
Abstract
Objective:
The purpose of this study was to establish a noninvasive, safe, and reliable sonographic technique for evaluating peritonsillar abscess and subsequent drainage. Also, of paramount interest to the emergency physicians was to determine whether this imaging technique could assist in localization and drainage of a tonsillar abscess, minimizing the risk of patient complications.
Materials and Methods:
This was a prospective nonrandomized study, conducted in a small urban community hospital. All sonographic examinations were performed by the staff sonographers. Imaging procedures were performed using a GE Logiq 9 or E9 ultrasound equipment system (GE Medical, Waukesha, Wisconsin). A broad-band curved linear array transducer (9L) was used to visualize the affected tonsil through a submandibular approach. An endocavity transducer (5 to 9 MHz) was used for all trans-oral cavity imaging. All aspirations were performed with an 18-G 20-cm Trocar needle (Cook Medical LLC. Bloomington, IN) inserted through a commercially available needle guide attachment (CIVCO Medical Solutions. Kalona, IA).
Results:
A total of 91 patients (N = 50 males and N = 41 females) are included in this cohort study. The patients ranged in age from 10 to 80 years of age and the average age was 34 years. In this patient cohort, 87 abscesses were found, and five patients had bilateral peritonsillar abscess. Of the remaining patients, one had inflammatory lymph nodes and four inflamed tonsils without abscess. All abscesses were successfully drained without complications.
Conclusion:
This level of evidence demonstrates a possible method is safer, which may be more effective than a nonimaging approach for needle aspiration. This technique is easily applied by both physician and sonographer with minimal training.
Peritonsillar abscess (PTA) aspiration is a common emergency medicine procedure. Traditionally, it has been performed without imaging guidance, which could lead to multiple complications, such as multiple needle redirections, negative aspirations, and occasional bleeding complications, based on the location of the internal carotid artery (ICA). Any complication involving the ICA should be avoided because an otolaryngologist is not readily available at many institutions, should a practitioner fail to aspirate pus properly. There appears to be a need to underscore the use of sonography as a powerful yet safe diagnostic tool for evaluating the tonsils. Moreover, it may have an important diagnostic role in the drainage of any abscess, compared to a nonimaging approach to the insertion of a needle.
There are very few reports in the literature describing the use of diagnostic imaging to evaluate the tonsils. Blaivas et al. described a small study of six patient cases of intraoral tonsillar imaging with drainage. However, in that study, the needle was inserted without the aid of a needle guide 1 Todsen et al. described one patient case in which a needle guide was used with sonographic guidance; however, he used a specialized transducer which is not widely available, at most medical facilities. Most publications describe transcutaneous imaging of the tonsils. 2 Therefore, a gap appears to be present in the literature on this particular clinical application for sonography.
The design of this clinical-based study was planned in 2010. The research question was, could sonography aid in the diagnostic imaging of the tonsils and drainage of any abscess that may be present. The emergency physicians were looking for a safer technique than a blind insertion of a needle into the area of the infection. They also wished to reduce the risk of accidentally perforating the ICA located just deep to the tonsil. The intent was to stage a clinical data collection that would report on the largest sample size related to tonsil’s imaging and sonographic guided drainage.
Materials and Methods
Study Protocol
The frame for this clinical study was to enroll all the patients, within the host institution, with a suspected PTA. The recruitment of patients was based on information obtained from the review of the retrospective review of medical charts and associated medical imaging studies. Also included were patients having a suspected PTA on physical examination.
To comply with medical center guidelines and the Health Insurance Portability and Accountability Act (HIPPA), institutional approval was obtained from the institution and the graduate medical education program. To assure anonymity, all patient information was removed from any of the data procured from patient’s imaging records, as well as from their medical record review. A case study number was then assigned to each patient eliminating all patient information from the compiled study data.
The imaging studies that were reviewed included computed tomography (CT), sonography, or both. This cohort study was limited to patients who were recruited from the emergency medicine department. Some of the patient symptoms that were used for inclusion criteria included one or more of the following symptoms: difficulty swallowing, trismus, drooling, and a “hot potato voice.” When a suspected PTA was noted with one imaging technique, the patient’s medical records were searched for any previous diagnostic studies that pertained to this condition.
Equipment
All sonographic examinations were performed by the staff sonographers. Imaging procedures were performed using a GE Logiq 9 or E9 ultrasound equipment system (GE Medical, Waukesha, Wisconsin). A broad-band curved linear array transducer (9L) was used to visualize the affected tonsil through a submandibular approach. An endocavity transducer (5 to 9 MHz) was used for all trans-oral cavity imaging. All aspirations were performed with an 18-G 20-cm Trocar needle (Cook Medical LLC. Bloomington, IN. DTN-18-20.0-U G02901) inserted through a commercially available needle guide attachment (CIVCO Medical Solutions. Kalona, IA.742-270). An extension set (B. Braum Medical Inc. Melsungen, Germany. US1320) with small syringe is attached and connected to the needle once the trocar is removed, which allows for flexibility, while aspirating the fluid. This procedural set-up allows for an easier aspiration of the localized abscess (Figure 1).

An example of the endocavitary guide with needle inserted, the extension tube, and syringe attached and ready for aspiration.
Results
The medical records were retrospectively reviewed for patients who consented to the study between March 2010 to November 2022 and treated in the emergency medicine department, with a suspected tonsillar abscess (TA). This resulted in a total of 91 patients consented to the study (N = 50 males and N = 41 females). Difficulty swallowing has been described as a common symptom for TAs. In this study cohort, however, only 63 participants presented with this symptom, based on the medical record search. Forty-eight participants presented with difficulty swallowing while another 15 experienced a sore throat. Patient’s duration of symptoms ranged from 1 to 14 days with an average duration of 5.8 days before seeking medical care. One patient reported symptoms lasting 90 days while most symptoms ranged from 1 to 7 days prior to seeking medical care.
