
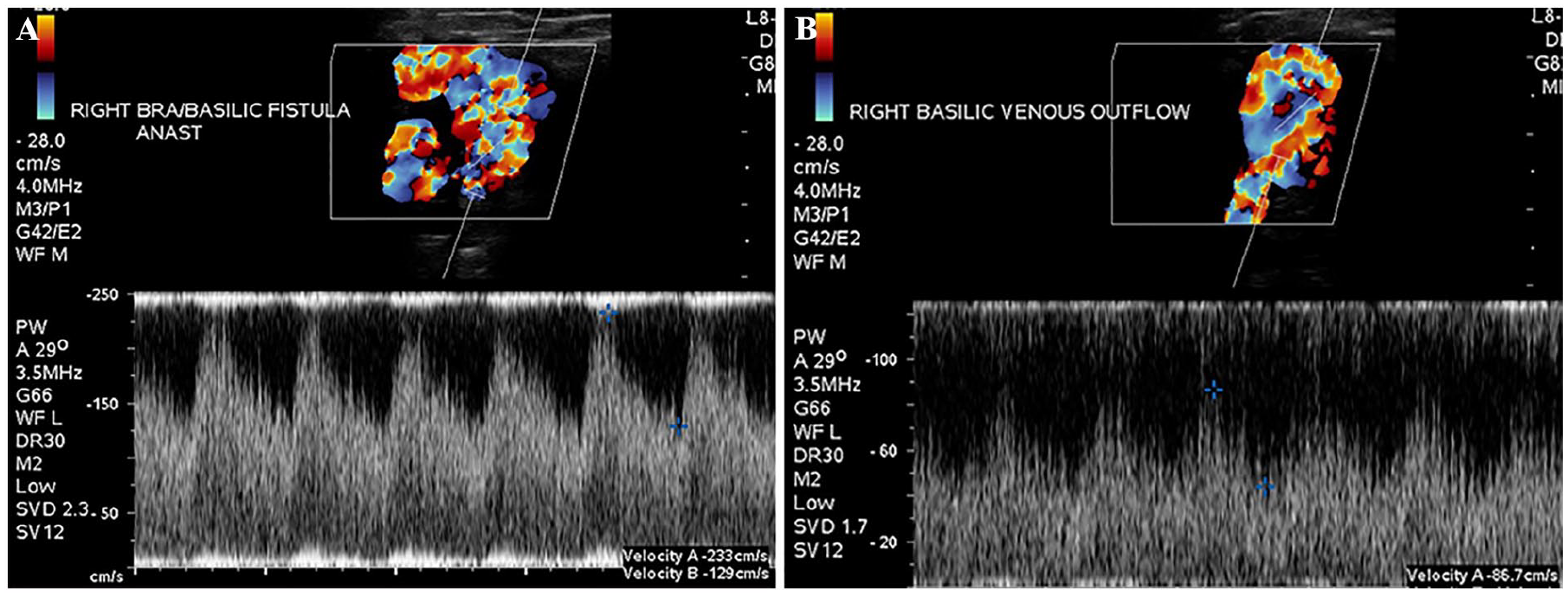
A sonogram of the right upper extremity brachial-basilic fistula using color and spectral Doppler in a patient with a patent arteriovenous fistula (AVF). (A) The sonogram demonstrates that the flow volume within the anastomosis measured 233 cm/s. (B) The sonographic measurement shows that the venous outflow, within the right basilic vein, was measured at 86.7 cm/s.
Statistical Analysis
The data were analyzed using SPSS version 24 (SPSS Inc., Chicago, IL, USA). Descriptive statistical methods were used to evaluate the parameters, and the data were reported as frequency (%) and mean ± standard deviation. The chi-square test was used to compare qualitative data, and a Student’s t-test was used for quantitative data. Pearson’s product-moment and Spearman’s coefficient were employed to determine the relationships between variables. A P-value less than .05 was considered statistically significant.
