
Abstract
This case report describes a patient who presented with cholangitis gallbladder sludge, choledocolithiasis, and biliary dilatation. The patient’s magnetic resonance cholangiopancreatography demonstrated that the cystic duct had low and medial insertion on common bile duct. However, the patient presented with abdominal discomfort after the completion of an endoscopic retrograde cholangiopancreatography stenting. Subsequent imaging revealed the proximal stent lying in the gallbladder lumen. The case highlights the importance of having the endoscopists recheck and confirm the positioning of the stent, post-procedure. In addition, it is important to raise awareness among physicians/gastroenterologists regarding the possibility of presence of biliary stent in gallbladder lumen, especially in those patients with a history of endoscopic biliary intervention(s).
Keywords
Endoscopic biliary stenting is a well-accepted therapy for biliary obstruction, which has developed due to malignant or benign disease. Stent migration is an uncommon complication that may be seen in 5% to 10% of patients who have undergone endoscopic stenting. 1 Both proximal as well as distal migration of stent has been described; however, migration of stent in lumen of gallbladder is believed to be extremely rare and is an unusual complication. A case is presented of a patient with cholangitis and presenting with abdominal discomfort after endoscopic retrograde cholangiopancreatography (ERCP) stenting. Upon subsequent imaging of this patient, it was revealed that the proximal stent was lying in the gallbladder lumen.
Case Report
A 55-year-old woman presented with epigastric pain and abdominal bloating for 1 month. An abdominal sonogram and a magnetic resonance cholangiopancreatography (MRCP) demonstrated that there was sludge in the gallbladder (GB), as well as choledocolithiasis with biliary dilatation. Based on these imaging results, the cystic duct had a low and medial insertion into the common bile duct. The combined results of the clinical examination and blood biomarkers suggested that the patient had obstructive jaundice with mild cholangitis.