The patients ranged in age from 10 to 80 years of age with the average being 34 years of age. Of the 91 patients, 34 right and 52 left tonsils were evaluated for an abscess. In addition, six patients were evaluated for bilateral TAs, which represented 6.5% of the patients in this study.
Sixty-one patients required abscess drainage under ultrasound guidance. Of these patients, the fluid volume drained ranged from 1 to 10 cc. Acute tonsilitis (N = 9) and lymphadenitis (N = 9) were reported in 18 patients. Four of the patients evaluated required no intervention as the exam revealed normal tissue.
Two patients with suspected TA were not drained in this cohort. The first did not use sonography guidance, but instead used the blind needle insertion approach. In the second patient case, sonography was unable to adequately assess it. The CT images demonstrated a very deep oropharynx abscess requiring surgical intervention.
In the early phases of the study, a CT of the neck was performed for all patients to confirm the presence of an abscess prior to sonography. As the study progressed and the confidence of the emergency medicine physicians grew, only a transoral sonogram was performed, to evaluate for TA. Of the 91 patients with a PTA, only 54 were imaged solely with sonography.
All patients were discharged from the emergency medicine department with a recommendation to consult their primary medicine physician for surveillance.
Procedure: Transducer Selection and Placement
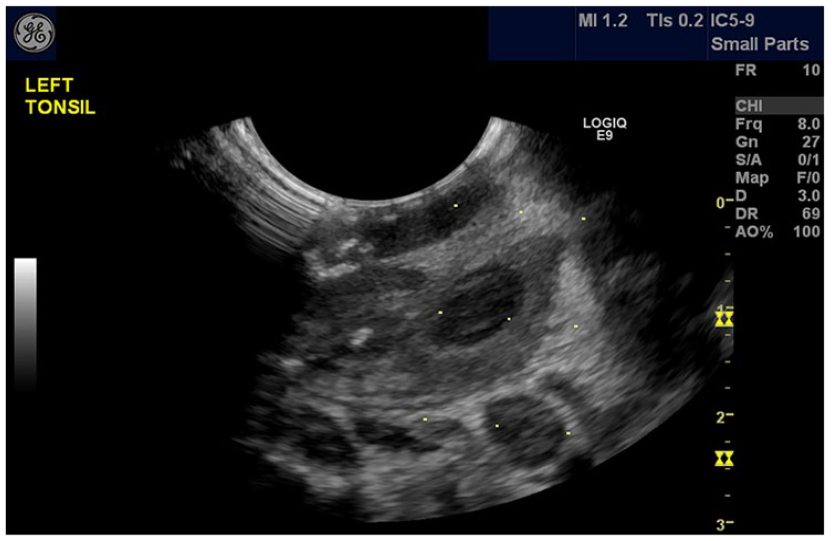
Only one patient was imaged, early in this study, using the submandibular approach. The initial thought was it might be easier on the patient during the initial evaluation. This was quickly changed to intraoral as it provided superior visualization of the tonsils (Figure 2). The remainder of the patients in this study were all evaluated transorally, with the endocavity probe IC 5-9D. During the initial evaluation, all patients were imaged without the needle guide attachment, to confirm the presence of an abscess. Buckey et al. described the use of a thin coat of sterile acoustic gel on transducer for a direct intraoral sonogram. 3 However, in this study, sterile acoustic gel was not required as the moist oropharynx was an adequate conductive surface. All patients were imaged in a semierect position.
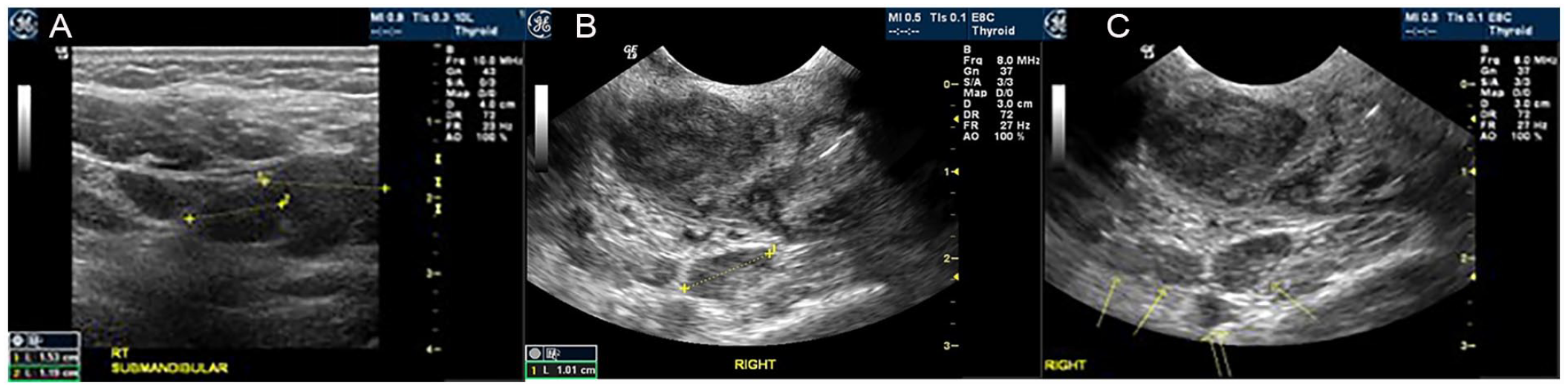
(A) The sonogram provided was accomplished using the submandibular approach and attempting to visualize a suspected tonsillar abscess (Note: The hypoechoic enlarged lymph node seen). (B) The additional sonogram was the result of an initial transoral visualization of the right tonsillar area. (C) The transoral sonographic image demonstrated a right tonsillar abscess and enlarged lymph nodes. See the solid yellow arrows (Note: The open yellow arrow indicates the adjacent area of the internal carotid artery.
