
Abstract
Objective:
This study was designed to compare sonography to skeletal radiography, in the diagnosis of long bone fractures.
Materials and Methods:
This was a cross-sectional and analytical study including 188 patients of varied ages that had 251 suspected long bone fractures. It was conducted over a 9-month period, in the emergency department of a teaching hospital, within the Swat district of Pakistan. After assessing the clinical symptoms of the fracture by an emergency orthopedic physician, sonography was followed by a radiograph performed for these referred patients.
Results:
Sonography shows a diagnostic accuracy of 91.23% for detecting long bone fractures, with a sensitivity and specificity of 100% and 76.84%, respectively. The positive predictive value and negative predictive value were 87.64% and 100%, respectively. Sonography was able to detect small fractures (up to 0.23 mm) that are often missed on the patient’s radiograph.
Conclusion:
Sonography may be useful as an initial screening imaging technique for the diagnosis of long bone fractures. The potential exists to reduce the need for unnecessary skeletal radiographs, which could reduce treatment time, cost, and ionizing radiation hazards.
Long bone fractures are one of the most common types seen in emergency departments (EDs), affecting people of all ages, genders, and social classes. 1 The term fracture, can be commonly described by the public as a break or crack, is a medical term used for a broken bone. 2 It is a medical condition in which a partial or complete fracture occurs in the continuity of the bone. 3 According to the Centers for Disease Control and Prevention, bone fractures are among the top 20 most common medical diagnoses reported in the ED. 4 One of the main causes of bone fracture is trauma, which can result from various sources such as traffic accidents, falls, and physical assaults. 5 Among these, roadside accidents have emerged as the primary cause for fractures and rank as the ninth leading cause of death globally. 6 According to World Health Organization (WHO), the global number of deaths due to road traffic accidents (RTAs) has exceeded 1 million annually. 7 Falls remain another frequent cause of bony injury, with a prevalence ranging from 21.8% to 35.1%, across both genders. 4 Notably, the likelihood of sustaining fractures due to falls increases with age. 2
Globally 178 million new cases of fracture were estimated in 2019, across all age groups. 3 The age-standardized incidence rate for bone fractures was calculated to be 2296, two per 100 000 population, while the age-standardized prevalence rate for the same population was identified to be 5614. 3 Consequently, in 2019, the prevalence of fractures for all age groups reached 455 million. 8 The age-standardized prevalence rate of bone fractures in men was found to be higher than that of the women. 8 In terms of distribution of fracture by age, men are more susceptible to fractures before the age of 50, whereas women are more prone to fractures after 50 years of age. 9 Considering age as a risk factor, fractures are more commonly observed in children compared with adults; however, these fractures are usually less complicated in nature. 2 Moreover, boys are three times more prone to fractures than girls. 10
Fracture can occur in any part of the skeleton, but fractures of long bones have a significant psycho-socioeconomic impact 4 because they play a crucial role in body movements, structural support, and organs protection. 11 In adults, the radius is the most commonly observed fractured bone, followed by the humerus and fibula. 12 Fractures of the long bones significantly impact society leading to decreased productivity, high treatment costs, increased mortality, and morbidity. Low-income countries are particularly affected by the consequences of long bone fractures as 90% of extremity fractures tend to occur in these countries. The effects of long bone fractures are not only physical, but psychological, financial, occupational, and social as well. Fractures can cause pain, swelling, lack of movement, and deformity in the affected bone. 4
According to the WHO, diagnostic imaging services are inaccessible to more than 75% of the global population.13,14 Conventional radiography is currently considered the diagnostic gold standard and the primary imaging technique, to diagnose skeletal fractures. 15 Additional diagnostic imaging techniques used to identify bone fractures include computed tomography (CT) 16 and magnetic resonance imaging (MRI). 17 However, CT cannot be used as the initial diagnostic choice, due to the increased radiation dose, despite its excellent sensitivity and specificity compared with radiography. Similarly, MRI cannot be used as the primary imaging technique primarily because of the increased cost and prolonged imaging time, despite its excellent sensitivity and specificity.5,18
Although radiography is used as the diagnostic gold standard for detecting skeletal fractures, it does have certain limitations. Radiography employs low-dose ionizing radiation which may be contraindicated for some patients. Adults exposed to ionizing radiation, during their childhood, may be at higher risk to develop breast and thyroid cancers, later in life. 19 Children are about ten times more radiosensitive compared with adults, which is the result of their smaller body size and higher mitotic activity. 20 In Germany alone, approximately 40 million extremity radiographs were performed in 2014. 21 A study revealed that 82.8% of the radiographs completed on children, for suspected fractures, provided no diagnostic evidence of a fracture. 21 Given the unnecessary exposure to ionizing radiation associated with radiography, an alternate noninvasive imaging technique that does not employ ionizing radiation, such as sonography, should be considered for detecting long bone fractures.22,23 Sonography has significant advantages in terms of accessibility and portability. In contrast to CT and MRI equipment, ultrasound equipment systems can be conveniently transported to locations where patients are unable to visit an imaging department. Dynamic assessment of patients is made possible using sonography, with the added ease of image reproduction without any risk. Furthermore, sonography possesses a unique capability of getting feedback from patients, using tactile pressure. Sonography of bone has the potential to detect minor abnormalities, owing to its superior axial resolution, and this is made possible due to imaging with a higher frequency transducer. Sonography can detect minute fractures as small as 1.0 mm in size. It is imperative to acknowledge that the accuracy of sonography in diagnosing long bone fractures relies on the proficiency of the sonographer and is user-dependent. The primary goal of this study was to discover the diagnostic accuracy of sonography, when operated by a proficient sonographer, in detecting long bone fractures. In addition, this study was designed to assess the capability of sonography in identifying fractures less than 1.0 mm in size.
Materials and Methods
This cross-sectional study was conducted from September 2022 to May 2023, at a teaching hospital located in the Swat district of Pakistan. The study was approved by the Institutional Review Board, at the University of Lahore, Pakistan (IRB#: REC-UOL-/240-09/2022). A total of 188 patients were recruited and were within the ages of 0 to 85 years. These participants presented to the ED with the clinical suspicion of a bony fracture and were potentially enrolled into the study. This cohort of patients had a total of 251 suspected long bone fractures, and the increased number was due to multiple fractures, in some patients. After obtaining clinical confirmation, by an orthopedic surgeon, the clinically suspected patients were referred to the radiology department, within the ED, for a radiograph, designed to confirm a fracture. Inclusion criteria for the study involved post-trauma patients presenting with pain, swelling, tenderness, deranged motion of the affected side, and bruising (ecchymosis), at the site of the bone injury. The exclusion criteria included patients with open fractures, neurovascular injuries, soft tissue lesions at the site of fracture, life threatening injuries, patients with unstable signs, refracture, severe pain during sonography, orthopedic hardware, and the presence of dislocation accompanied with a fracture. After fulfilling the inclusion criteria, the patients/guardians were informed about the study and written informed consent was obtained before the patient undergoing sonography and a radiographic evaluation of the potential long bone fracture.
Sonographic Technique
The patients were evaluated sonographically in a comfortable position. Children were usually evaluated in the lap of their parents/guardians. For patients who were unable to be shifted to the patient’s examination couch, such as those on stretchers and wheelchairs, the sonogram was performed in their respective position. A well-maintained portable MyLab Sigma (Esaote, Florence, Italy) ultrasound equipment system, equipped with a 4 to 15 MHz linear transducer, was used to evaluate the suspected fracture site. By employing a high-frequency transducer, the axial resolution is significantly improved, enhancing the transducer’s capability to capture high-resolution images, with fine anatomic details. Enough ultrasonic lotion was applied to the area of interest for proper transducer coupling. The examination was started by placing the transducer at right angle to the lateral side of the injured bone. The focus and gain settings were adjusted according to the area of interest, to acquire high-quality images and determine the precise location and depth of the bone affected. Once the hyperechoic cortex of the bone identified (see Figure 1A), the transducer was placed longitudinally to assess the entire bone for the presence of fracture. Sonographic features indicative of a long bone fracture included the presence of a cortical gap (see Figure 2), cortical bulging (see Figure 3), deviation (see Figure 4), irregularity (see Figure 5), localized thin appearance, double-line cortex (see Figure 6), presence of the avulsed fragments (see Figure 7), and hematoma (see Figure 2). If a cortical gap was detected, its measurement was taken by determining the distance between the cortex of the displaced fractured and normal bone.
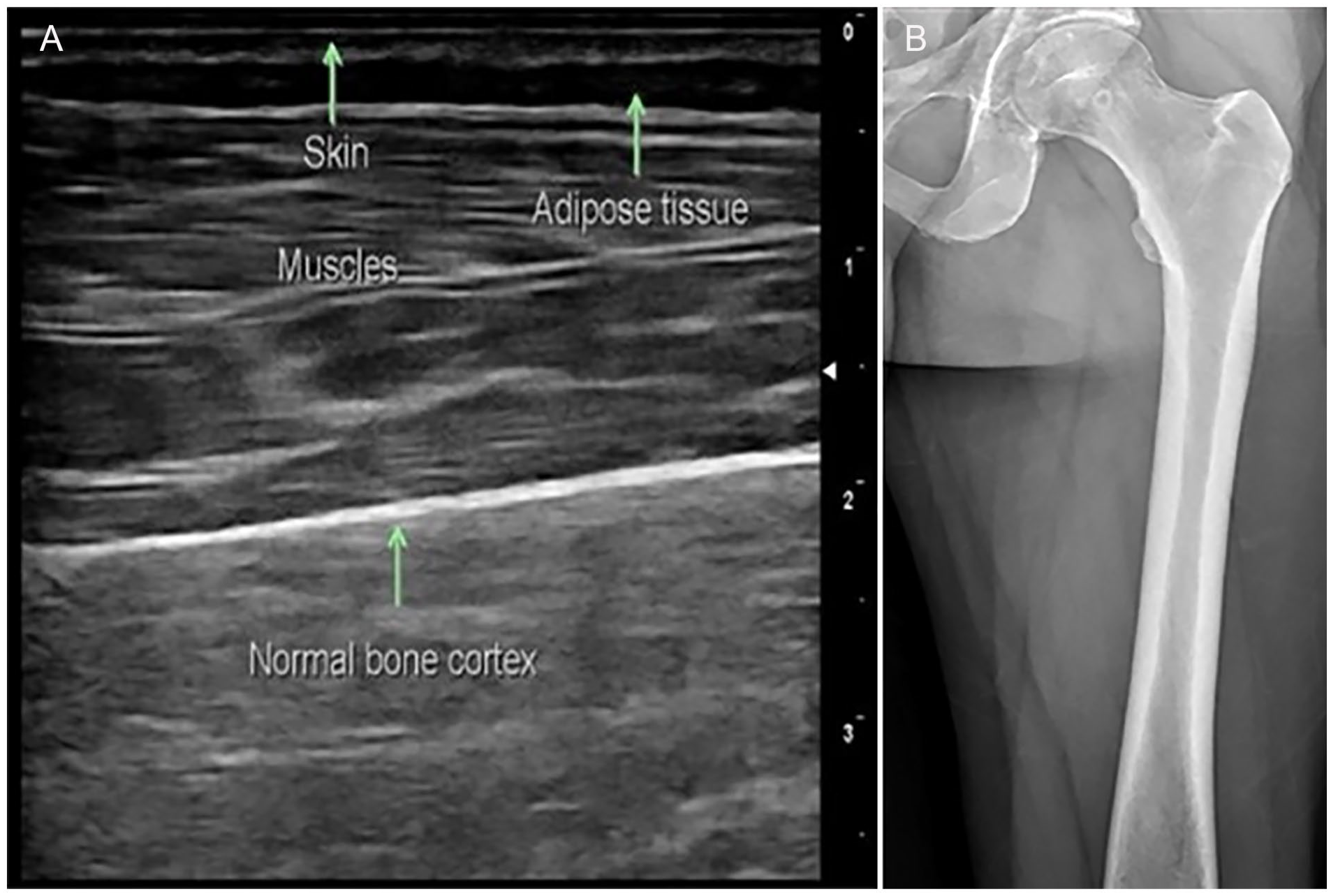
(A) A sonogram that demonstrates a hyperechoic bone cortex (normal). (B) A normal radiographic anteroposterior view, of the same patient’s femur.
