
Abstract
Aims:
Bacteremia during elective tonsillectomy is well recognized, whereas bacteremia during quinsy tonsillectomy has never been studied. The aim of the present study was to explore the incidence of bacteremia during elective and quinsy tonsillectomy in order to evaluate the antibiotic prophylaxis recommendations to patients at high risk of infective endocarditis who are undergoing tonsillectomy.
Methods:
A prospective study was conducted on 80 patients undergoing elective tonsillectomy and 36 patients undergoing acute tonsillectomy due to peritonsillar abscess. Blood cultures, tonsillar swabs, core tissue, and pus aspirates were analyzed by standard microbiological techniques.
Results:
Bacteremia was detected in 73% of patients during elective tonsillectomy compared to 56% during quinsy tonsillectomy (P = .089, Fishers exact test). Significantly more blood culture bottles were positive for each isolate obtained from elective tonsillectomy cases compared to quinsy tonsillectomy cases (P < .001, Spearman rank correlation). In all, 59% and 42% of electively and acutely tonsillectomized patients, respectively, had bacteremia with microorganisms that are predominant in bacterial endocarditis. Ninety-three percent of the isolated strains were sensitive to amoxicillin, and all were sensitive to amoxicillin with clavulanic acid.
Discussion:
Our results challenge the distinction made by the European Society of Cardiology between elective and quinsy tonsillectomy, with regard to antibiotic prophylaxis recommendation only to patients undergoing procedures to treat an established infection. To provide full empiric coverage, including coverage for Staphylococcus aureus, we advocate the use of amoxicillin with clavulanic acid in patients at high risk of infective endocarditis.
Introduction
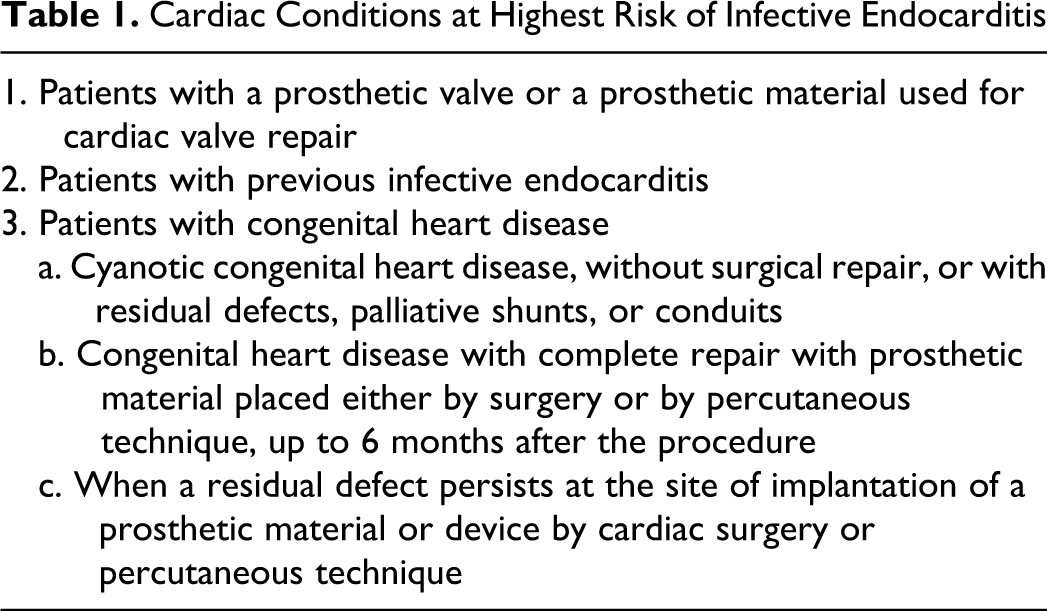
Bacteremia during elective tonsillectomy is well recognized.1–10 In healthy participants, bacteremia usually ceases within 20 to 40 minutes. 10 ,11 and is not of concern with regard to endocarditis. Thus, routine antibiotic prophylaxis is not recommended. 12 However, for patients at high risk of infective endocarditis (Table 1), who are undergoing a procedure at high risk of resulting in bacteremia, antibiotic prophylaxis is recommended. 13 ,14 According to the guidelines from the American Heart Association (AHA), tonsillectomy is a procedure at high risk of resulting in bacteremia, whether performed electively or acutely due to peritonsillar abscess (PTA), 13 and their current recommendation is amoxicillin 2 g orally 30 to 60 minutes before undergoing tonsillectomy for high-risk adult patients. In cases where infection with Staphylococcus aureus is suspected, an anti-staphylococcal penicillin or cephalosporin is recommended. Similarly, the European Society of Cardiology advises antibiotic prophylaxis for high-risk patients, who undergo invasive procedures. 14 However, in contrast to AHA, prophylaxis is recommended only when the patient is undergoing the procedure to treat an established infection (ie, drainage of abscess). An anti-staphylococcal penicillin or cephalosporin is then recommended. In Denmark, penicillin G is generally given during surgery to all patients undergoing acute tonsillectomy due to PTA, on the assumption that operating in an area with high bacterial load increases the risk of significant bacteremia and the risk of spread to other sites. The same assumption must be the basis for the distinction between elective and abscess tonsillectomy made by the European Society of Cardiology in recommending prophylaxis only in the latter cases. However, no studies have been previously conducted to determine the extent of bacteremia during quinsy tonsillectomy (acute tonsillectomy due to peritonsillar abscess).