Anesthesia
Throughout this study, various techniques for patient anesthesia were used. All patients received one or more of the following techniques.
First Anesthesia Technique
During the initial phase of this study, physicians preferred to infiltrate varying amounts of 1% lidocaine to the posterior pharynx, directly over the area to be aspirated. This technique required the physician to directly visualize the tonsil. This could be very difficult for the patient with severe trismus. A light source was focused into the oral cavity, and tongue blade was used to depress the tongue allowing the tonsil to be seen. At this point an uncapped needle is inserted trans-orally and into the tonsil, in the region of the suspected abscess. This technique was rather risky as any patient motion could result in tissue laceration or perforation of unintended regions. To minimize this risk, some physicians used a technique where they would remove the cap from a shorter needle and place the longer needle through it perforating the end of the cap. This resulted in only a small portion of the needle being exposed inside the mouth (Figure 3). This greatly decreased the patients’ risk of having the needle inserted deeply and risking ICA perforation. It also allowed the physician to properly anesthetize the region.
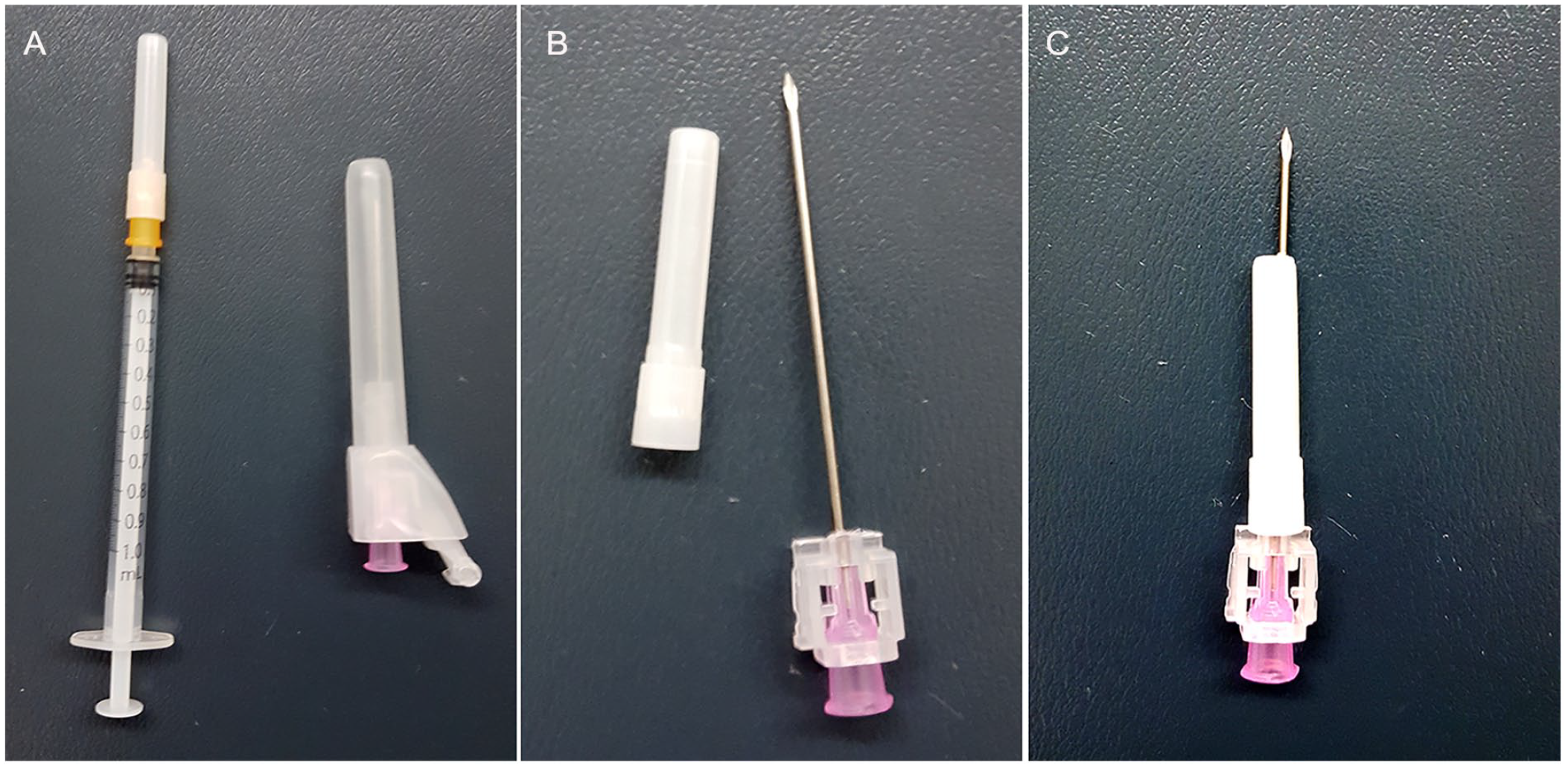
(A) Images of a short length needle/syringe and longer 18 gage needle. (B) An image of the cap removed from the short needle and adjacent to uncapped longer needle. (C) An image of the longer needle inserted through short needle cap which was used to anesthetize the region of interest.