Results
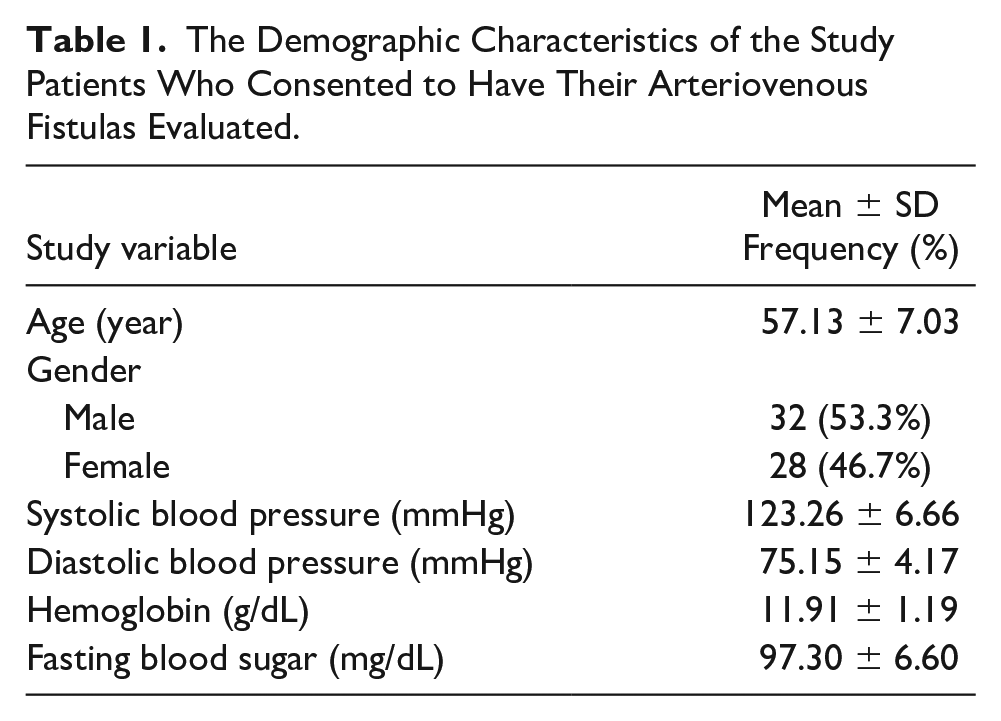
In this case–control study, 106 patients with AVFs were included. The control group consisted of 61 patients with a healthy AVF, and the comparison group had 45 patients with an unhealthy AVF. The demographic characteristics of the patients are presented in Table 1. The mean age of the participants was 57.13 ± 7.03 years, ranging from 15 to 75 years of age. Among the patients, 32 (53.3%) were male. The mean systolic blood pressure was 123.26 ± 6.66, and the mean hemoglobin level was 11.91 ± 1.19 g/dL (see Table 1).
The Demographic Characteristics of the Study Patients Who Consented to Have Their Arteriovenous Fistulas Evaluated.
Among the 61 healthy AVFs, 22 (36%) were of the brachial-cephalic type, 8 (13%) were brachial-basilic, and 31 (50%) were radiocephalic. In the group with unhealthy AVFs, 24 (53%) were of the brachial-cephalic type, 6 (13%) were brachial-basilic, and 15 (33%) were radiocephalic (see Table 2).
The Varied Types of Arteriovenous Fistulas (AVFs) are Further Classified for This Study Into Patient Groups, as to Healthy and Unhealthy Fistulas.
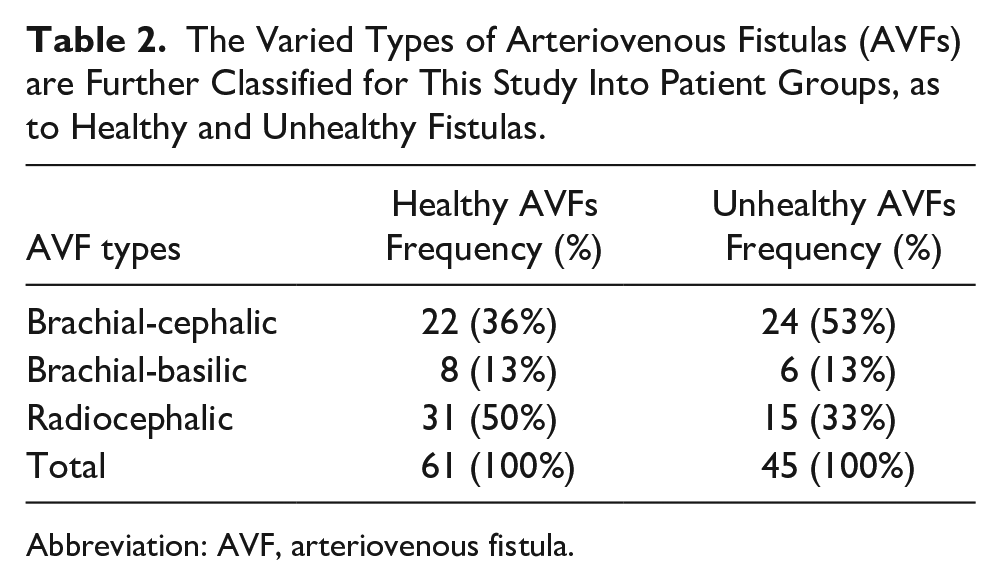
Abbreviation: AVF, arteriovenous fistula.