Cardiac Conditions at Highest Risk of Infective Endocarditis
The aim of this study was to determine the incidence of bacteremia during elective versus quinsy tonsillectomy in order to evaluate the current prophylaxis recommendations to patients at highest risk of infective endocarditis.
Methods and Materials
Patients
This prospective study was performed between November 2005 and February 2009 at 3 Danish ear, nose, and throat (ENT) departments. The study consisted of 2 patient groups (1) 36 patients with PTA undergoing acute bilateral tonsillectomy and (2) 80 patients admitted for elective tonsillectomy. Group 2 patients were categorized into 4 subgroups according to indication for tonsillectomy (a) recurrent acute tonsillitis (RT; more than 5 episodes within 2 years), (b) tonsillar hypertrophy (TH) with the history of airway obstruction, (c) both RT and TH, and (d) halitosis or persistant sore throat syndrome (PSTS) without signs or symptoms of infection at any time.
Only patients aged 8 to 30 years, without antibiotic treatment during the month preceding surgery (including the time up to and during hospitalization) and without cardiac conditions necessitating antibiotic prophylaxis, were included in the study. Patients were examined and asked about complications in our outpatient clinic 2 to 4 weeks postoperatively.
Specimen Collection
After anesthetizing the patients, surface swabs from each of the tonsils were obtained and placed in transport media (Stuart medium; SSI Diagnostic, Hilleröd, Denmark). In PTA patients, the abscess was punctured and pus was aspirated into a sterile syringe. The tonsils were removed by blunt dissection and placed in sterile containers separately.
Within 2 minutes of removal of the first tonsil (in PTA patients the tonsil at the side of the abscess was removed before the contralateral side tonsil), blood samples (2 × 10 mL for aerobic growth and 2 × 10 mL for anaerobic growth) were taken from a peripheral vein in accordance with the techniques of sterile blood collection. None of the patients received antibiotics before the collection of specimens had been completed.
Microbiological Analysis of the Blood Cultures
In the laboratory, blood culture bottles were processed in the BacT/Alert (BioMerieux, Herlev, Denmark) with a 6-day incubation protocol. A Gram stain was performed on each positive blood culture. The positive blood cultures in the aerobic media were subcultured on 5% blood agar and chocolate agar in an atmosphere of 5% carbon dioxide (CO2) and on MacConkey agar under aerobic conditions. The same protocol was used for positive blood cultures in anaerobic media, with subculture on anaerobic agar plates and incubation in an anaerobic atmosphere. All media were obtained through SSI Diagnostic.
Propionibacteria and coagulase-negative staphylococci isolated from blood cultures, but not detected in tonsillar core or surface cultures, were considered cutaneous contamination and disregarded in the text and tables.