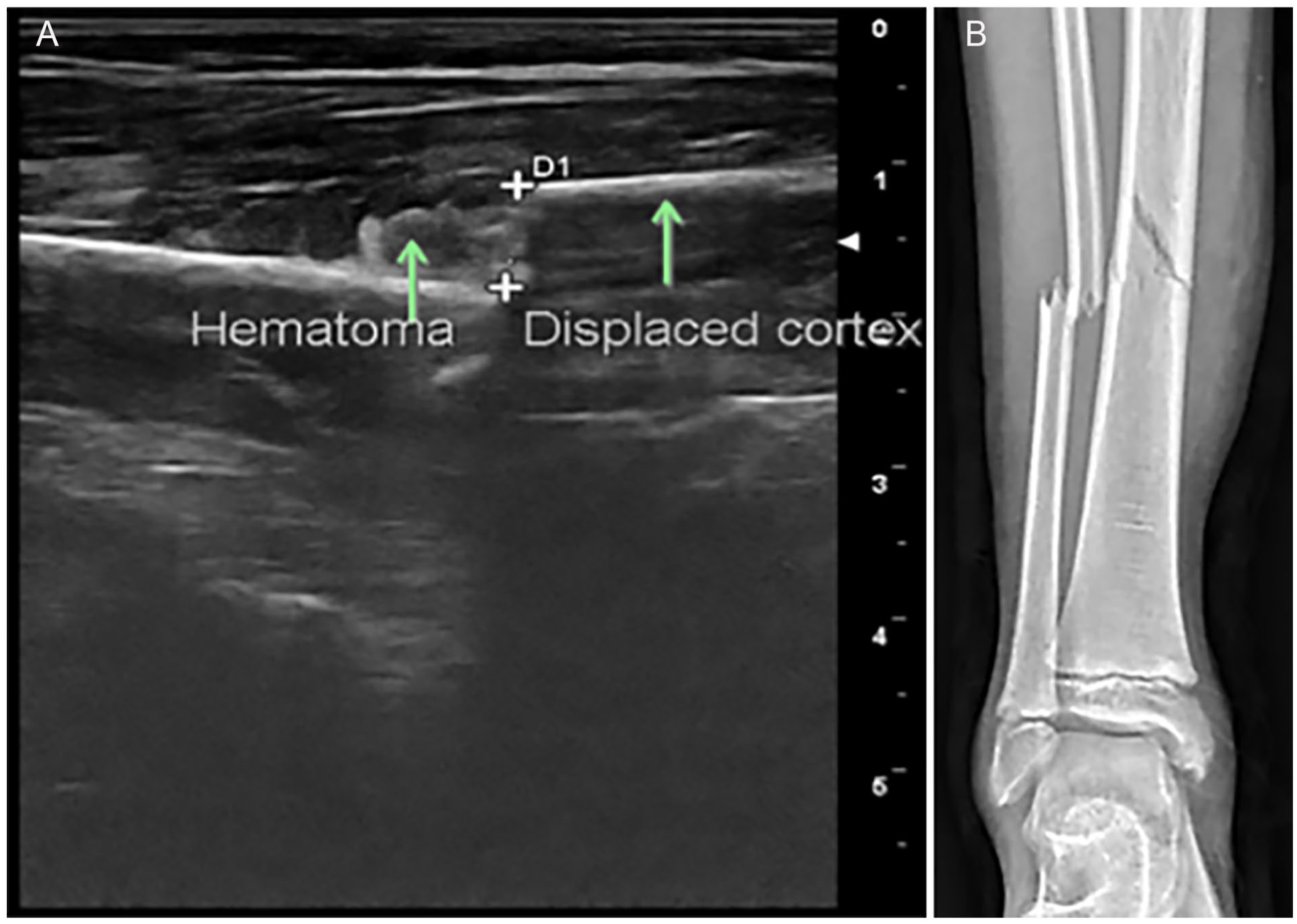
(A) A sonogram that demonstrates a “step-off” in the cortex surface of the fibula. (B) An anteroposterior radiographic view of the same patient’s tibia and fibula (fractures noted in both bones).
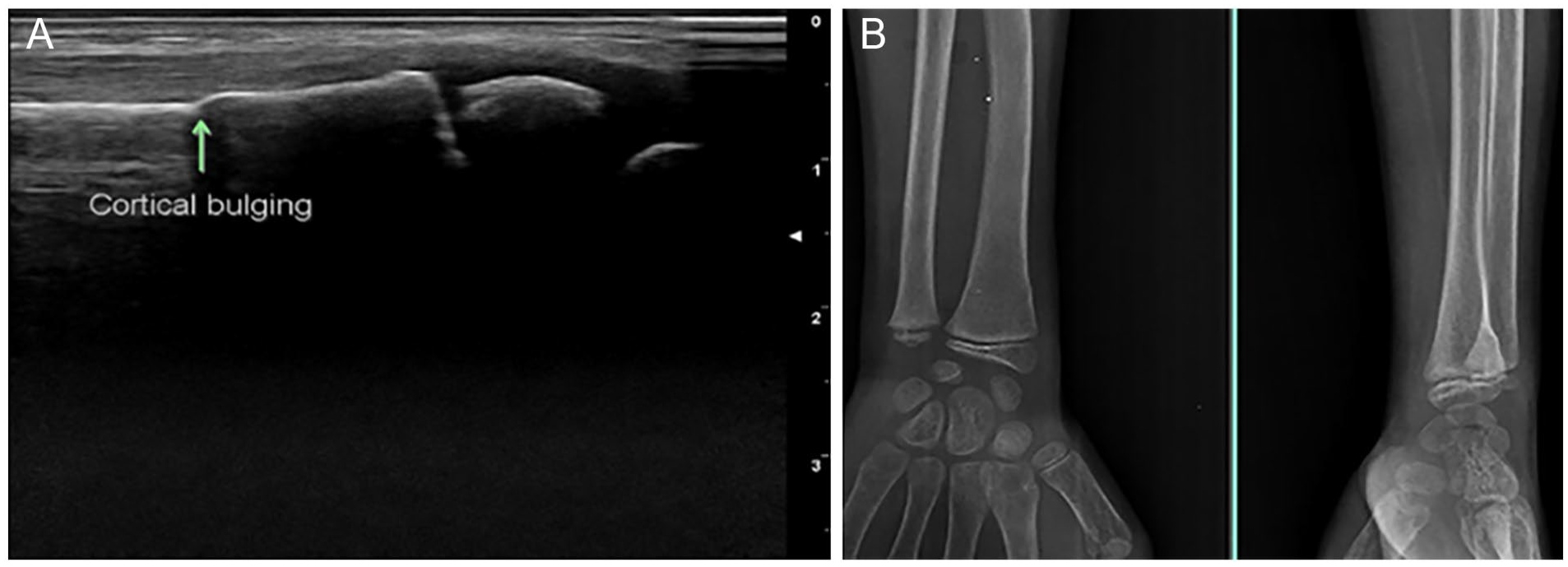
(A) A sonogram demonstrating a cortical bulging that would indicate a fracture. (B) Anteroposterior and lateral radiographic views of the forearm and wrist, which demonstrated a buckle fracture, on the same patient.
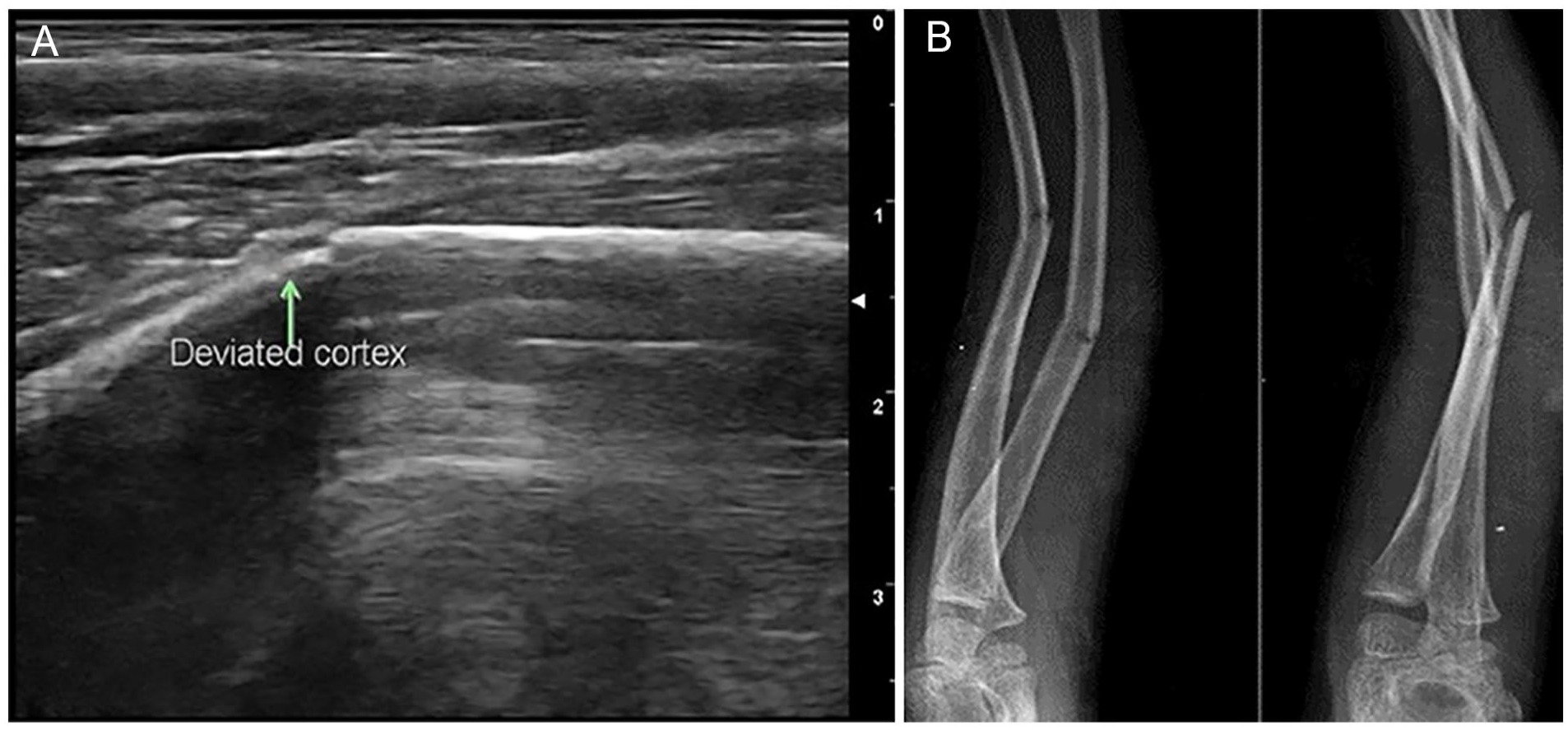
(A) A sonogram that captures a cortical deviation of the ulna, which indicates a fracture. (B) A radiographic set of views that confirms the fractures in the radius and ulna, on the same patient.