Second Anesthesia Technique
Another technique was to have the patient gargle with viscous xylocaine. This technique had some success. However, it relied on the cooperation of each patient. A modification of this technique was used by atomizing 1 or 2% xylocaine (figure 4). This was accomplished by placing it within the device respiratory therapists used to give patients breathing treatments.

An image of how the xylocaine is placed within the clear cup. The flow volume must be high (above 10 L/m) to assure proper atomization of the xylocaine.
Topical anesthesia is performed with nebulizer 2% lidocaine and or 2% viscous lidocaine soaked gauzed wrapped around a curved clamp from the suture kit and held to the ipsilateral mucosa for a few minutes, while getting equipment ready. Light sedation with an opiate or benzodiazepine can be used. This is followed by submucosal injection of lidocaine for additional anesthesia.
While this technique was more successful than gargling alone, some patients were not fully anesthetized. This required the physician to directly inject the anesthesia into the area of interest prior to inserting the Trocar needle.
Third Anesthesia Technique
A topical anesthetic (14% benzocaine, 2% butamben, 2% tetracaine) was sprayed directly into the posterior pharynx (Figure 5). This technique has been highly successful with reducing patients’ discomfort. Using this spray allowed the affected area to be completely anesthetized. The use of this spray has also minimized the effect of trismus and allowed the patient to open their mouth with less discomfort. While this technique was most effective, the topical spray became unavailable at the host facility.

An example of one of the topical spray anesthetics.
Needle Guiding the Drainage
On the saved static sonogram, electronic calipers were used to measure the distance from the side of the image, where the needle would pass and the surface of the suspected abscess. This minimizes the risk of advancing the needle deeper than necessary (Figure 6).
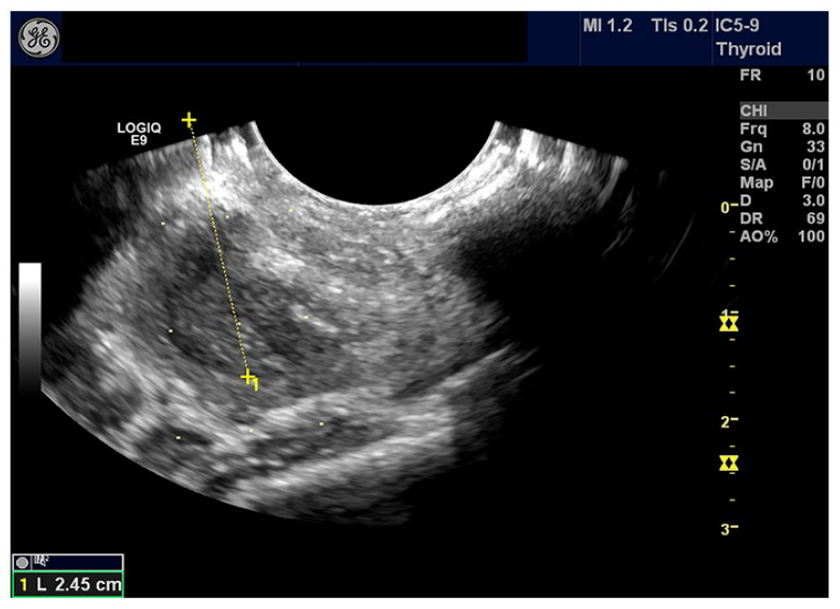
A sagittal sonogram that was used to allow for electronic calipers to trace the anticipated trajectory of the aspiration needle and provide minimal distance to the suspected abscess.
It is at this point in the procedure, that the needle is placed through the needle guide and advanced until the tip of the needle is the same measured distance, past the lateral portion of the gray rubber active part of the transducer (Figure 7). Then measure the distance from the distal portion of the hub of the needle to the beginning of the needle guide to obtain the measurement of the plastic bumper that will prevent excess advancement of the trocar. Remove the trocar, cut a piece of the plastic cover, and slide the piece of tubular cover over the trocar prior to reinserting it through the needle guide.
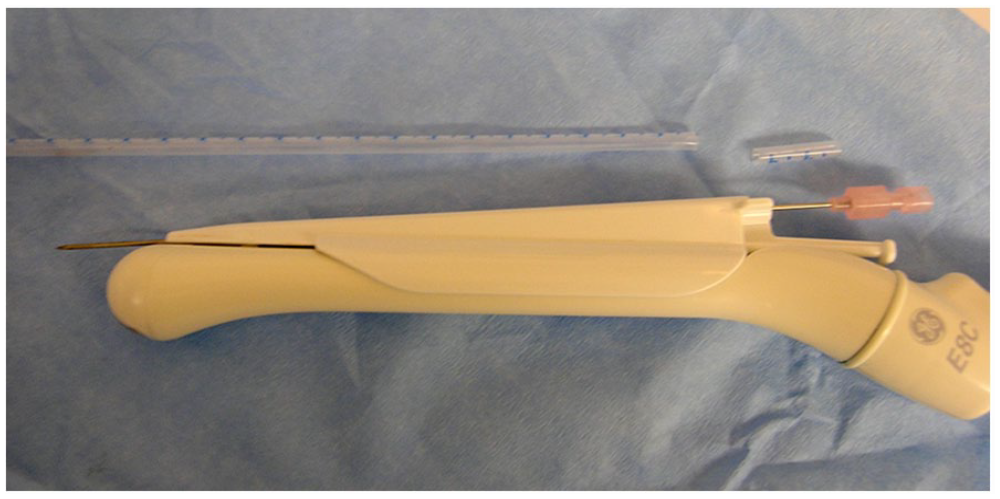
An image of the transducer with needle inserted into guide attachment. In addition, the needle at tip of transducer is inserted to the measured depth for aspiration.