The patient was taken up for ERCP stenting for biliary decompression. A 7-French 10.0 cm double-pigtail plastic stent was inserted in the common bile duct. The deployment of the stent was smooth with no patient complications. A colangiogram was not done for this patient in view of having cholangitis. The post-ERCP course of recovery was uneventful, and the patient was advised to return after 6 weeks. However, the patient came back after 3 weeks with abdominal discomfort. An abdomen sonogram revealed the proximal end of stent in the GB and, in addition, sludge was seen within the lumen (see Figures 1–3). Another calculus was seen in the proximal common bile duct along with the stent in its distal part. There was associated mild dilatation of the intrahepatic biliary radicals, within the liver. All these diagnostic findings were confirmed on the computed tomogram, which was subsequently completed (see Figures 4 and 5).
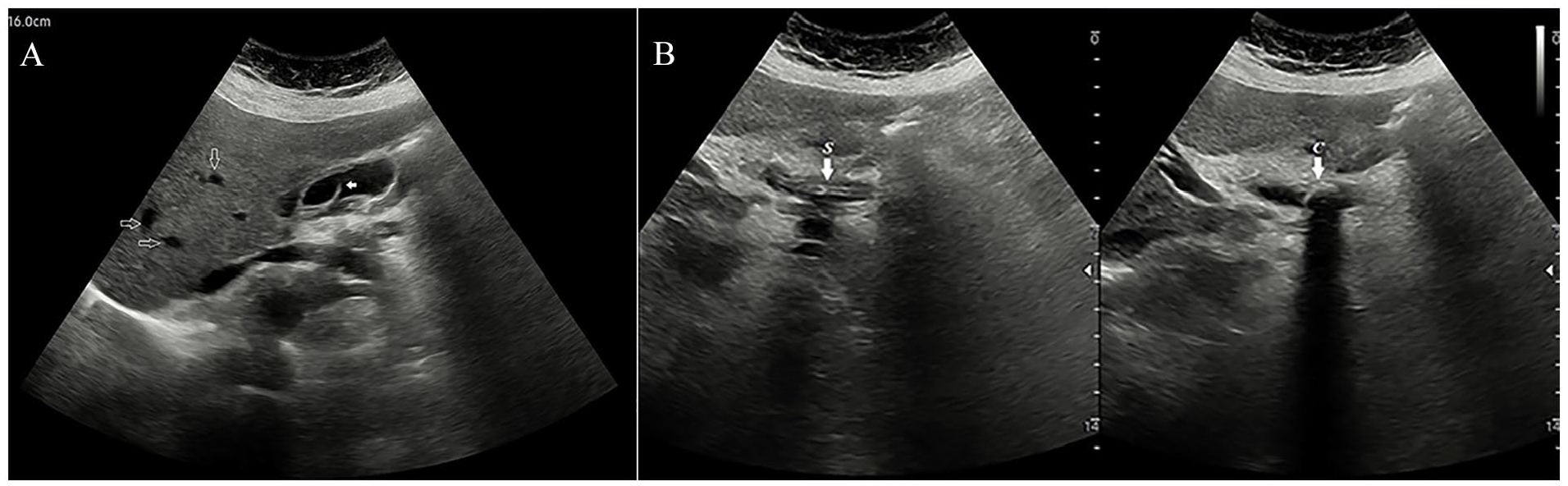
(A) The sagittal view of a grayscale sonogram demonstrates the proximal end of the biliary stent within the gallbladder lumen (see solid arrow); dilated intrahepatic biliary radicles are also noted (see open arrows). (B) The dual sagittal views of a grayscale sonogram shows the common bile duct with the double lumen stent inserted (denoted by the letter S) and an obstructive calculus (denoted by the letter C) within the duct (see arrows).