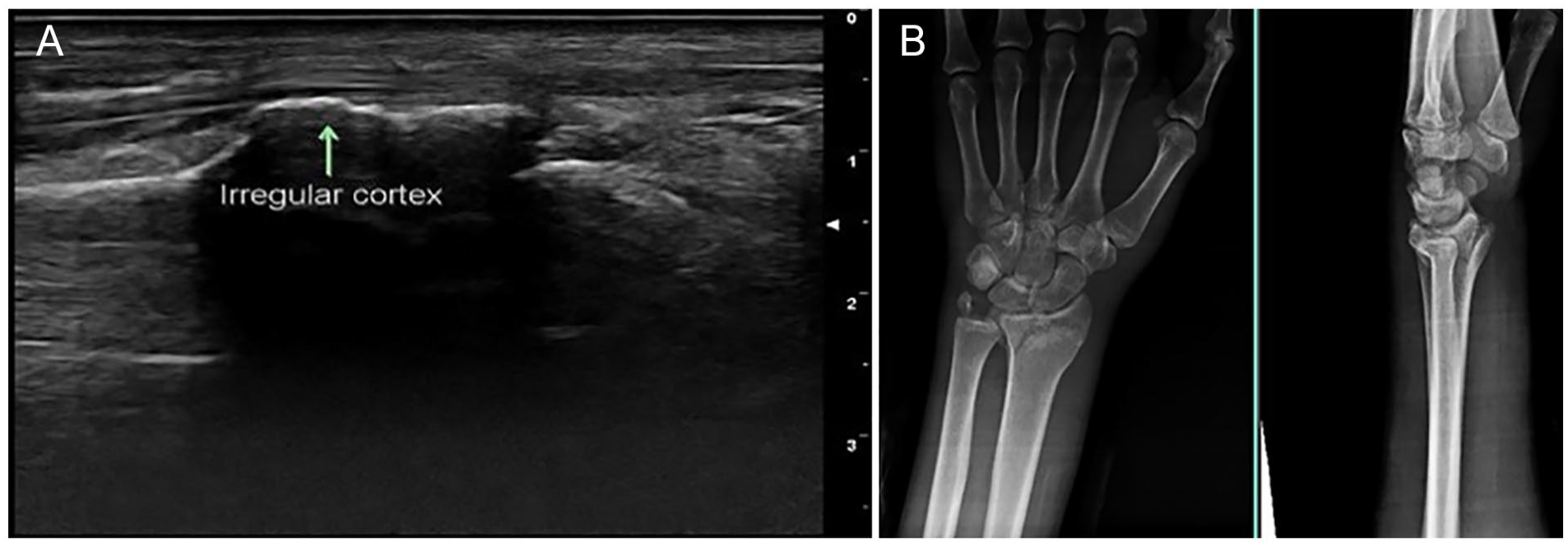
(A) A sonogram that demonstrates the cortical irregularity within the radius, which would indicate a fracture. (B) A posteroanterior and lateral radiographic views of the same patient’s wrist.
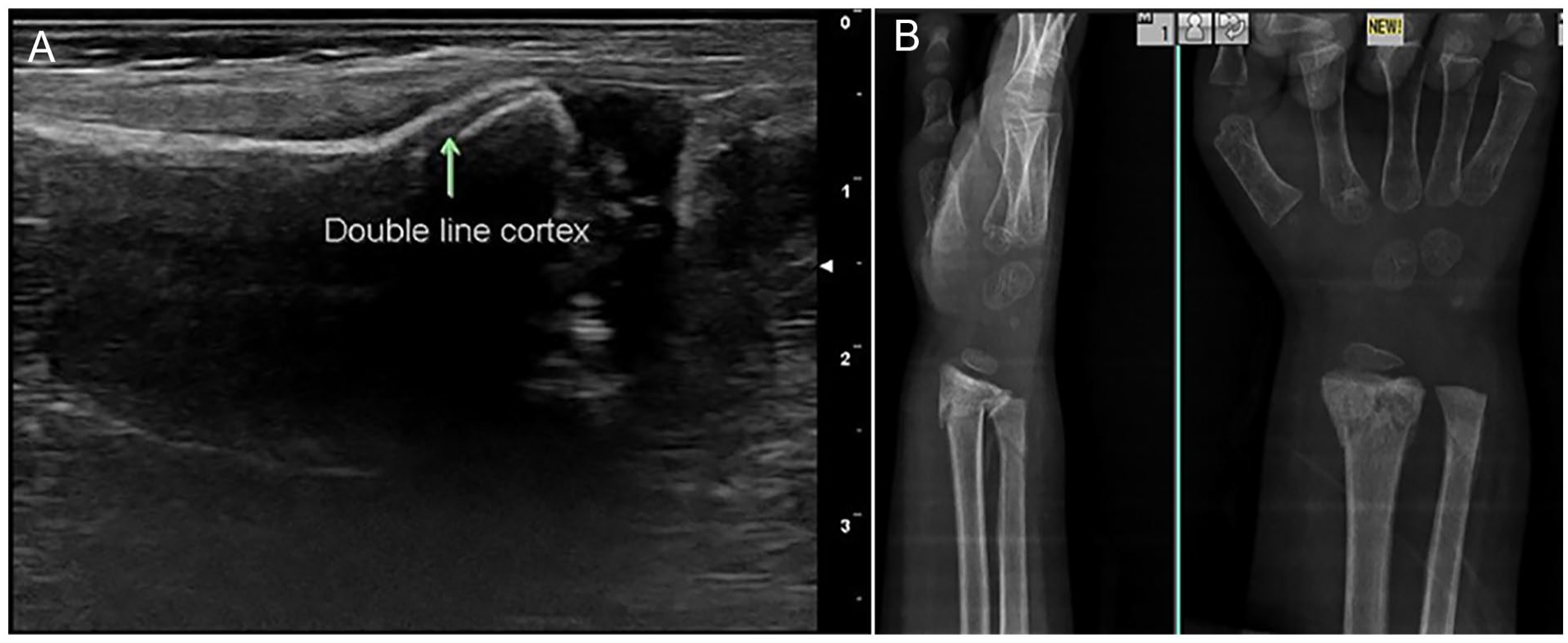
(A) A sonogram that shows a “double-line” cortex within the radius, which indicates a fracture. (B) A posteroanterior and lateral radiographic views of the same patient’s wrist and confirms fracture at the distal radius and ulna.
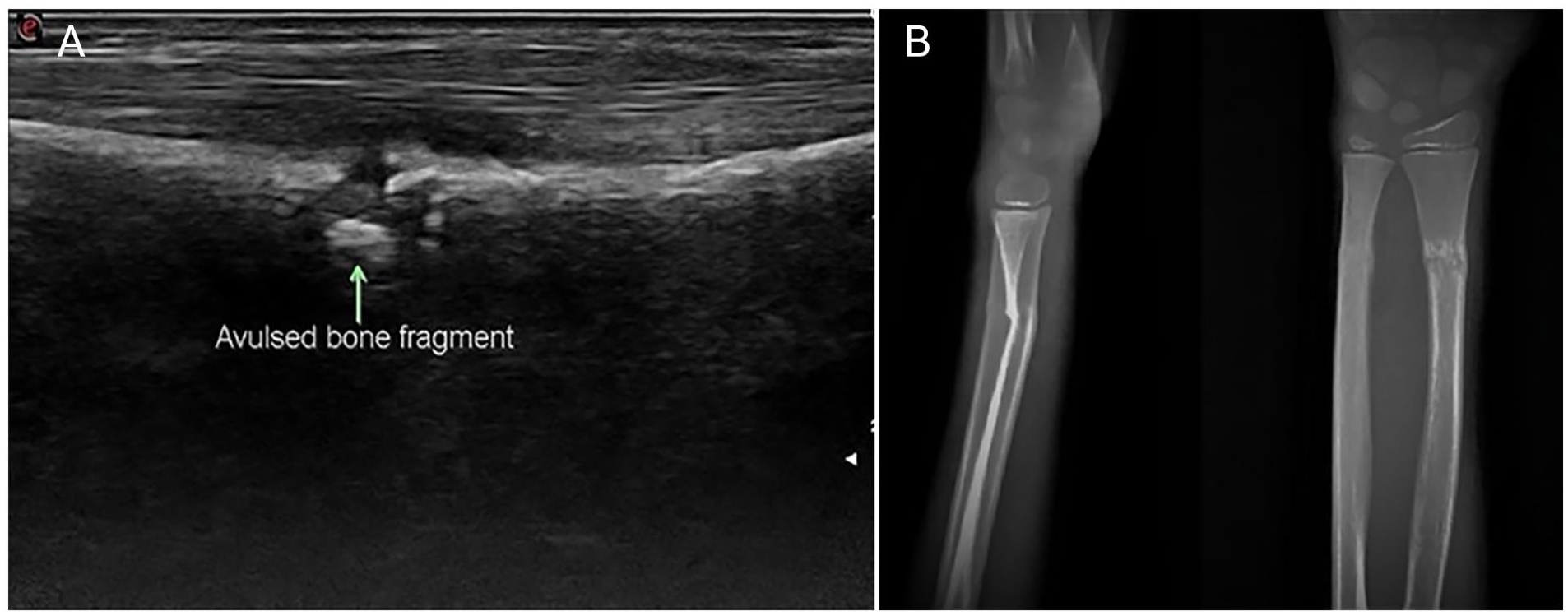
(A) A sonogram that shows an avulsed fragment within the radius. (B) A posteroanterior and lateral radiographic views of the same patient’s wrist that confirms a distal radial fracture.