Microbiological Analysis of Tissue, Aspirates, and Swabs
Microbiological analysis was carried out at the Department of Clinical Microbiology at Aarhus University Hospital. Samples were stored at −80°C until bacteriologic investigations were performed. Specimens were processed in a class-2 laminar airflow safety cabinet by aseptic technique. Tissue samples, aspirates, and swaps were cultured onto 5% blood agar plates, chocolate agar plates, and anaerobic plates (all from SSI Diagnostic). The plates were incubated at 35°C in either a CO2-enriched atmosphere for 3 days or anaerobically for 5 days using the Concept 400 anaerobic workstation (Fisher Scientific, Denmark).
Microbiological Speciation and Susceptibility Testing
Speciation for microorganisms was performed by standard methods 15 or by using the VITEK 2 system. Special care was taken to differentiate (small colony) β-hemolytic group C and G streptococci (Voges-Proskauer test negative) from Streptococcus anginosus (Voges-Proskauer test positive). Organisms of the same species were deemed indistinguishable if they had the same colonial morphology, the same basic biochemical features, and an identical antibiogram. Antibiotic sensitivities were determined by a standard disc diffusion method using the protocol from http://www.srga.org/on isosensitivity plates (Oxoid, Denmark).
Statistical Analysis
The Fisher exact test (2-sided) was used for between-group comparisons of individual bacteriologic findings, Spearman rank correlation was used for between-group comparisons of the distribution of all recovered bacteria, and Wilcoxon rank sum test was used for between-group comparisons of sum of bacteria and between-group comparisons of average times to detection of bacteria in blood cultures. Statistical significance was defined as P < .05.
The study was approved by the Ethical Committee of Aarhus County (number 20050034). All patients were included after informed consent was obtained in accordance with the guidelines from The Danish National Board of Health.
Investigations regarding tonsillar core, pus aspirate, and surface swab bacteriology are presented and discussed in detail elsewhere.
Results
The patient demographics are presented in Table 2. Bacteremia was detected in 56% and 73% of patients during quinsy and elective tonsillectomy, respectively (Table 3). This difference did not reach statistical significance (P = .089, Fishers exact test). The bacteria most frequently isolated from blood cultures of PTA patients were viridans streptococci and Fusobacterium necrophorum ([FN]; Table 3). The predominant bacteria detected from elective tonsillectomy patients were viridans streptococci, Hemophilus influenzae, and S aureus (Table 3). Viridans streptococci were isolated significantly more often (P = .026, Fishers exact test) during elective than quinsy tonsillectomy (Table 3), while FN was isolated significantly less often (P = .004).
Sex and Age Distribution of Patients With Peritonsillar Abcess (PTA), and Electively Tonsillectomized Patients (Elective) With Subgrouping According to Indication for Surgery a
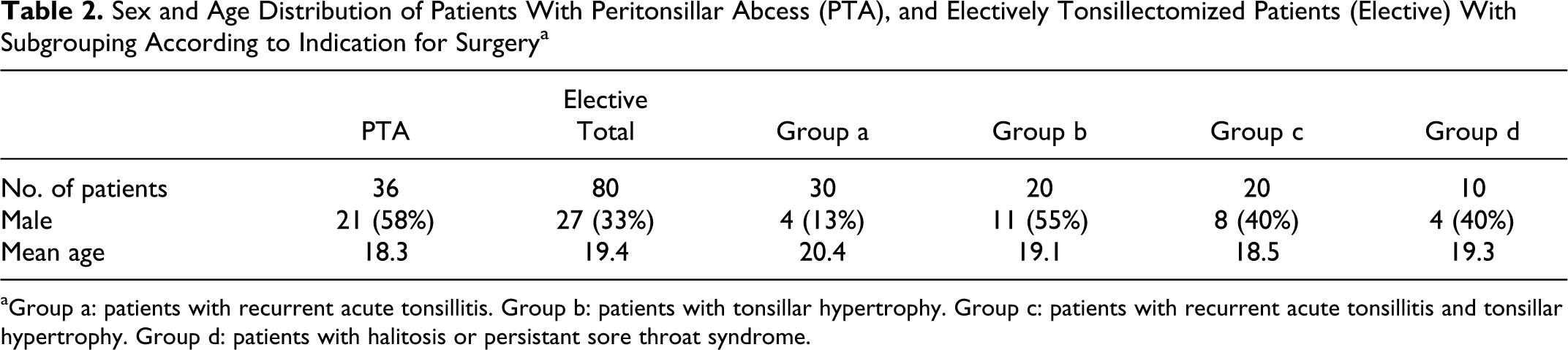
aGroup a: patients with recurrent acute tonsillitis. Group b: patients with tonsillar hypertrophy. Group c: patients with recurrent acute tonsillitis and tonsillar hypertrophy. Group d: patients with halitosis or persistant sore throat syndrome.