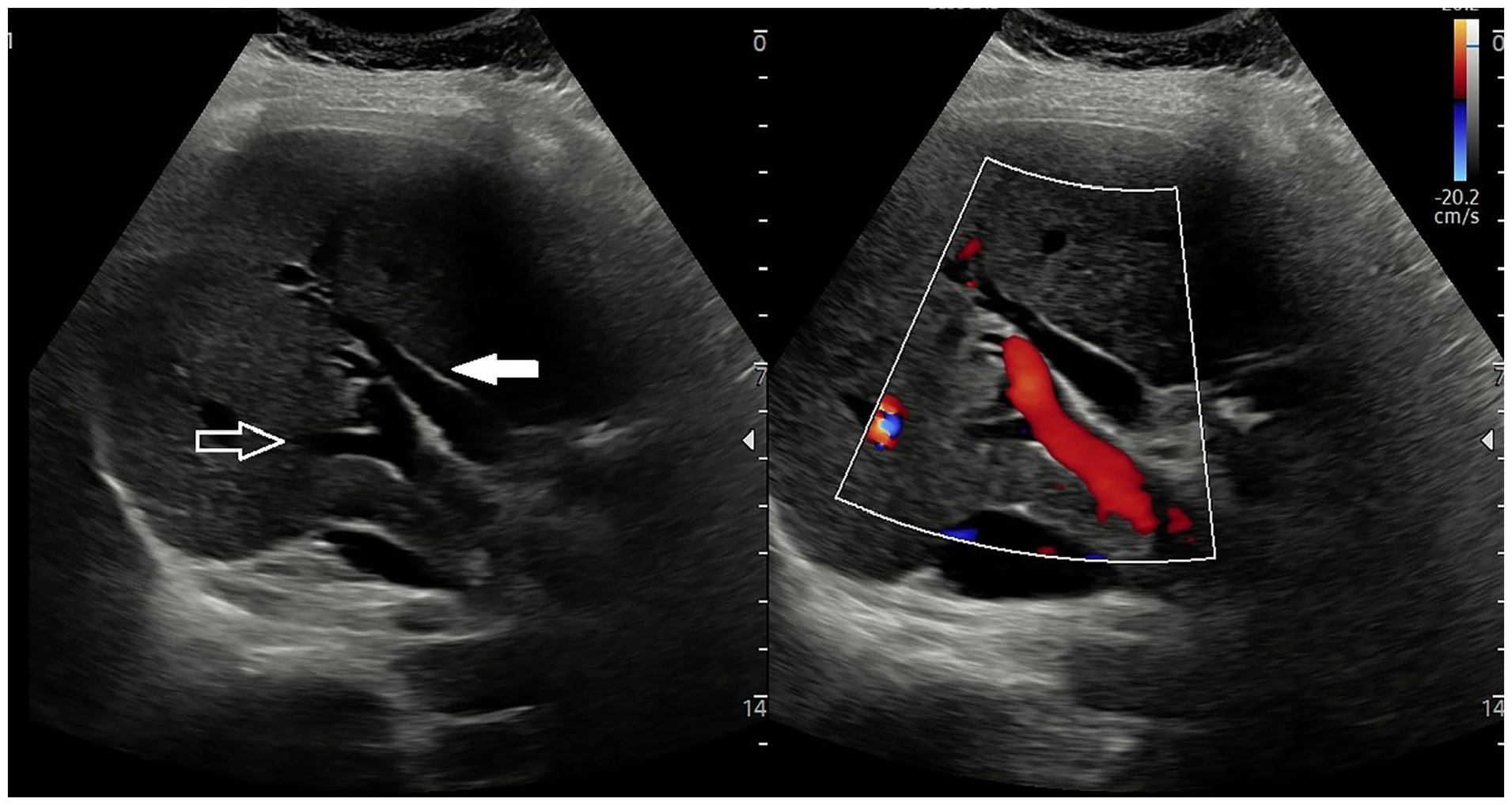
A dual transverse view of a grayscale sonogram, as well as an image with color Doppler applied. This set of images demonstrates the dilated common hepatic duct (see solid arrow) and main portal vein (see open arrow).
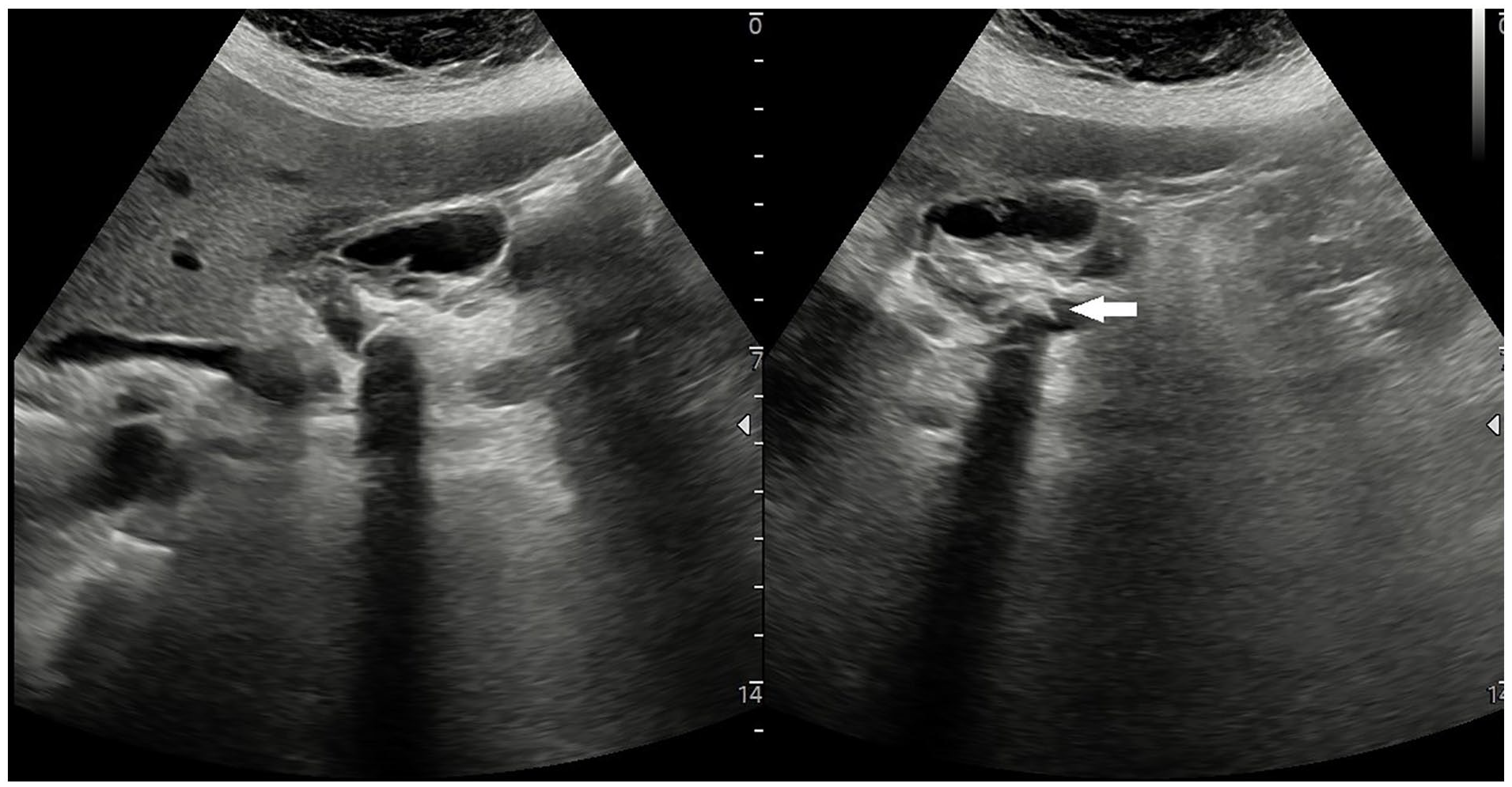
A dual transverse view of a grayscale sonogram that shows the biliary stent within the gallbladder lumen. It is also important to note that an echogenic calculus is lodged within the common bile duct (see white arrow).
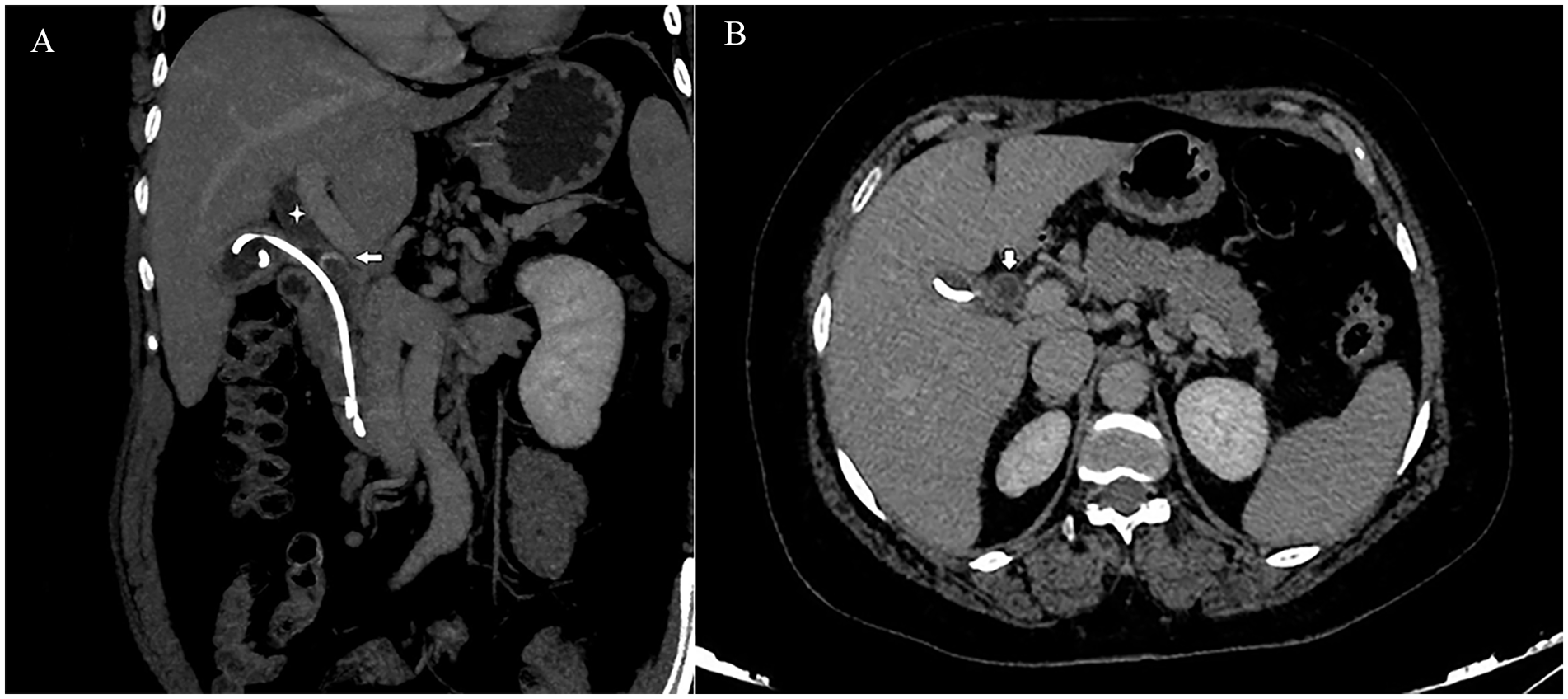
(A) A 2D reformatted abdominal computed tomogram provides a coronal view that shows the proximal end of the biliary stent, coiled up in gallbladder lumen. The common hepatic duct is also shown to be dilated (denoted by a star). In addition, a calculus is seen in the proximal portion of the common bile duct (see arrow). (B) A 2D reformatted abdominal computed tomogram provides an axial image, which demonstrates the stent in the gallbladder lumen. In addition, in this image, a dilated common hepatic duct is also noted (see arrow).