Next, it was necessary to localize the abscess and determine whether to have the needle on the medial or lateral side of the transducer. Since the needle guide protrudes from the transducer, it was necessary to put it in the patient’s mouth and place the device either at the 3 o’clock or 9 o’clock position. In this study, the best results came by directing the needle from the medial aspect of the tonsil toward the abscess without targeting the ICA, located just deep to the tonsil. This approach avoided inserting the needle through the palatine arch, since this tissue is more difficult to penetrate. The ICA is easily visualized in this view with color Doppler (Figure 8).
A transoral sonographic image is provided of a left tonsillar abscess, with the needle path guidelines activated.
During this study, it was noted that trismus very rarely prevented entry of the transducer, when it was attempted after topicalization and light sedation. Imaging is performed with the ultrasound equipment system’s “biopsy guide” mode being activated. This electronic overlay projects guidance lines onto the ultrasound equipment’s monitor. The goal is to have the aspiration needle follow the middle-projected line, on the monitor. When inserting the needle, this centerline needs to be aligned within the abscess and, if possible, excluding the ICA.
The sonographer localized the abscess and aligned it with the center biopsy guideline (Figure 8). With the sonographer holding the transducer, the physician then advanced the trocar, as they observed the screen (Figure 9).
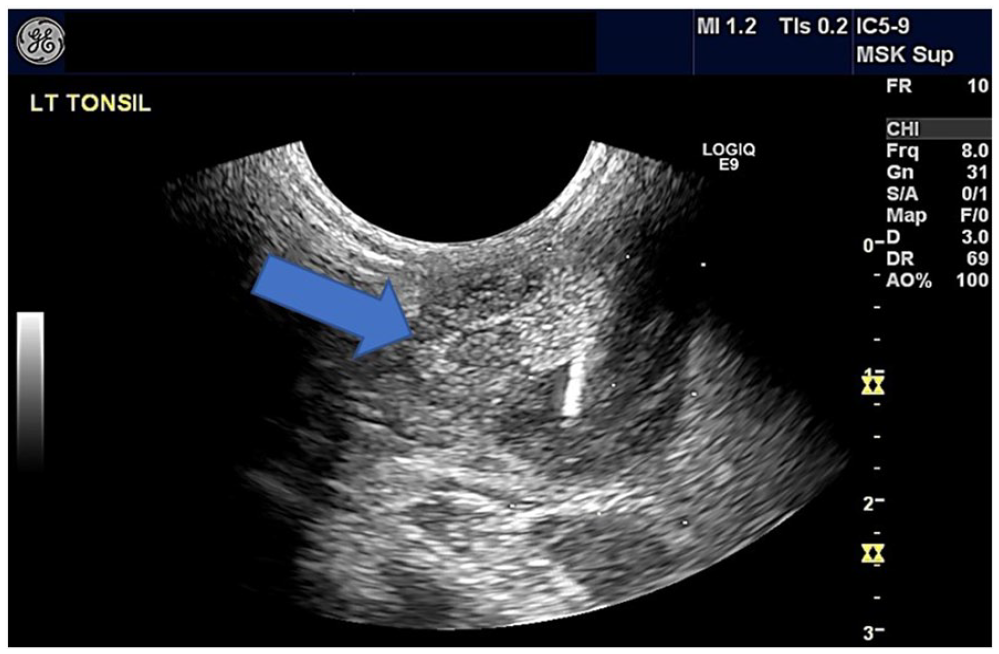
The sonogram provided demonstrates (Note blue arrow) how the echogenic needle tip is adjacent to the projected center needle guide indicators.
Once in the abscess cavity, the needle trocar was removed, and a short extension tubing was attached to a syringe for the purpose of aspiration. During aspiration of the abscess the trocar may be freely moved within the cavity until there is no abscess material remaining. The trocar was then retracted, and the transducer was removed from the patient’s mouth.
Discussion
This pathology was first described in medieval England as “quinsy,” and it was used to describe any infection of the throat. It was not until the early 19th century that quinsy slowly evolved to PTA. 1 Peritonsillar infections have been occurring for hundreds of years with the first reported incision and drainage of a PTA dating as far back as 1362, by a French surgeon, Guy de Chauliac. The first peritonsullar abscess tonsillectomy was thought to have been performed by Chassaignac, in 1859.