Isolates From Blood Cultures Obtained During Quinsy and Elective Tonsillectomy
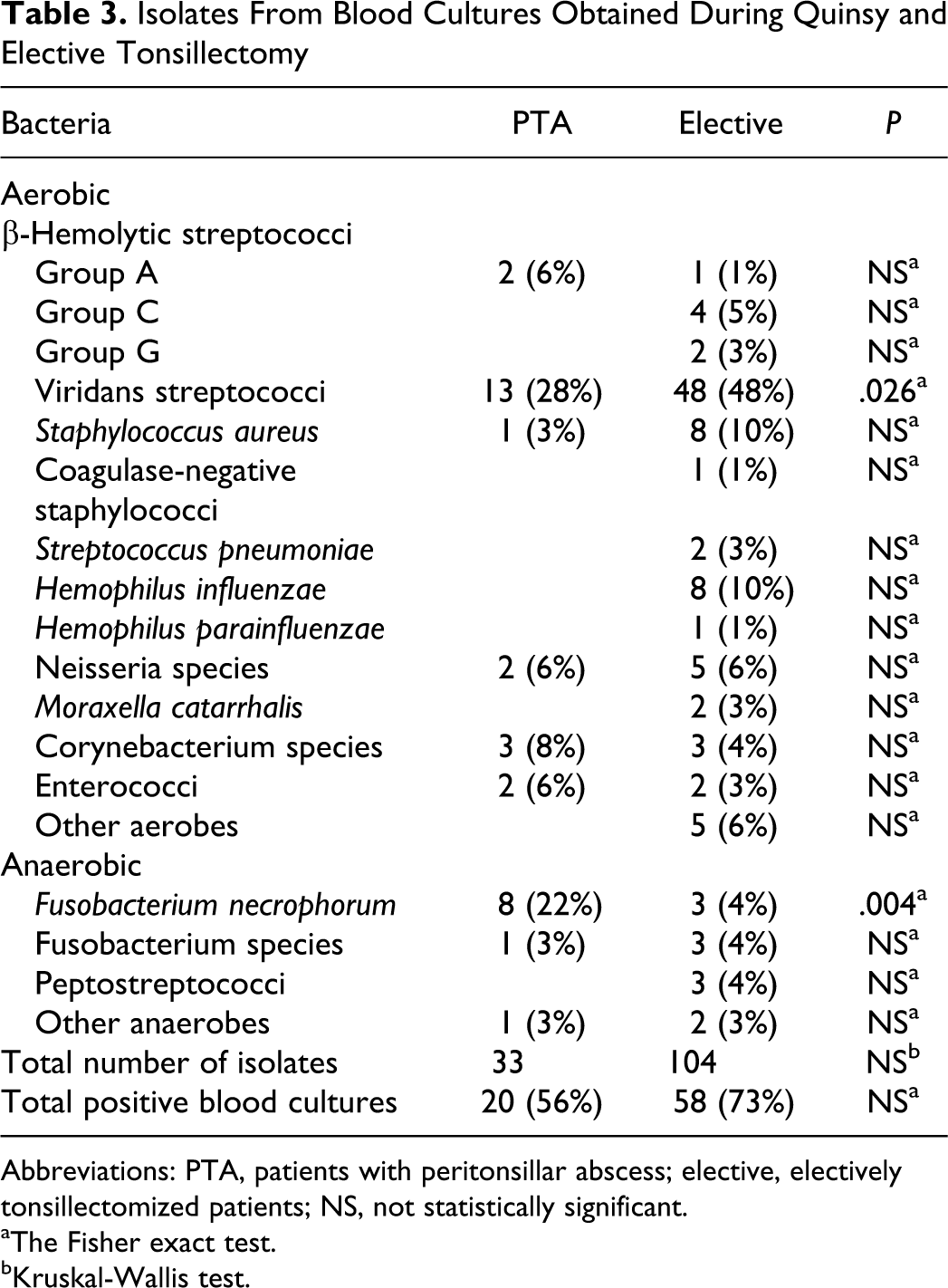
Abbreviations: PTA, patients with peritonsillar abscess; elective, electively tonsillectomized patients; NS, not statistically significant.