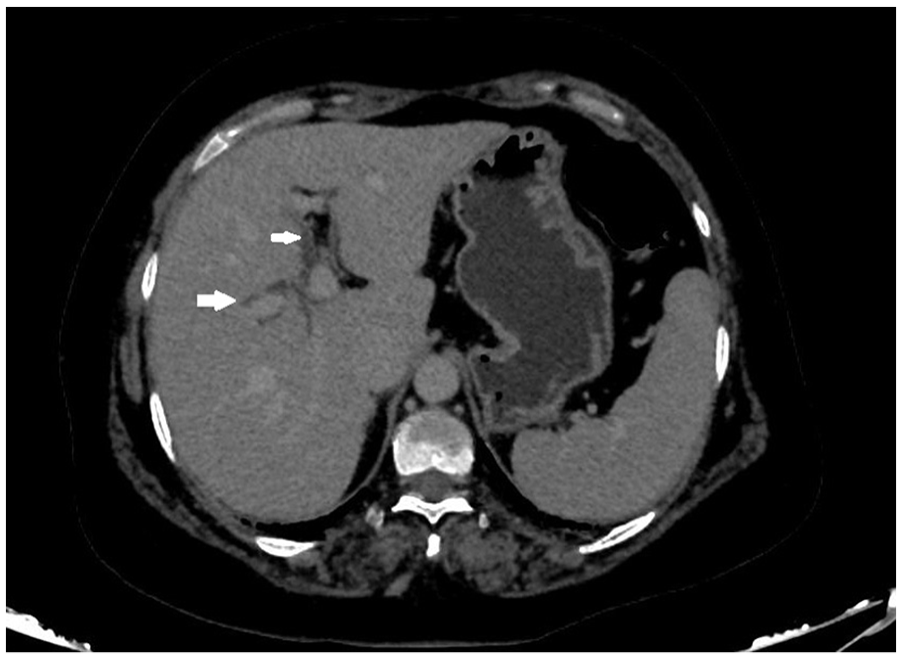
A 2D reformatted abdominal computed tomogram provides an axial view of the patient’s abdomen, which demonstrates dilated biliary radicles, within the liver.
Discussion
The use of endoscopic stenting is an established treatment option for biliary obstruction secondary to malignant or benign disease. Andersen et al. 2 suggested that, compared with surgery, endoprosthesis placement is associated with lower total mortality, lower major complications, and a reduced duration of total hospital stay, as well as being equally efficacious. However, use of biliary stents may be associated with complications in 8% to 10% of patient cases and includes cholangitis, cholecystitis, pancreatitis, duodenal injury, stent breakage, migration, or occlusion, which may lead to recurrent biliary obstruction.3 –5 Among these, the most commonly seen complication is cholangitis, 3 which may occur due to the stent clogging from an accumulation of biliary sludge and ingrowth of microbial biofilm.