The entire bone was assessed longitudinally in the anterior, posterior, medial, lateral and in their oblique positions, due to humeral and femoral injury. In case of the presence of two adjacent bones, additional medial and lateral oblique views were acquired both anteriorly and posteriorly. In case of fracture, the area of interest was re-evaluated axially to confirm the presence of the fracture. The sonographic findings obtained during the examination were documented on the study proforma. The presence or absence of fracture was declared sonographically, and the images and video clips were saved for future reference.
Radiographic Technique
Following the sonographic examination, the patients were referred to the radiographic examination room for imaging of the fracture. Using a high kilovoltage technique, mainly two standard projections, an anteroposterior and lateral views were obtained for the assessment of long bone fractures. An additional oblique view was also obtained where necessary, especially in the case of distal forearm fractures, to improve the diagnosis. Bony radiographs were obtained using a well-maintained AeroDR X70 (Konica Minolta, Tokyo, Japan), 1000 milliamperes radiographic equipment system, which is a digital radiography system. The digital radiography equipment underwent regular quality control measures to maintain the diagnostic range of both optical density and contrast, thereby ensuring consistent and quality imaging. Radiographic assessment of bone fractures involved evaluation of the cortical discontinuity, step-off in the cortex, displacement of bone fragments, or presence of impaction lines. Once presence or absence of fractures was declared radiographically, images were saved for future reference. Finally, all diagnostic images were viewed by a radiologist for the confirmation of the final diagnosis. The patients were referred to the orthopedic department for further treatment of their fracture.
Data Analysis
The data were analyzed with SPSS software version 29. Quantitative variables were reported in terms of frequencies and percentages. Pie charts and bar charts were used for the graphical presentation of qualitative variables. Fractures identified through sonography and radiography were categorized as either present or absent. The patient’s demographic information affected/fractured long bones, and the sonographic features were separately plotted based on their presence or absence in the sonographic evaluation.
The diagnostic accuracy of sonography was assessed in terms of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), as well as positive and negative likelihood ratios. The correlation between the sonographic and radiographic findings of fractures was determined by using the chi-squared test and Fisher’s exact test. A P value of 0.05 was established a priori.
Results
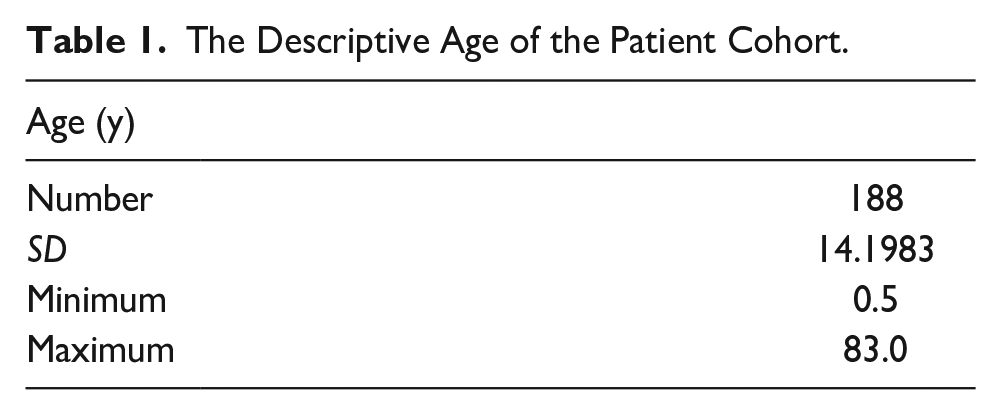
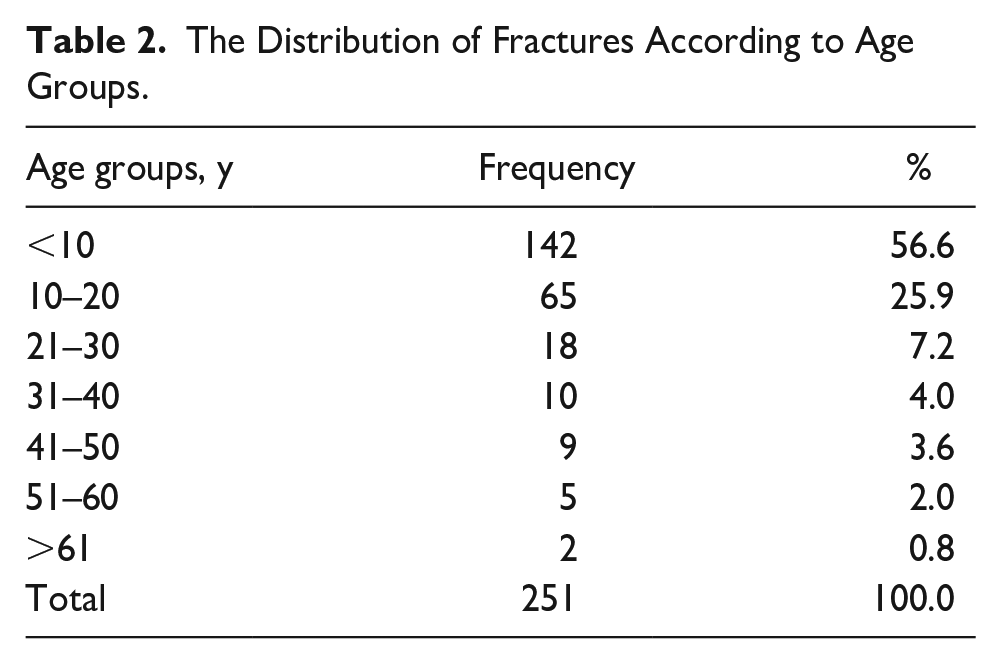
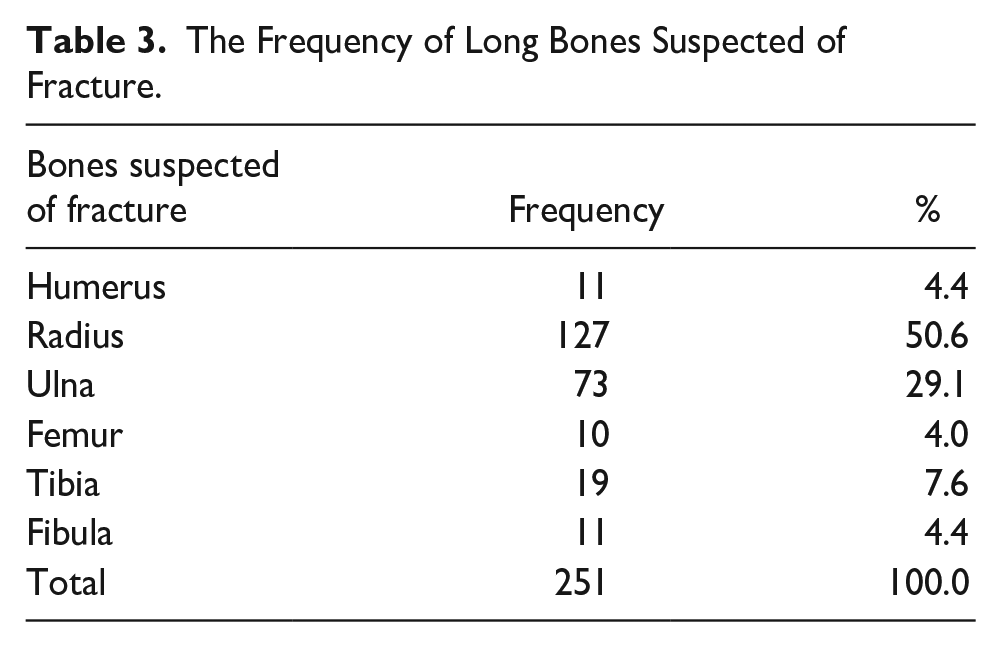
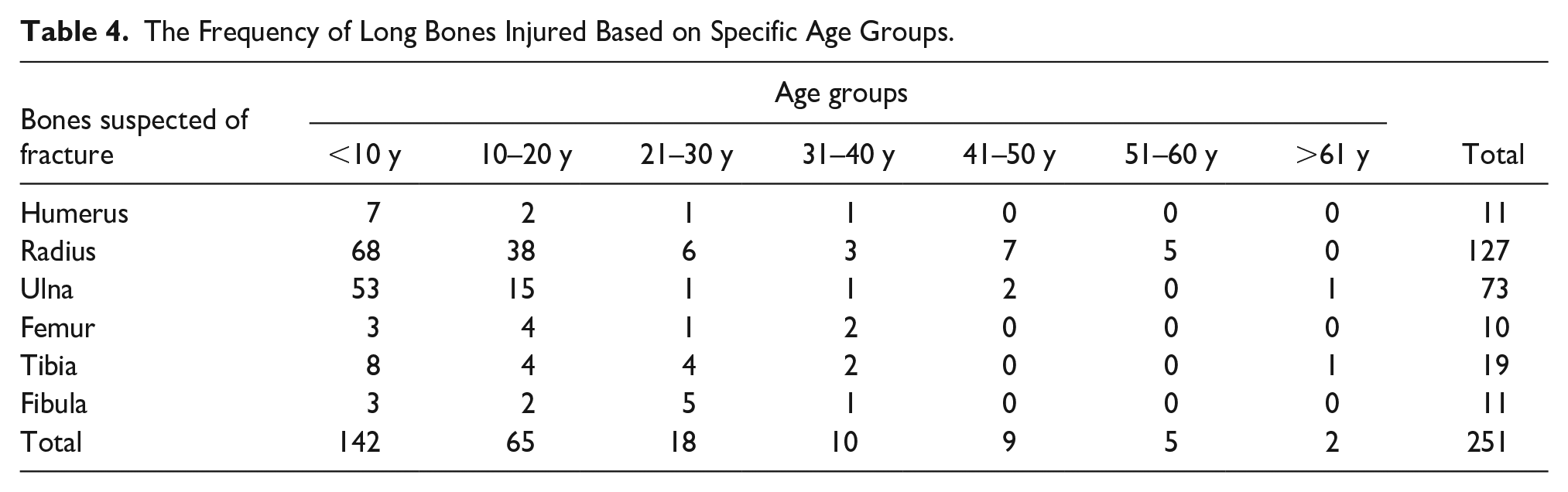
A total 188 patients, between 0 and 85 years of age, presented to the ED with a clinical suspicion of bone fracture were evaluated using sonography and radiography. A total of 251 suspected fractured bones were evaluated as some patients had multiple fractures. The age of patients consented to this study ranged from 0.5 to 83 years, with a mean age of 14.72 ± 14.19 years (see Table 1). Out of the total participants, 146 patients were males and 42 were females (see Figure 8). More than half of the participants (56.6%) were below the age of 10 years followed by the age group 10 to 20 years with a percentage of 25.9% (see Table 2). The majority of long bone injuries (84.1%) were reported in upper extremities while lower extremity injuries were 15.9% of the total (see Figure 9). Among the long bones evaluated, the radius was the most frequently fractured, accounting for 50.6% of all patient cases, followed by the ulna with a percentage of 29.1% (see Table 3). Fracture of the radius was commonly observed across all age groups, with the highest occurrence below 10 years of age, followed by the age group 10 to 20 years (see Table 4).