aThe Fisher exact test.
bKruskal-Wallis test.
In all, 33 isolates (averaging 0.9 isolates per patient) were grown from blood cultures obtained during quinsy tonsillectomy compared to 104 isolates (an average of 1.3 isolates per patient) among electively tonsillectomized patients. This difference did not reach statistical significance (P = .14, Wilcoxon rank sum test).
Out of 2 aerobic and 2 anaerobic blood culture bottles taken from each patient, 1.1 bottles on average were positive for each strain isolated from quinsy tonsillectomy cases. This was significantly less than the average of 1.7 positive bottles acquired from elective tonsillectomy cases (P < .001, Spearman rank correlation).
The average time to detection of bacteria in blood cultures was significantly (P = .003, Wilcoxon rank sum test) lower in bottles taken during quinsy tonsillectomy (13.7 hours) than in bottles obtained during elective tonsillectomy (19.1 hours).
In electively tonsillectomized patients, 68% and 67% of the 104 isolates were also detected in tonsillar cores and surfaces, respectively. All FN, all S aureus, and 57% of β-hemolytic streptococci (BHS) isolated from blood cultures were also recovered from tonsillar cores.
In PTA patients, 82% of blood isolates were also found in tonsillar cores, 64% in surfaces, and 55% in pus. All BHS and FN detected in blood cultures were also isolated from pus and tonsillar cores. No association was found between the extent of growth of FN and BHS in cultures from tonsillar cores versus blood cultures, both for PTA and electively tonsillectomized patients.
In all, 93% (128 of 137) of the isolated strains were sensitive to amoxicillin, all were sensitive to amoxicillin with clavulanic acid, and 44% (60 of 137) were sensitive to erythromycin.
Discussion
Bacteremia during elective tonsillectomy was found in 73% of patients, which was higher than the detection rates in former studies, which ranged from 7% to 40%.1–10 These studies focused on the pediatric population and required 4 to 20 mL of blood, compared to 40 mL in the present study of primarily young adults. Bacteremia during quinsy tonsillectomy was found in 56% of patients. No previous studies have included PTA patients undergoing acute tonsillectomy.
Somewhat surprisingly, bacteremia was more frequent during elective tonsillectomy than during removal of acutely infected, abscessed tonsils. However, this strong trend did not reach statistical significance. Nevertheless, significantly more blood culture bottles were positive for each strain isolated from elective tonsillectomy patient than from quinsy tonsillectomy patients, indicating higher bacterial load from blood cultures in the former group. On the contrary, the average time to detection of bacteria was significantly shorter in the PTA group than in the elective tonsillectomy group. Taken together, the frequency and quantity of bacteremia during elective tonsillectomy seem at least as high as during quinsy tonsillectomy, if not higher. An explanation could be, that FN, the most frequent pathogen recovered in PTA in this study (recovered from 60% of all PTA aspirates), produces hemagglutinin and thus promotes blood clotting and reduces the flow of bacteria from the tonsil (and abscess) to the blood stream. However, there was no difference in bacteremia rate between patients from whom FN was recovered from tonsillar specimens and patients without growth of FN from tonsillar specimens (P = .86, Wilcoxon rank sum test).