Migration of biliary stents is an uncommon complication, which may be seen in 5% to 10% of patients who have undergone biliary stenting. 1 Arhan et al. 4 observed that the rate of migration for plastic stents, in patients undergoing endoscopic biliary stenting, was 8.58%. Migration of the stents can occur either proximally into the hepatic ducts or distally into the duodenum or the colon.3 –5 Risk factors for stent migration include a dilated common bile duct, wide sphincterotomy, and biliary balloon dilation.1 –3 Kawaguchi et al. 1 observed that the frequency of migration was significantly more in cases with a bile duct diameter more than 10 mm, compared with a diameter less than or equal to 10 mm.
Furthermore, migration of stents depends on a variety of conditions and the type of stent used, nature of disease, and duration of stent placement. As compared with pigtail stents, migration is more commonly seen in the case of straight stents, which is the reason that straight tube stents have been modified with side flaps or barbs, to reduce the risk of migration.1 –4 For these same reasons, most of the stents used now are double pigtailed with flaps at each end, to reduce the chances of migration.
Proximal stent migration is more commonly seen with shorter stents, while longer stents tend to migrate distally. This may be since it is less likely for the longer stents in the bile duct to migrate, due to a longer segment of the stent being fixed in the common bile duct, thus limiting proximal displacement. 3 Moreover, the placement of multiple stents and subsequent breaking or fracture of stents increases the risk of stent migration. A longer duration of stent placement also increases the risk of migration.
Compared with malignant disease processes, stent migration is more commonly associated with benign biliary disorders, which may possibly be since the degree of stenosis in malignant pathology is more than in benign disease.3 –5 Therefore, upon resolution of local inflammation, stents used in benign pathology will have more space to migrate, when compared with the tight covering of the stents within malignant tissues.
Proximal migration of a biliary stent was more commonly noted in cases of biliary stenosis due to benign pathology, stenosis in the distal common bile duct, bile duct diameter more than 10 mm, stent placement duration more than 1 month, and straight-type stents.1,5,6 Arhan et al. 4 reported that proximal stent migration occurs in cases with cholangiocarcinoma, short stents, or stents with large diameters. Most of the stents that migrate distally do not lead to any significant symptoms and are eliminated spontaneously; however, proximally migrated stents may lead to obstructive jaundice and cholangitis, necessitating retrieval or re-stenting. Stents that have migrated proximally can be successfully retrieved endoscopically by using a variety of grasping techniques involving baskets or balloons.4,5
In this case, one possibility for the stent to be lying in the GB lumen could be a misplaced stent due to cannulation of cystic duct during ERCP procedure. 7 It is also important to note that the MRCP revealed a low and medial insertion of cystic duct. Another less likely possibility could be migration of the stent post-ERCP, into the GB. Based on a limited review of the literature, there was only one other reported case of proximal migration of biliary stent in the GB lumen and, in that case, the stent was ligated, as well as the cystic duct, during cholecystectomy. 8
Conclusion
This case report highlights the need for the endoscopists to recheck and confirm the positioning of the stent after the ERCP procedure. In addition, the level of evidence may suggest the need for heightened awareness by surgeons and gastroenterologists regarding the possibility of presence of biliary stent in the GB lumen, especially in patients with a history of endoscopic biliary intervention(s).
Supplemental Material
sj-pdf-1-jdm-10.1177_87564793231189009 – Supplemental material for A Biliary Stent in the Gallbladder Lumen: Misplacement or Migration?
Supplemental material, sj-pdf-1-jdm-10.1177_87564793231189009 for A Biliary Stent in the Gallbladder Lumen: Misplacement or Migration? by Rohit Bhoil, Anupam Jhobta and Nidhi Rana in Journal of Diagnostic Medical Sonography
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This was a case report which in which the findings were analyzed retrospectively. The case study did not affect/alter the management in any way.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.