The Descriptive Age of the Patient Cohort.
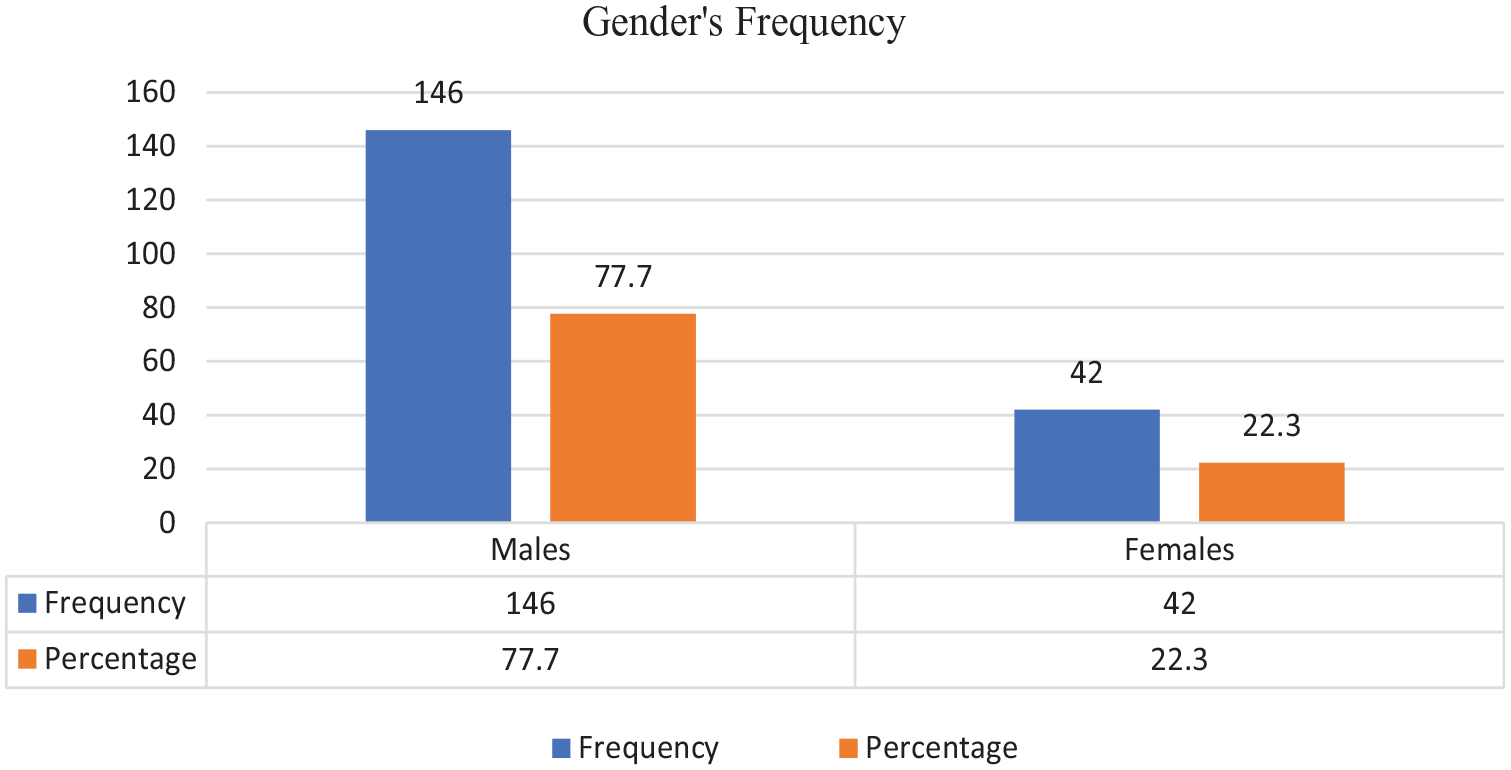
A bar chart providing the cohort’s gender distribution suspected of long bone fractures.
The Distribution of Fractures According to Age Groups.
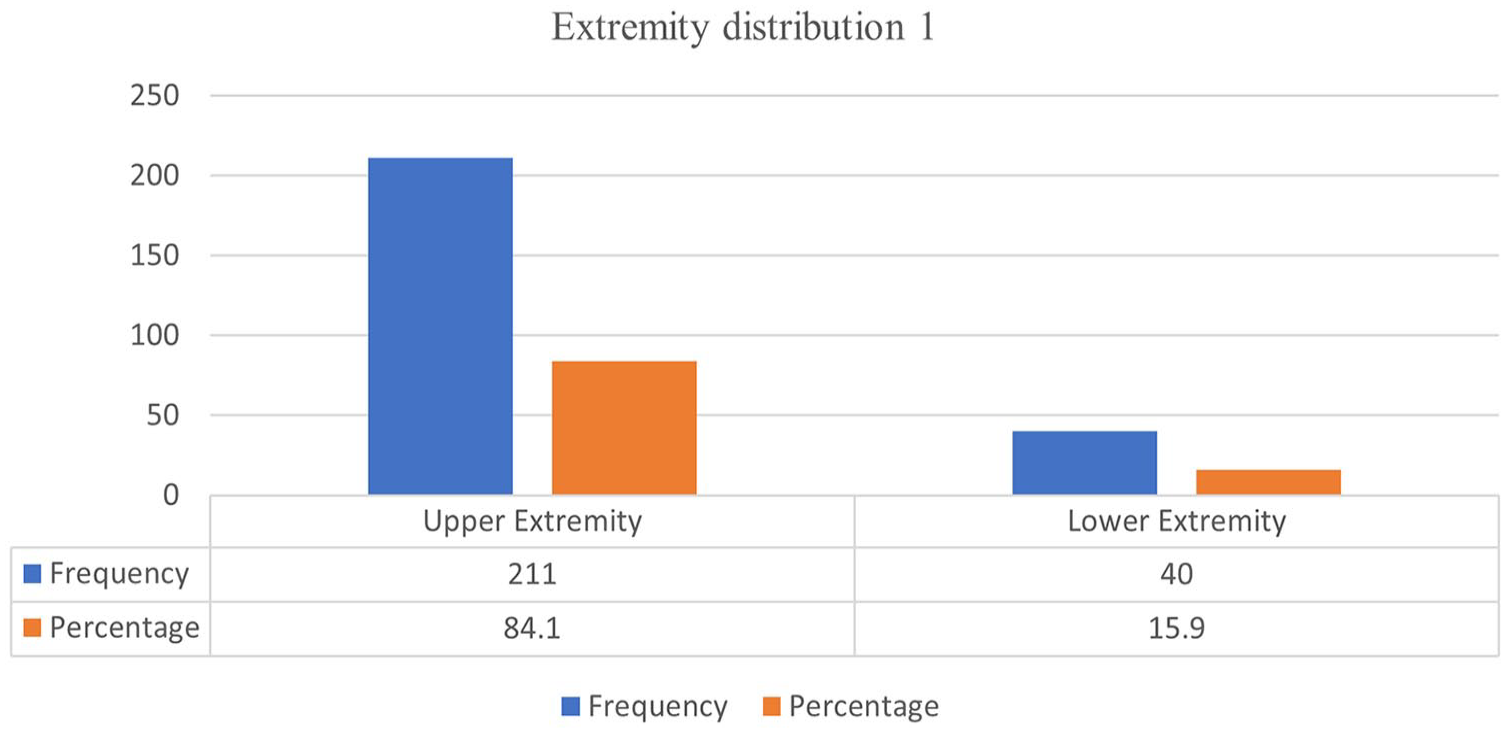
A bar chart that illustrates the distribution of upper and lower extremities suspected of fracture.
The Frequency of Long Bones Suspected of Fracture.
The Frequency of Long Bones Injured Based on Specific Age Groups.
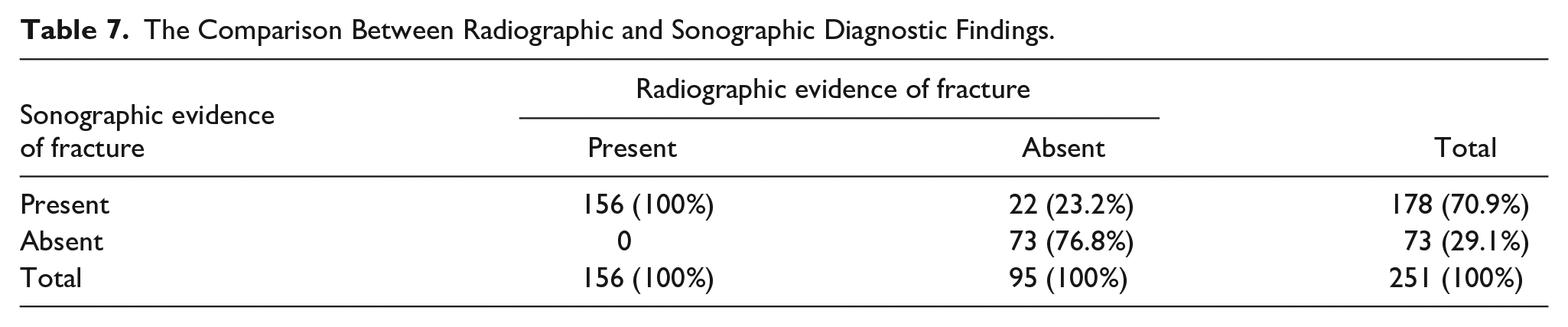
Falls were identified as the leading cause of long bone fractures, accounting for 85.1% of all cases, followed by RTAs, with a rate of 10.1%. Road traffic accidents were prevalent in the 10 to 20 years of age group constituting 40.1% of all cases, and all the sports-related injuries occurred within this age group (see Tables 5 and 6). Out of the 178 sonographic fractures detected in long bones, 156 were also confirmed by radiography, while 22 were not. Sonography failed to detect a fracture in 73 individuals while radiography did not reveal a fracture in 95 cases (see Table 7, Figure 10).
The Frequency of Fracture Causation.