In general, the recovered bacteria were a reflection of the tonsillar core flora, as 68% and 82% of blood culture isolates were also found in the tonsillar cores of electively tonsillectomized and PTA patients, respectively. Accordingly, FN was detected significantly more frequently and viridans streptococci significantly less frequently in PTA patients than electively tonsillectomized patients.
Of note, FN was detected in 22% of blood cultures from PTA patients. The bacterium is most commonly associated with Lemierre syndrome. Fusobacterium necrophorum bacteremia in patients with other conditions is scarcely reported. However, in our study, the patients did not develop metastatic infections or have complications secondary to their bacteremia. This was true not only in the context of FN bacteremia but for all isolates. This observation emphasizes that the bacteremia associated with tonsillectomy is transient and does not lead to complications in patients without comorbidities predisposing them to infective endocarditis.
The predominant causative bacteria in infective endocarditis are viridans streptococci, staphylococci, enterococci, and BHS. Hemophilus species are less frequently a cause. Only 3 cases of FN endocarditis have been previously reported. 16 Sixty-one percent of the bacteria detected in the present study are among the causative organisms in endocarditis. In all, 59% and 42% of electively and acutely tonsillectomized patients, respectively, had bacteremia with such bacteria. Hence, our study demonstrates that a significant proportion of patients have bacteremia with microorganisms associated with endocarditis. However, the study cannot provide an exact quantification of colony-forming units per milliliter blood, and we are therefore unable to evaluate the importance of antibiotic prophylaxis in patients at risk of infective endocarditis. Nevertheless, our findings do not support the need for additional or altered prophylaxis in PTA patients undergoing acute tonsillectomy. Most importantly, our results challenge the distinction made by the European Society of Cardiology between elective and quinsy tonsillectomy, with regard to antibiotic prophylaxis. 14 In fact, the trend from our study suggests that antibiotic prophylaxis seems just as, if not more, important in patients undergoing elective tonsillectomy.
In the only previous study comparing bacteremia during tonsillectomy in patients with RT versus TH, Esposito et al found a higher prevalence of bacteremia in patients with recurrent infections. They concluded therefore that the risk of bacteremia is minimal when operating on a noninfected site, even if the site is colonized by potential pathogens. 10 Our bacteremia detection rates of 72% in patients with RT and of 73% in patients without do not support that there are differences in bacteremia rates according to the different indications for tonsillectomy and quite clearly oppose the belief that removal of clinically noninfected tonsils does not cause bacteremia. The new guidelines from the European Society of Cardiology do not discriminate between removal of recurrently and not recurrently infected tonsils, but the findings of Esposito et al 10 might have influenced the guidelines on distinguishing between elective and quinsy tonsillectomy.
One limitation of the present study is the fact that patients included here were children and young adults, whereas most patients with infective endocarditis are older. Whether predominant bacteria in peritonsillar abscesses are related to age have not been studied, but tonsillar flora are different between children and adults with RT. 17
Ninety-three percent of the isolated strains were sensitive to amoxicillin and all were sensitive to amoxicillin with clavulanic acid. In order to get full empiric coverage, including coverage of S aureus, we advocate the use of amoxillin with clavulanic acid in patients fulfilling the criteria listed in Table 1. The addition of clavulanic acid is more important in patients undergoing elective than quinsy tonsillectomy, as S aureus is frequently isolated in recurrent and hypertrophic tonsils but does not seem to play an important role in PTA. Clindamycin can be used for individuals who are allergic to amoxicillin.
Conclusion
In all, 59% and 42% of electively and acutely tonsillectomized patients, respectively, had bacteremia with microorganisms that are predominant in bacterial endocarditis. These results challenge the distinction made by the European Society of Cardiology between elective and quinsy tonsillectomy, namely that antibiotic prophylaxis is the only recommendation to patients undergoing procedures to treat an established infection. Based on our findings, we advocate the use of amoxicillin with clavulanic acid in patients at high risk of developing infective endocarditis.
Footnotes
Acknowledgments
The authors acknowledge the Department of Biostatistics, Aarhus University, Denmark, for the advice concerning statistical analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.