In the control group, the mean diameter of the draining vein was 15.53 ± 9.38 mm, and the mean distance of the draining vein from the skin surface was 4.63 ± 2.77 mm. The RI and PI were 0.37 ± 0.14 and 0.88 ± 0.06, respectively, and the PSV was 168.46 ± 52.40 cm/s. In the comparison group, the draining vein’s mean diameter and the draining vein’s mean distance from the skin surface were 8.15 ± 3.16 mm and 1.91 ± 0.05 mm, respectively. Additionally, the mean RI of the AVFs was 0.55 ± 0.33 (see Table 3).
A Diagnostic Comparison of the Grayscale and Spectral Doppler Findings That Are Compared Between Healthy and Unhealthy Arteriovenous Fistulas (AVFs), in This Study Cohort.
Abbreviation: AVF, arteriovenous fistulas.
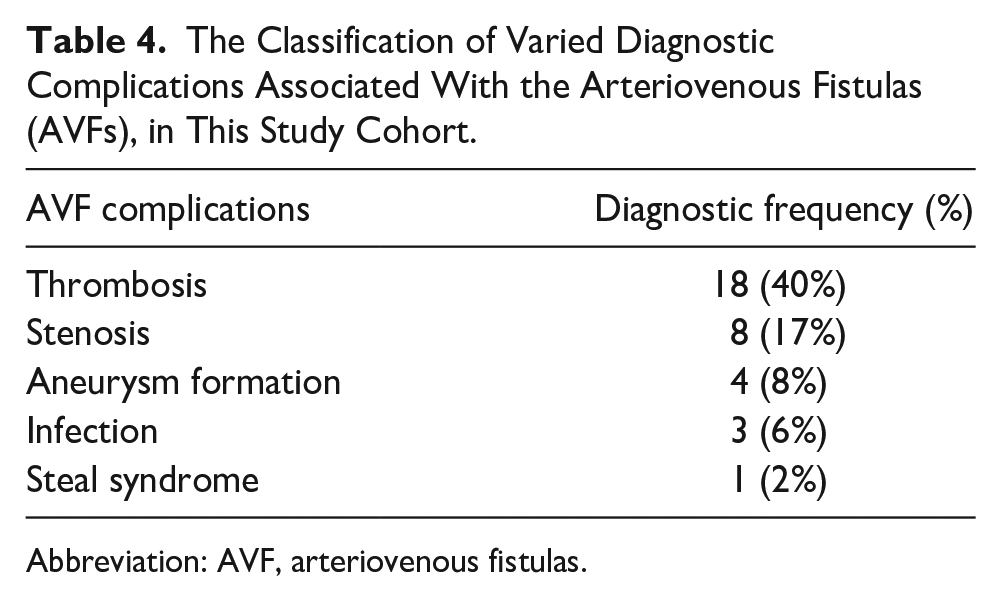
In the evaluation of all the AVFs, it was noted that 18 (40%) had thrombosis, 8 (17%) had varying degrees of stenosis, and 4 (8%) had an aneurysm present (see Table 4 and Figure 3).
The Classification of Varied Diagnostic Complications Associated With the Arteriovenous Fistulas (AVFs), in This Study Cohort.
Abbreviation: AVF, arteriovenous fistulas.
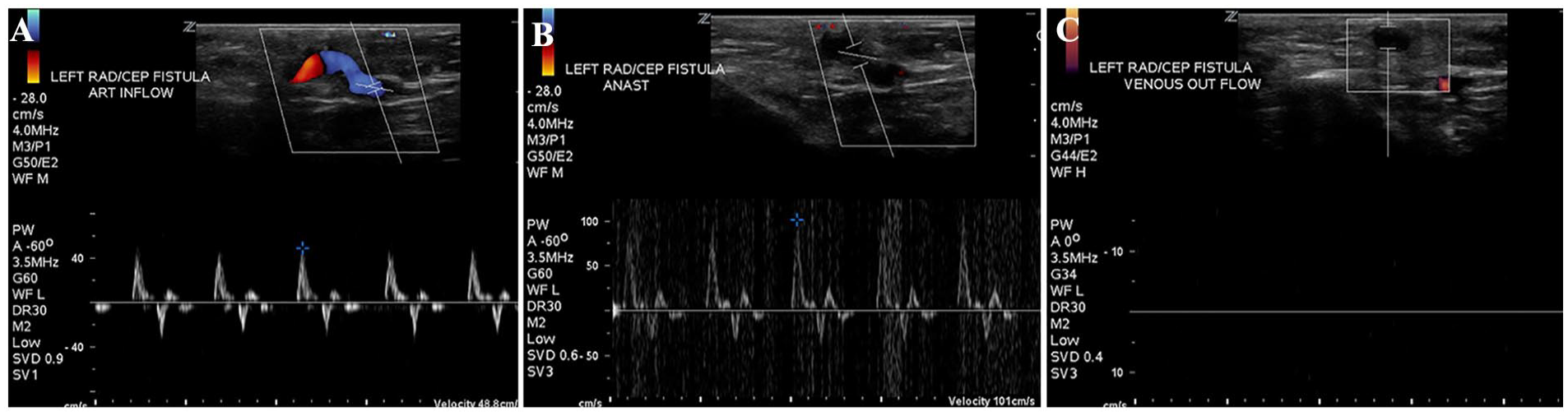
The sonographic evaluation of the left upper extremity radiocephalic fistula using color and spectral Doppler, in a patient with diminished thrill. (A) The sonogram captures the left radial artery inflow and demonstrates a triphasic waveform, with an abnormal flow velocity measured at 48.8 cm/s. (B) The sonogram demonstrates the anastomosis site of the fistula and captured an increased velocity of 101 cm/s. (C) The sonographic image shows that the cephalic vein outflow was completely thrombosed with no evidence of color flow or spectral Doppler tracing.