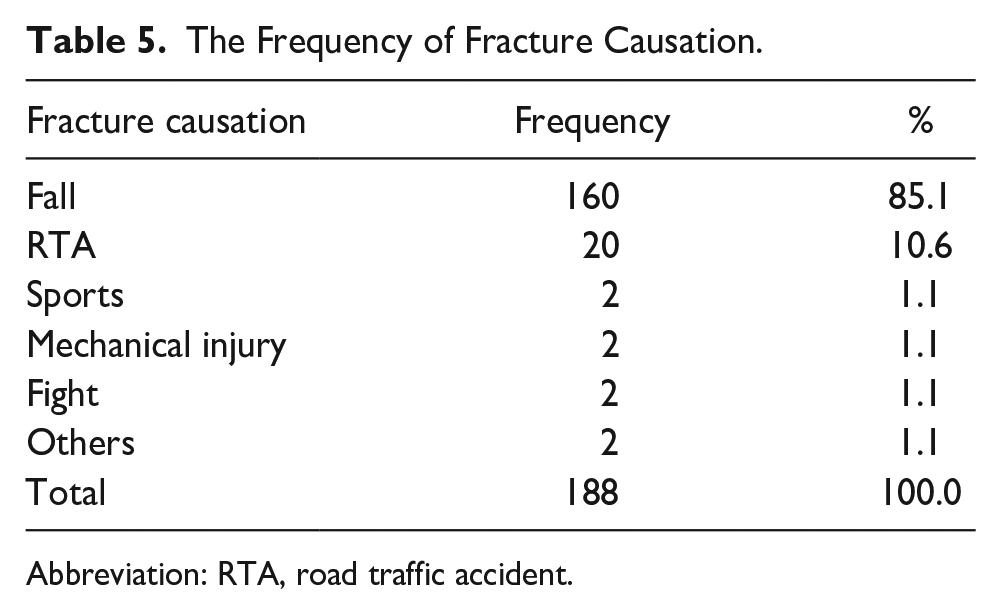
Abbreviation: RTA, road traffic accident.
The Frequency of Fracture Causation, Based on Age Groups.
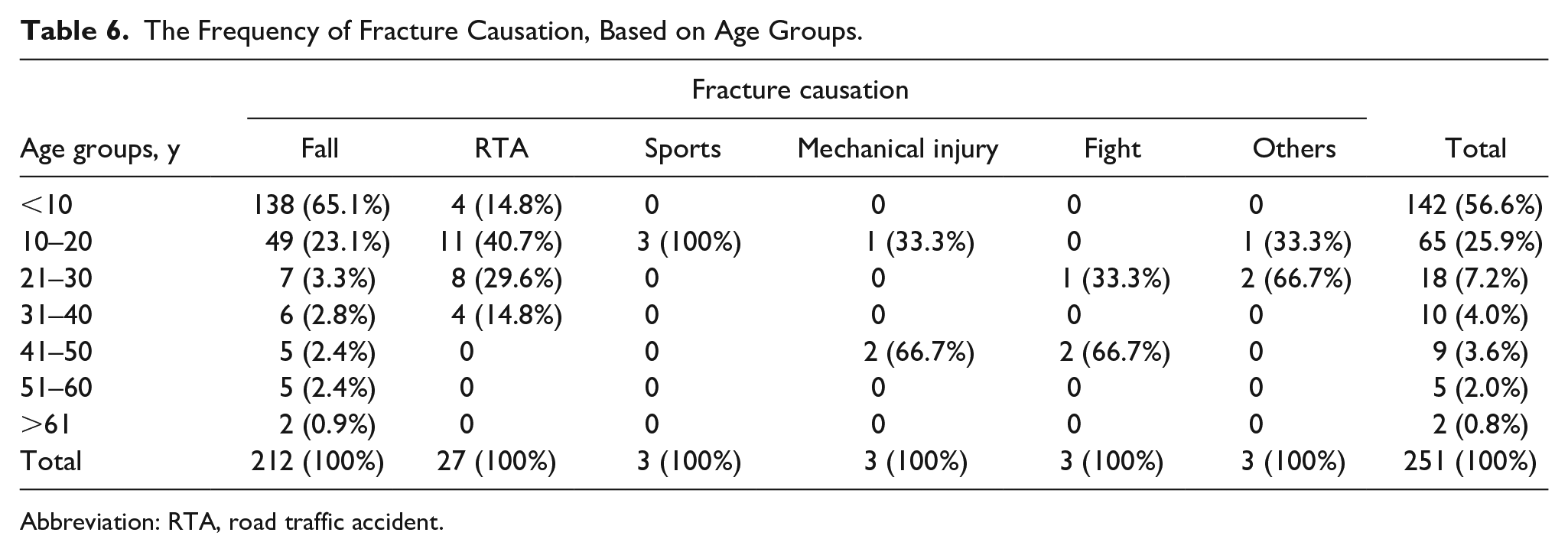
Abbreviation: RTA, road traffic accident.
The Comparison Between Radiographic and Sonographic Diagnostic Findings.
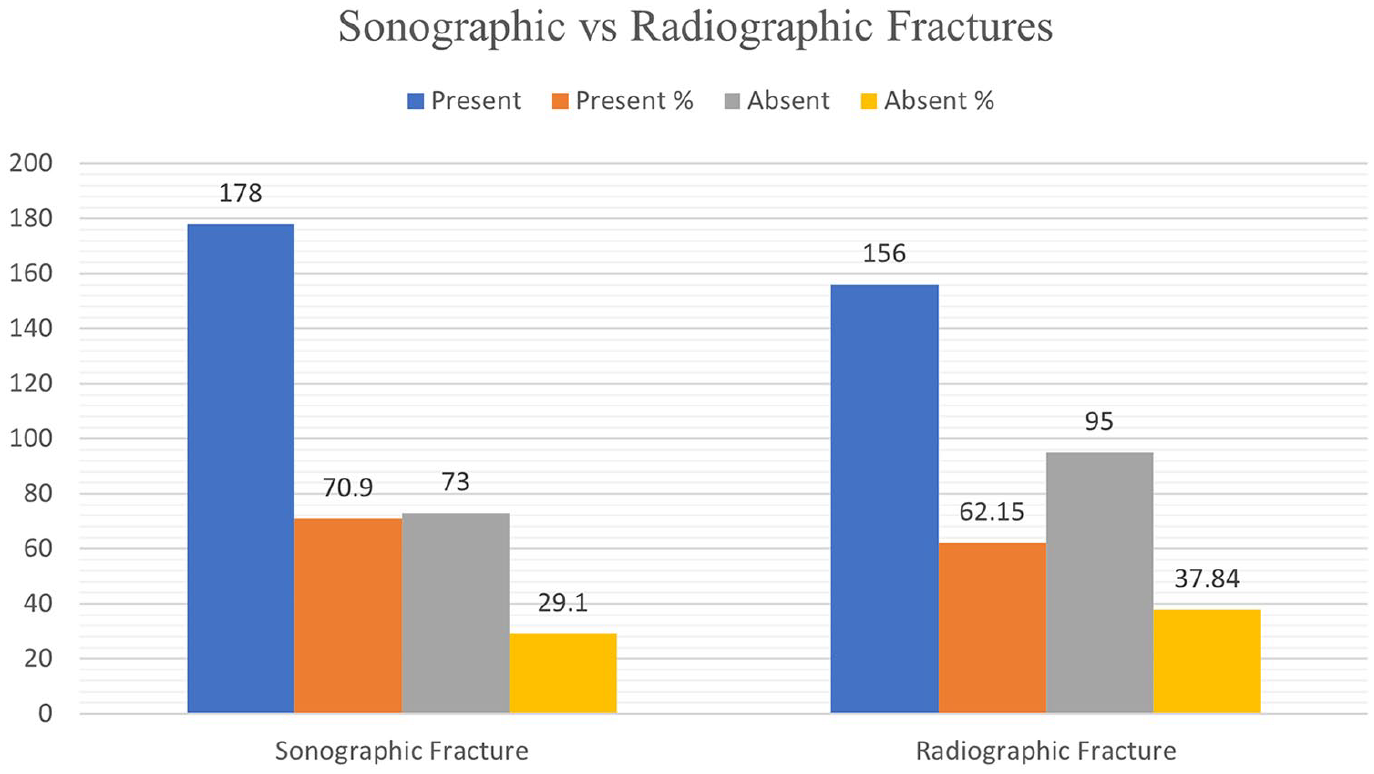
A bar chart that provides the distribution of fractures detected with sonography and radiography.
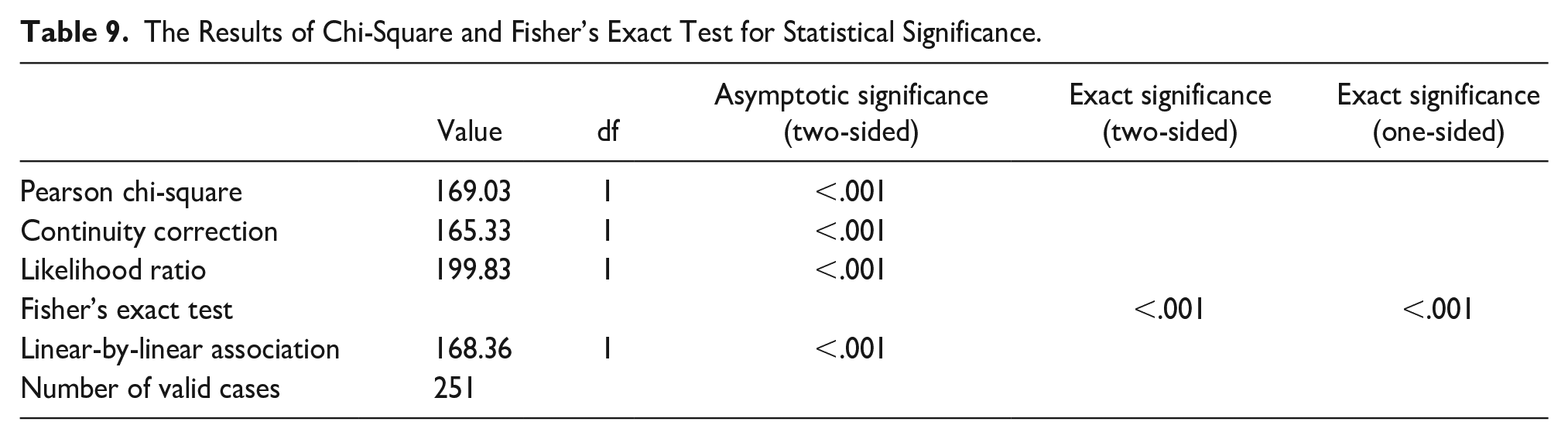
The sensitivity and specificity of sonography, in diagnosing long bone fractures, in this study were determined as 100% and 76.84%, respectively. The PPV and NPV were found to be 87.64% and 100%, respectively. The positive and negative likelihood ratios were estimated at 4.32 and 0.0, respectively. The overall diagnostic accuracy of sonography in diagnosing long bone fractures was calculated as 91.23% (see Table 8). The chi-squared test demonstrated a statistically significance, at a P value of lesser than 0.001 (see Table 9).
Diagnostic Accuracy of Sonographic Diagnosis for Fracture.