Anatomy and Embryologic Development
During the embryonic stage, the tonsils arise from the second pharyngeal pouch as buds of endodermal cells. Shortly after birth, the tonsils grow irregularly until they reach their ultimate size and shape, depending on the amount of lymphoid tissue present. 4
The palatine tonsils and their surrounding tissues are depicted in Figure 10. The two tonsillar pillars/arches define the tonsils anteriorly and posteriorly borders. The glossopalatine and the pharyngopalatine muscles are the major muscles of the anterior and posterior pillars, respectively. The tonsil lays in the depression between the palatoglossal and the palatopharyngeal arches. 5 It is the muscles of the anterior pillars that the needle should be directed in a medial to lateral approach. These muscles can be difficult to penetrate. The tonsils are surrounded by a capsule, which attaches their deep surface to the fascia overlying the musculature of the pharynx. 6 Several branches of the external carotid artery supply blood to the tonsils. Lymphatic drainage occurs by both the jugular and deep cervical lymph node chains. It is due to these chains that tonsil infections can lead to cervical adenitis. 7
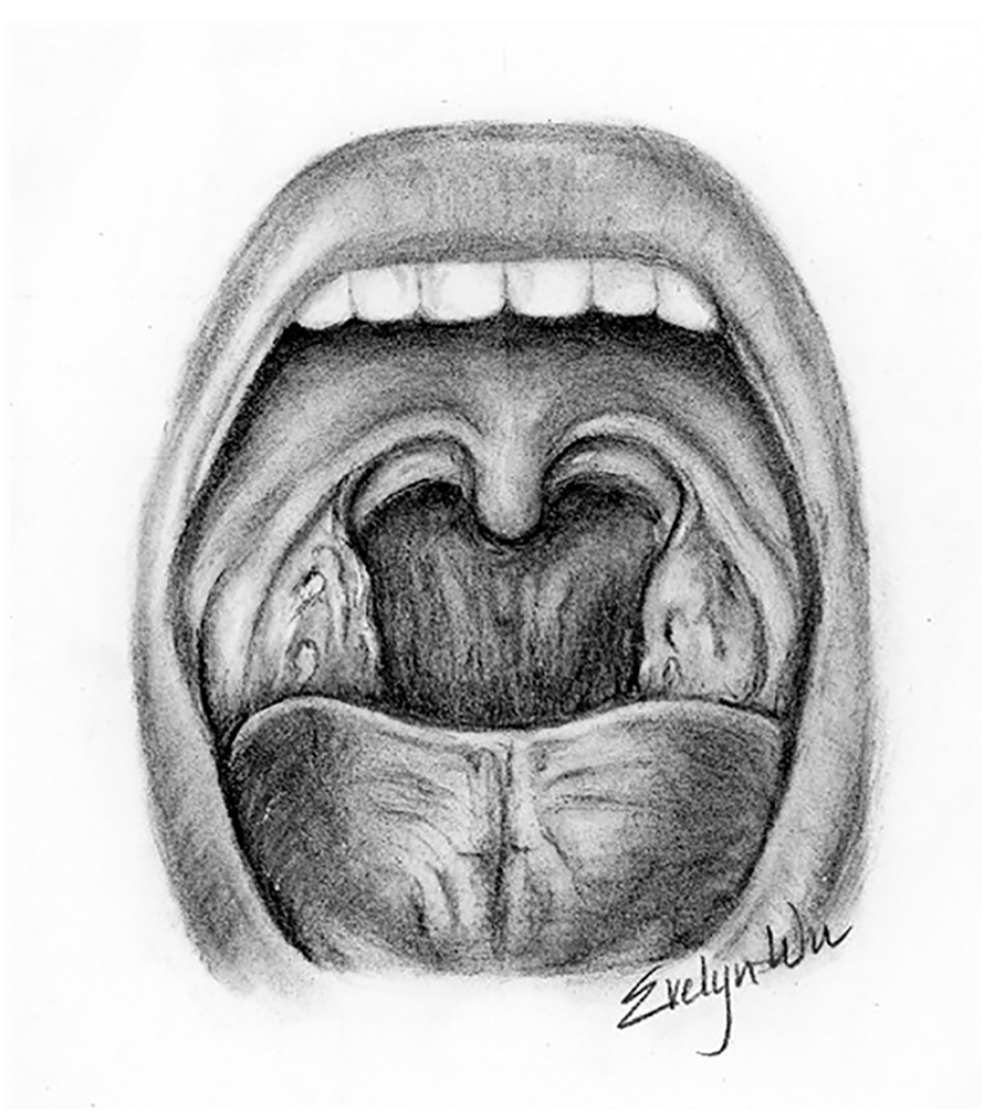
An anatomical illustration of the human mouth, palatine tonsils, and the surrounding tissues.
Etiology
Peritonsillar abscess is the endpoint of disease progression. It starts with acute exudative tonsillitis moving to cellulitis and finally abscess formation.7,8 In this study, cellulitis was seen in multiple patients. These patients were treated with oral antibiotics and returned in 1 to 2 days with formation of an abscess.
The Weber’s glands are suspected of playing a role in the formation of PTA.8,9 This group of mucous salivary glands are located superior to the tonsil in the soft palate and are connected to the surface of the tonsil by a duct. 9 Their function is to clear debris from the tonsils and aid in digestion of food particles, within the tonsillar crypts. If their ducts are obstructed inflammation and cellulitis can develop.
Lehnerdt et al 9 described that smoking has an increased factor for PTA. Another author included significant periodontal disease as well. 8 In this study, 78 of the 91 patients provided information about smoking. In this study, 40 of the 78 patients were active smokers.
Physical Exam
When the patient first presents to the emergency medicine physician, they will perform a intraoral inspection to rule out an infection of the salivary glands, teeth, and mastoid bone, as well as neoplasms, cervical adenitis, and aneurysm of the ICA. A thorough history and physical examination often suggests a diagnosis of PTA. However, imaging is performed to differentiate PTA from other diagnoses. At the host facility, a CT of the neck was the chosen imaging technique. However, sonography conducted by a skilled and experienced sonographer proved to be a useful diagnostic tool. Boesen described the use of transcutaneous sonography by placing the transducer over the submandibular gland and examining the entire tonsillar area. 10 The transcutaneous approach was performed in only one patient in this study, as the transoral approach demonstrated superior visualization and was well tolerated by these patients. The presence of trismus was not a limiting factor in this study.