The results indicated that the diameter of draining veins in unhealthy AVFs was less than in healthy ones, and the difference was statistically significant (P = .006). There was a significant difference in the mean FV between healthy and unhealthy AVFs, with a higher FV observed in healthy AVFs (1384.43 vs 283.5 mL/min, respectively; P = .006). Spectral Doppler assessment demonstrated a higher RI in unhealthy AVFs compared to healthy ones (0.55 vs 0.37, respectively), which was statistically significant (P = .004).
No significant differences were found in PI, PSV, and mean diastolic velocity between unhealthy and healthy AVFs (P > .05) (see Table 3).
Discussion
Regular monitoring of an AVF in HD patients is vital for the early detection of abnormalities and any vascular malfunctions, which could lead to proper interventions and improved patient survival. While angiography has been considered the gold standard for evaluating AVF status, spectral Doppler offers some diagnostic advantages over angiography.21,26
In this case-control study, spectral Doppler assessment revealed significantly a lower FV and higher RI in unhealthy AVFs compared to those that were healthy. Other study variables that were investigated did not show significant differences. The most common diagnostic complication observed was a thrombosis (40%). A study by Pietura et al. examined 139 patients with mature AVFs. The mean duration of dialysis was 38 months, and the mean fistula lifespan was 26 months. Only 38% of those patients had a primary fistula implantation. The mean FV was reported as 1204.1 mL/min, the mean RI as 0.51, and the mean PI as 0.86, which is consistent with the present study findings. 27
Katherin et al. evaluated 61 patients with AVFs using spectral Doppler. They reported a mean FV of 464 mL/min in a normally functioning AVF. 28 Their reported average FV is lower than what was recorded in the present study; however, this could potentially be attributed to variances in technical measurements. Previous studies by Moghazy et al. and England et al. have reported average FVs ranging from 500 to 1000 mL/min.29,30 Von Stemple et al. found that an FV in the brachial artery, of over 1000 mL/min, predicted good fistula function, and those findings do support the present study findings. 31
Several studies have demonstrated a decrease in AVF complications with an increasing FV. Complication rates increase when the FV falls below 460 mL/min. Studies have suggested that the FV of AVFs should ideally range between 600 and 1500 mL/min.5,24,32 Recent evidence suggests that stenosis incidence in AVFs is high when the FV is below 650 mL/min.33,34 Another study by Mohamed et al. showed a high incidence of thrombosis with FVs below 500 mL/min or a reduction of more than 25% from baseline. 35 Considering the standard protocols, HD is typically performed with blood flow rates of 350 to 450 mL/min for 3.5 to 4 hours, three times a week. Therefore, AVFs with FVs below 350 mL/min cannot provide adequate flow for HD. 36
Limitations
The major limitation of this study is the research design, which has threats to internal and external validity. It is important to note that these results cannot be generalized beyond those patients within this study. An added limitation to this study is the limited number of patient cases, which may introduce some bias to the results. A replication of this study, with an expanded number of patients, is recommended to validate these study results. Another limitation of the current study is the absence of individual comparisons for Doppler measurements across different types of unhealthy fistulas. Further studies, with a more focused diagnostic approach, might reveal diagnostic results and Doppler findings based on varied subtypes of unhealthy AVFs. The current study focused solely on assessing patients with an AVF and did not include patients with an AVG. Therefore, future studies that specifically address and focus on these types of AVFs would be valuable and add to the literature.
Conclusion
Spectral Doppler and grayscale sonographic techniques can help evaluate AVF performance and determine its hemodynamic quality. Decreased FV, increased RI, and a decreased draining vein diameter were commonly observed in this cohort’s unhealthy AVFs. Therefore, sonographers and clinicians should pay close attention to these parameters when assessing the function of AVF in patients undergoing HD.
Footnotes
Ethics Approval
This study was approved based on an ethical review by the hospital’s Institutional Review Board (IR.TBZMED.REC.1398.175).
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.