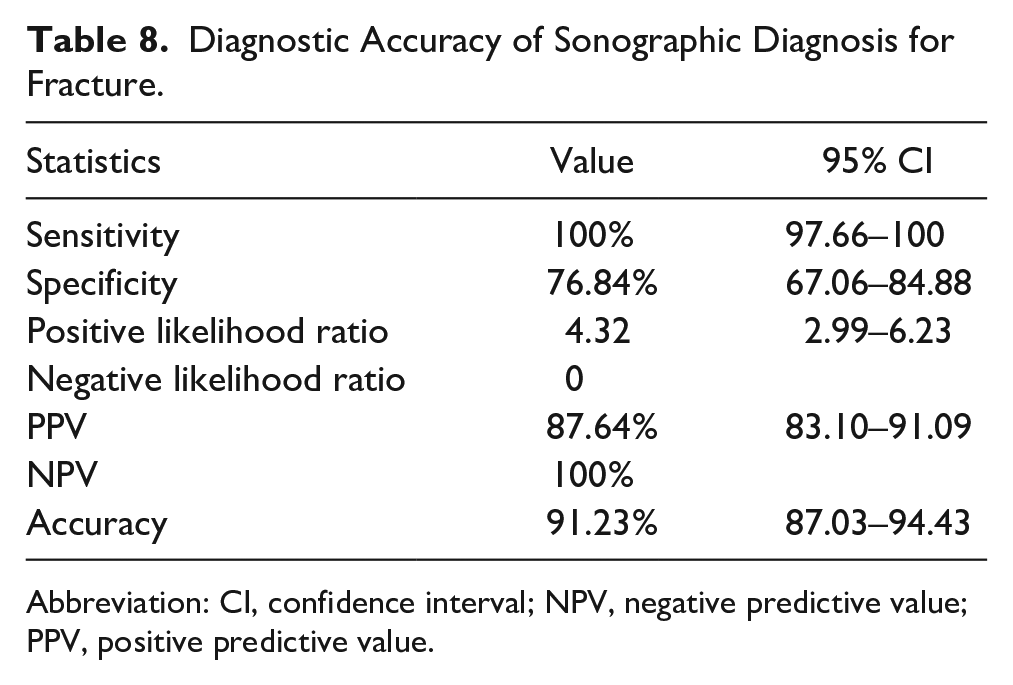
Abbreviation: CI, confidence interval; NPV, negative predictive value; PPV, positive predictive value.
The Results of Chi-Square and Fisher’s Exact Test for Statistical Significance.
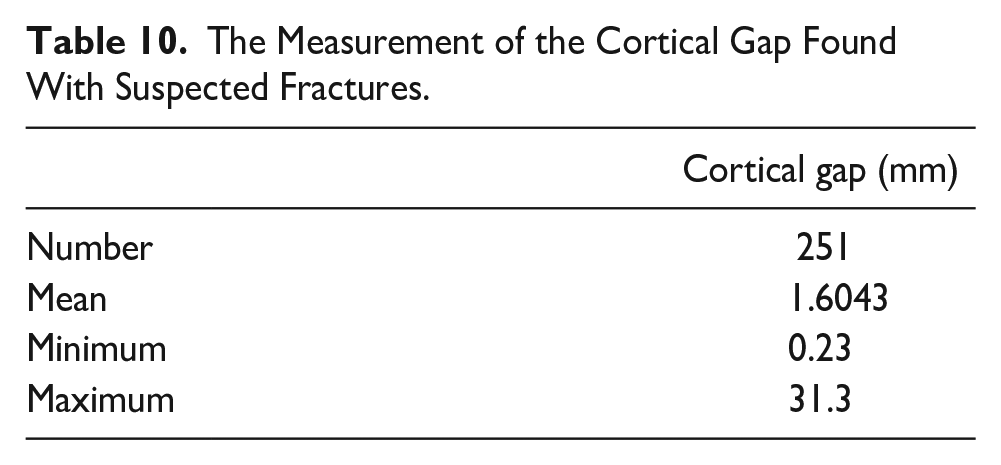
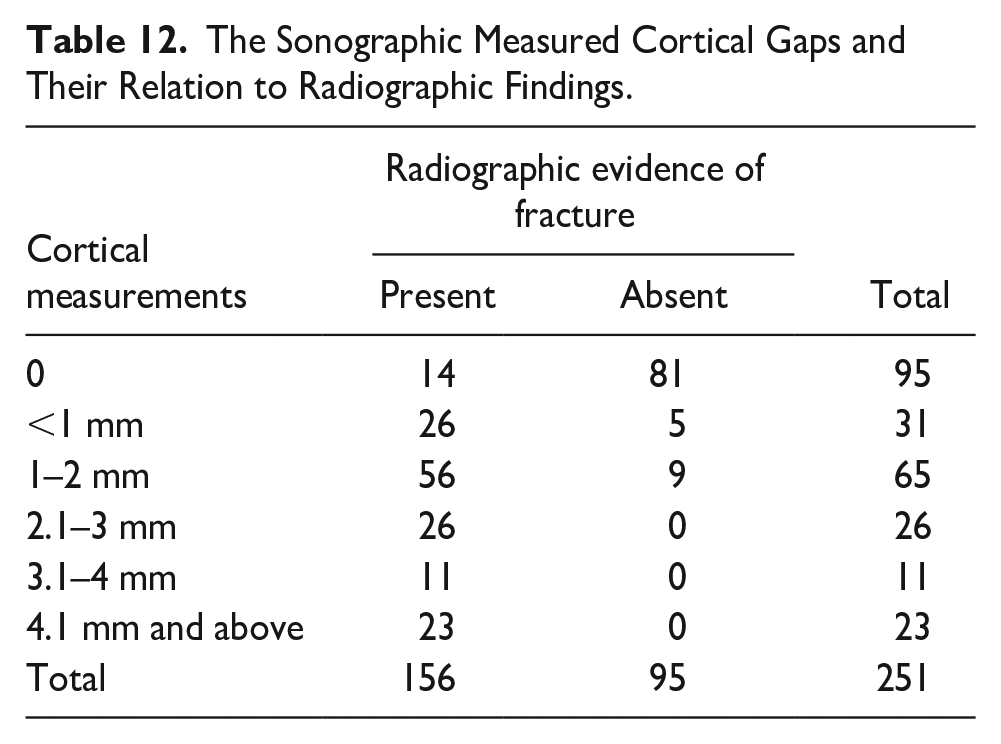
Sonography could detect a cortical gap present in fractures as small as 0.23 mm (see Table 10). In 37.8% of patient cases, no cortical gaps were observed. The most common encountered cortical gaps were within the range of 1.0 to 2.0 mm and accounted for 25.9% of all patient cases; however, radiography missed nine patient cases. In addition, five of the cortical gaps measuring less than 1.0 mm, as detected sonographically, were not identified with radiography (see Tables 11 and 12).
The Measurement of the Cortical Gap Found With Suspected Fractures.
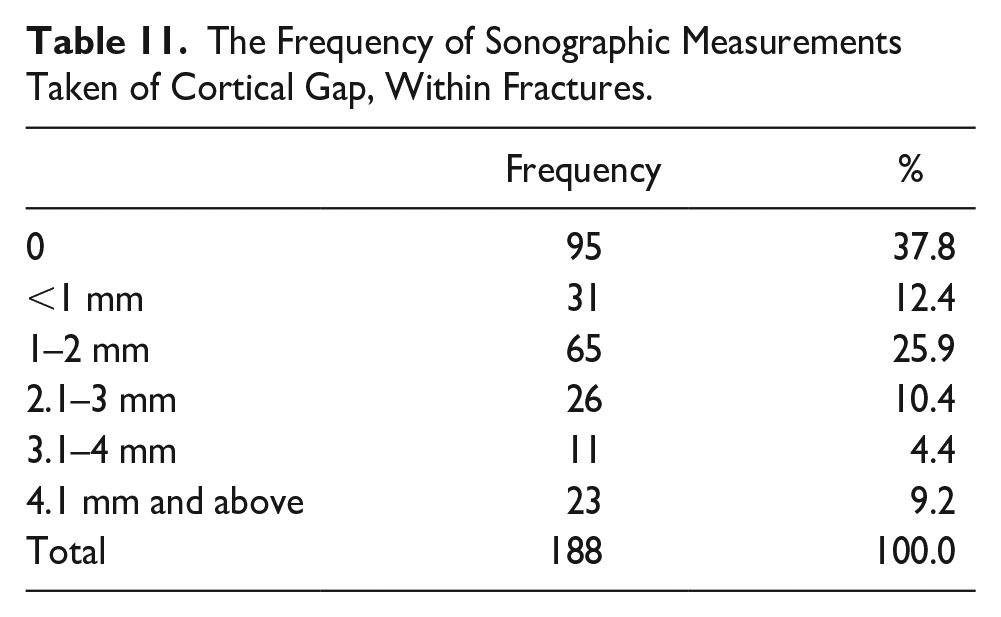
The Frequency of Sonographic Measurements Taken of Cortical Gap, Within Fractures.
The Sonographic Measured Cortical Gaps and Their Relation to Radiographic Findings.
Discussion
The primary objective of this study was to assess the diagnostic accuracy of sonography as an alternative imaging technique to radiography, for the diagnosis of long bone fractures, in post-traumatic patients. Furthermore, an additional aim of the study was to investigate the capability of sonography to identify fractures with a cortical gap of less than 1 mm. This assessment was motivated by the previous literature indicating that sonography can detect fractures up to a cortical gap of 1.0 mm. In addition to the stated objectives, this study was designed to evaluate the diagnostic accuracy of sonography when operated by a skilled sonographer. The data collected within this cohort did indicate that sonography exhibited a notable diagnostic accuracy in the detection of long bone fractures, as evidenced by the significant values of sensitivity, specificity, PPV, and NPV. Statistical analysis, using a chi-squared test and Fisher’s exact test, revealed a significant association between the sonographic and radiographic findings (P < .001). In this cohort, sonography exhibited superior sensitivity compared with radiography, enabling the identification of fractures in submillimeters that might have been missed by a radiographic examination. Furthermore, the results demonstrate that sonography demonstrated a consistent diagnostic sensitivity across all age groups and genders.
Sonography has been shown to possess a high level of accuracy in diagnosing long bone fractures, as demonstrated by Caroselli et al. In their study, the sensitivity, specificity, PPV, and NPV of sonography in detecting bone fractures of various types were determined to be 93.89%, 94.13%, 88.48%, and 96.98%, respectively. 24 This study yielded comparable results with a sensitivity, specificity, PPV, and NPV of 100%, 76.84%, 87.64%, and 100%, respectively. However, there was a slight increase in sensitivity and a noticeable decrease in specificity when compared with the study of Caroselli et al. Several factors may contribute to these variations, including the inclusion of all types of skeletal bones other than long bones in their study and the utilization of two hospitals and two radiologists for performing sonography.
Similarly, Akinmade et al. 13 evaluated the sensitivity, specificity, PPV, and NPV of sonography for pediatric long bone fractures as 96.2%, 100%, 100%, and 83.3%, respectively. In this study, a slightly higher sensitivity was observed but a noticeably lower specificity compared with their findings. Possible reasons for these differences may include a smaller sample size and the use of low frequency (5.0 MHz) transducer, which resulted in missing two fractures, sonographically.