Clinical Manifestations
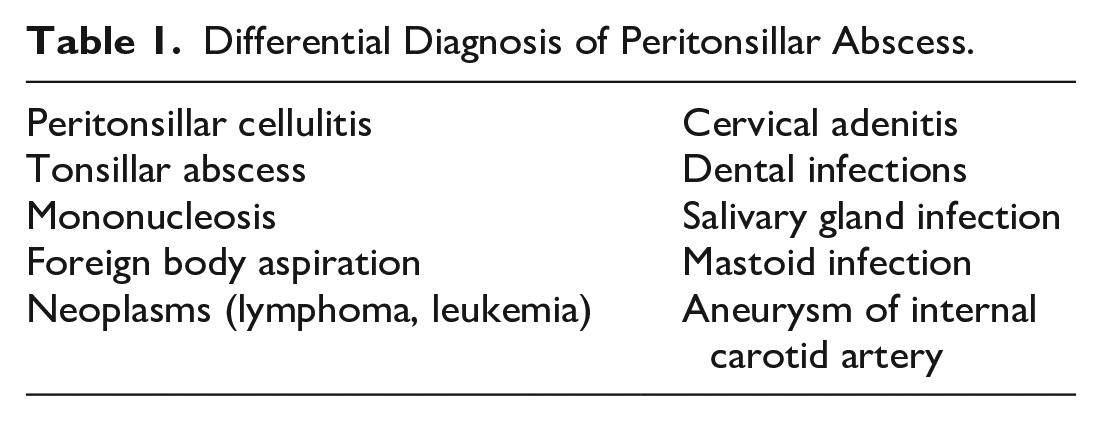
Early in the disease, peritonsillar cellulitis may represent a transitional stage in the development of PTA. 11 In this study, only one patient presented with peritonsillar cellulitis. See Table 1 for a complete list of the differential diagnoses.
Differential Diagnosis of Peritonsillar Abscess.
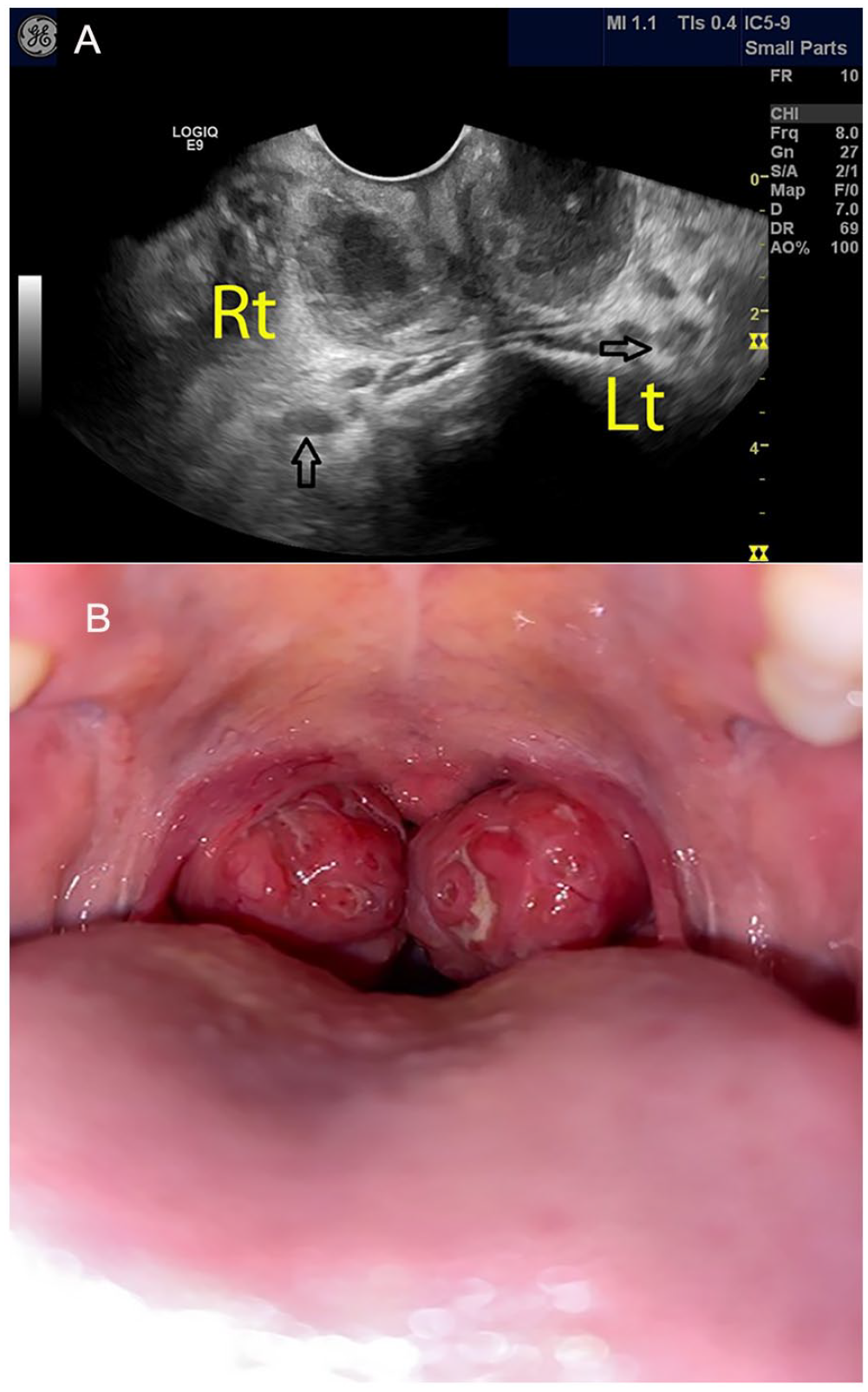
Patients with PTA may present with fever, malaise, sore throat, dysphagia, or otalgia. In more advanced stages, patients may speak in a muffled voice (also called “hot potato voice”). 12 In this study, only a few with advanced PTA presented with the “hot potato voice.” Swallowing can be difficult for these patients as it can be highly painful. This can result in pooling of saliva or drooling 12 (Table 2). In this study, 68 of the 91 patients had documented information on their ability to swallow. Of those, 48 had difficulty with swallowing, while 15 had no symptoms. Of the 48 patients’ symptoms ranged from slight dysphagia to severe drooling, with a muffled voice.