In another study conducted by Avci et al., sonography was compared with radiography, for the diagnosis of long bone fractures. Their study revealed the sensitivity, specificity, PPV, and NPV of sonography as 99%, 93%, 93%, and 99%, respectively. 12 The findings of this study align with these results except for the specificity which is lower than the Avic et al. findings. Several factors may contribute to this difference including the use of a lower frequency transducer (7.5 MHz) and the examinations being performed by five ED physicians, rather than a single operator. Notably, Avci et al. identified six sonographic fractures which were not detected radiographically. The sensitivity of both studies remains comparable, likely due to a similar sample size. In addition, the change in specificity may be due to the use of high-frequency transducer (15 MHz), in this study, which lead to enhanced sonographic resolution. Consequently, this study identified 22 fractures that were missed radiographically, thereby contributing to the lower specificity observed.
The sensitivity and specificity observed in this study, which are determined to be 100% and 76.84%, respectively, are in line with the values reported in a recent systematic review conducted by Li and Tan. The review was composed of several studies, and the sensitivities ranged from 85% to 100%, while the specificities ranged from 73% to 100%, respectively. 6 These findings further support the consistency of this study’s results with the existing body of scientific literature. This could indicate that this study’s diagnostic performance aligns with the reported range of sensitivities and specificities in the published literature.
All of the parameters of this study are aligned to the aforementioned publications, conducted to evaluate the accuracy of long bone sonography, except for the specificity which stands out comparatively lower than those studies. This difference may be due to the inverse relationship between the sensitivity and specificity, as sensitivity increases, specificity tends to decrease. The higher the sensitivity, the higher the positive cases of a disease. 25
Among the total of 251 suspected fractures examined in this study, 178 cases were sonographically determined as positive for fracture, out of which 22 were not detected radiographically. These findings may support the existing evidence that radiography is not a highly sensitive technique to diagnose all fractures, compared with sonography. This statement is validated by Al-Baghdadi et al., in their case series to compare radiography and sonography in detecting bone fractures. Their study revealed that several suspected long bone fractures were not identified by radiography but were successfully diagnosed the same day by using sonography. 26 This is again favored by Scholl and Knupp’s case report, in which a 74-year-old patient with ankle trauma was initially diagnosed using sonography. The patient was then evaluated radiographically, as well as with a coned beam tomogram; however, the fracture was not demonstrated. A CT ankle was performed for the patient which detected a fracture at the distal tibia. 27
Keeping the mentioned case report and series into consideration, a CT was performed on one of the 22 patients from this study cohort, who were sonographically diagnosed as having fractures, but declared negative radiographically. The use of a multidetector CT equipment system revealed the presence of fracture (see Figure 11C), which confirms that some positive cases of fractures can be missed radiographically, resulting in increased sensitivity of sonography.
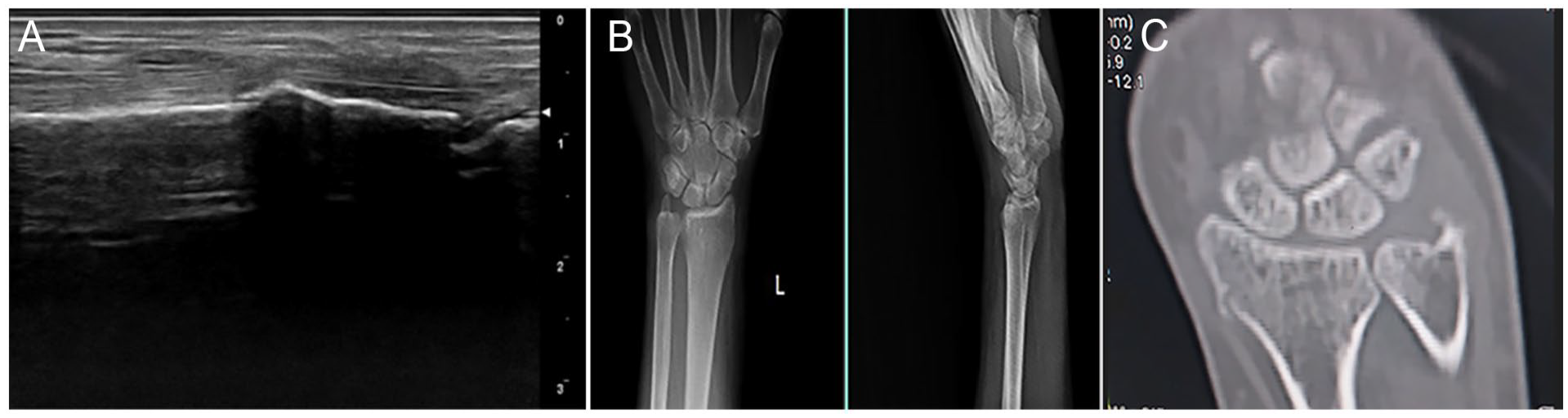
(A) A sonogram that shows a cortical gap along the surface of the bone. (B) A posteroanterior and lateral radiographic views, which do not demonstrate a fracture within the distal forearm and wrist. (C) A computed tomogram of the wrist and distal upper extremity, of the same patient, which shows a fracture.
The accuracy of sonography is user-dependent affecting the sensitivity and specificity of ultrasound. Iacob et al. demonstrated that the sensitivity and specificity of sonography were higher when operated by experienced operators compared with those with minimal training. In their study, sonography performed by a radiologist yielded a sensitivity of 91.1% and specificity of 97.6%. The results of the ED physicians were nearly identical to those of the radiologists, with a sensitivity and specificity of 91.5% and 96.8%, respectively. 28 However, when the sonograms were performed by the medical students, the sensitivity and specificity decreased to 75% and 89.5%, respectively. 14 The sensitivity and specificity of sonography raised to 94.6% and 85.3%, respectively, when the examinations were performed by nurse practitioners. 29
In this study, sonograms were performed by a skilled sonographer resulting in a sensitivity of 100%. This would suggest that the high level of expertise possessed by the skilled sonographer impacts the accuracy of sonography, in detecting bone fractures. Akinmade et al. 13 highlighted that sonography can detect fractures as small as 1.0 mm. However contrary to this assertion, the results in this study revealed that sonography can detect a fracture of size as small as to 0.23 mm (see Figure 12B), when employing a high-frequency transducer (15 MHz), capable of producing high-resolution images. The findings of this study demonstrated that among the fractures detected by sonography, 25 cases had cortical gaps of less than 1.0 mm, while 46 fractures were diagnosed with cortical gaps of 1.0 to 2.0 mm. Among these patient cases, radiography failed to identify five patients with fractures less than 1.0 mm and nine patients with fractures between 1.0 and 2.0 mm.
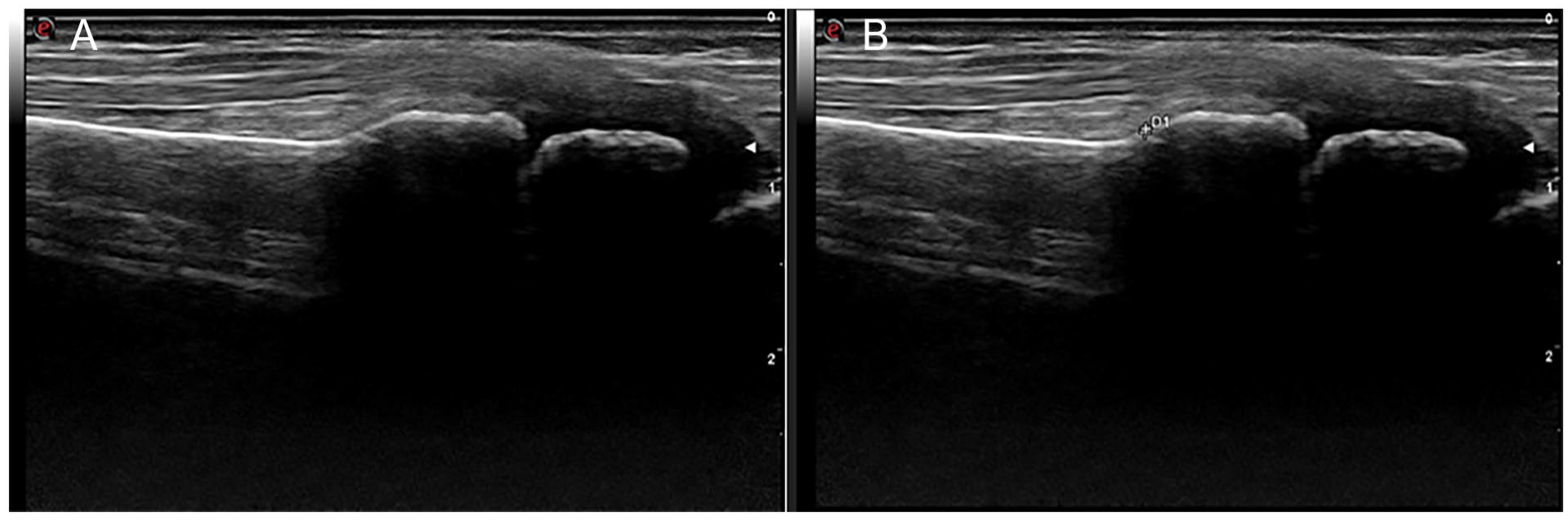
(A) A sonogram of the distal upper extremity which demonstrates a small cortical gap in the bone surface. (B) A sonogram of the distal upper extremity that shows a cortical gap that measures 0.23 mm.
Limitations
The major limitation to this study is the research design and the use of a convenient sample of patients. Another notable limitation of this study pertains to the use of radiography as the reference standard instead of CT, due to limited resources. Computed tomography offers high sensitivity and specificity in detecting long bone fractures. The use of CT as a diagnostic reference standard would have provided a more comprehensive evaluation of sonography’s diagnostic accuracy. Furthermore, findings of this study cannot be fully generalizable due to threats to internal and external validity as well as the high number of young patients, particularly those under 20 years of age presenting with forearm fractures.
Conclusion
This study demonstrated that sonography had a good diagnostic accuracy, in diagnosing long bone fractures. Sonography was a useful, cost-effective, portable, and versatile diagnostic alternative to radiography, which can lead to a drastic reduction in unnecessary radiographs, as well as reducing patient’s radiation dose, especially among the children. The diagnostic accuracy of sonography is likely influenced by the expertise of the operator, with a skilled sonographer achieving the best diagnostic results. Moreover, sonography can detect small fractures measuring less than 1.0 mm, using high-frequency transducers. These findings may further support the utility of sonography as a potential diagnostic tool for the diagnosis of long bone fractures, in clinical practice.
Footnotes
Acknowledgements
The authors would like to thank all the imaging technologists of the ED, Saidu Group of teaching Hospitals Saidu Sharif, Swat especially to Saeed Ullah, Rahim Zada, Abdullah, Aizaz, Sheraz, and Hamza for taking quality radiographs and saving them for future use. They also thank DR Bahadar Ali for his precious time taken for discussing and finalizing fractures of the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from the Institutional Review Board, at the University of Lahore, Pakistan (IRB#: REC-UOL-/240-09/2022).
Informed Consent
Informed consent informed consents were obtained and then de identified and/or aggregated and followed ethics committee or institutional review board guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to this study because animals were not used in the study.
Trial Registration.
Not applicable.