Common Symptoms and Physical Findings in Patients With Peritonsillar Abscess.
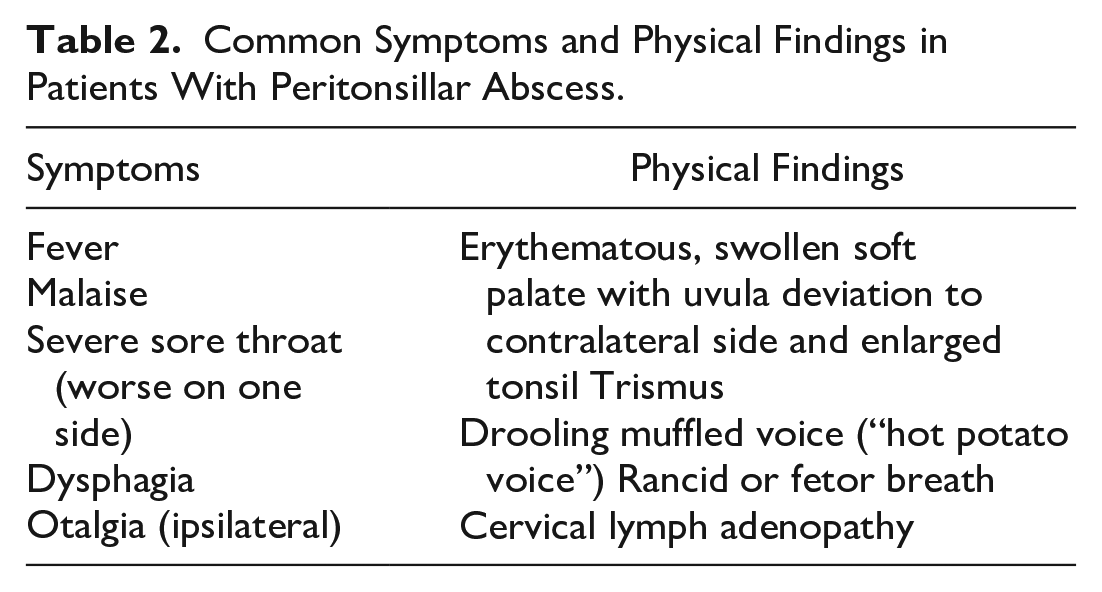
Traditionally, the presence of a unilateral swollen tonsil with contralateral deviation of the uvula, in addition to drooling, trismus, and dysphagia, was suggestive of a diagnosis of PTA. 13 However, in the presence of a bilateral PTA, the uvula is not deviated (Figure 11).
(A) A sonogram is provided that demonstrates a bilateral tonsil abscess and captured with a transoral approach. The open black arrows demonstrate the position of the internal carotid arteries. (B) The photograph shows the centrally located uvula along with the large bilateral tonsils and small airway.
Current Technology
As new equipment became available during this study, improved image quality and resolution was obtained, due to the availability of high-frequency transducers. Improvements in image quality have been observed using tissue harmonics, speckle reduction, and crossbeam imaging. Along with higher frequency, the improved color Doppler and power Doppler capabilities were helpful in evaluating the vascularity of these lesions as well as the location of the ICA. All these options provided an improvement over normal imaging parameters, and on most occasions, improved the image resolution.
Limitations
The major limitation to this study was the pre-experimental design which has threats to internal and external validity. As a cohort study, this clinical work demonstrates how higher-level evidence can be generated. Trismus can be a limitation of this diagnostic technique, which could not preclude the standard aspiration technique. The only case that this precluded aspiration was in one of two bilateral PTA. In the first, a patient had significant trismus and required the operating room for drainage. In the second incidence, the physician was able to drain each side under sonographic guidance and discharge the patient. The patient had significant improvement on her follow-up visit. There are many patients who cannot open their mouths wide enough to insert the transducer at first, but after topical lidocaine and light sedation, almost everyone can be imaged and drained.
Special equipment may need to be ordered or located. Most radiology departments should have an intracavitary transducer and needle guide for biopsies, and they may have the blunt-ended trocar. If not, these are inexpensive and readily available items to order. The most efficient way to perform this is to have the sonographer bring these with the ultrasound equipment system to the emergency medicine department and assist with the procedure.
As with any procedure involving sonography, there is a small learning curve regarding identifying the anatomy. It does take some experience to become familiar with regional anatomy. Compared to other sonography guided procedures, it is technically easy to image as it is a superficial structure and the quality is not significantly altered by obesity.
Conclusion
In emergency medicine, there is some reluctance to drain a PTA, since it was performed without guidance and can have serious complications, such as puncturing of the carotid arteries, jugular veins, or parotid gland. 14 However, performing PTA drainage under direct guided visualization has been demonstrated to be a safe and effective alternative to blind aspiration. This procedure was well tolerated by both young and older patients, in this cohort. The results of this cohort study would suggest that for those small hospitals, where otolaryngologists are not available, this may be a potential diagnostic/therapeutic procedure and a less-risky alternative to nonimaging directed aspiration.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from Graduate Medical Education Program.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
Not applicable.