
Abstract
Objective:
Migraine is a debilitating disease affecting a large number of young people. In this study, he aim was to assess the extracranial arteries during migraine headaches and non-headache headache intervals using sonography.
Materials and Methods:
The study enrolled 210 patients with confirmed migraine headaches. The vertebral arteries, superficial temporal arteries, internal carotid arteries (ICAs), and common carotid arteries were assessed using a sonographic method. Grayscale and spectral doppler criteria, such as the diameter of arteries, peak systolic velocity (PSV), and pulsatility index (PI), during migraine headaches and non-headache headache intervals were measured.
Results:
Assessing the vertebral and external carotid arteries, a significant difference was observed between the diameter of the arteries during active headaches and that during non-headache headache periods. The mean PSV of ICA during active headaches was 60.05 cm/s, which was lower than that during non-headache headache periods, which was 69.35 cm/s (P = .016).
Conclusion:
In this cohort’s migraine headaches, the diameter of the superficial temporal artery and ICA are increased and the diameter of the vertebral artery is decreased. Decreased PSV of the vertebral artery in contrast with increased PSV of the temporal artery is seen during headaches. These diagnostic findings may be useful in predicting migraine headaches and should be replicated with other patients.
A migraine headache is a chronic and debilitating disease that usually affects a large number of young people. Its prevalence is estimated to be 12% in the population. 1 This is the most common neurological disease affecting the quality of life of in the United States and Europe.1–5 In addition, a migraine is defined as severe headache attacks leading to reduced work performance more commonly in females.6–9 In late 1930, Wolff was the first to use a vascular theory to explain the cause of migraine headaches. 10 This theory consisted of two parts. The first one is intracranial vessel constriction that causes an aura, and the second one is dilation of extracranial vessels, leading to migraine headaches. 10 Wolff measured temporal artery diameter in patients with a migraine and found it to be increased. 10 Following treatment with vasoconstrictive drugs such as ergotamine, temporal artery vasoconstriction and significant pain relief were noted. 10 Even though the reason for vasodilatation and related symptoms was not clear, 11 arterial pulsation can activate chemoreceptors causing neuropeptide releases and pain. 12 As arteriovenous anastomosis of the carotid artery has an important role in the pathogenesis of migraine disease, the administration of vasoconstrictive drugs can be effective in relieving migraine symptoms.13,14 Later studies have revealed that the 5-hydroxytryptamine receptor 1B in arteriovenous anastomosis of the carotid, temporal, and middle meningeal arteries plays a significant role in the sumatriptan-relating vasoconstriction. 15 According to previous studies, intracranial blood flow changes during migraine headaches and can cause electrical brain stem stimulation. 16 These studies have assessed the relationship between the trigeminal nerve and cranial arteries and demonstrated that vasoactive peptides released from trigeminovascular axons can cause a sterile inflammatory process, leading to pain.17,18 During this neurogenic inflammation, the trigeminal ganglion is stimulated and releases neurogenic proteins followed by vasodilation peptides such as calcitonin gene-related peptide. This theory is an attempt to reveal the role of vessel changes, with neuronal dysfunction, in migraine disease and includes headache attacks being related to inflammation and vasodilation, in the meninges and dura.19,20,21 Previous studies have tried to show the changes in diameter and hemodynamics of extracranial arteries, such as vertebral arteries, internal carotid arteries (ICAs), and temporal arteries, during migraine headaches. In most of the abovementioned studies, only a few extracranial arteries were studied.22–30 Given the fact that migraine is a debilitating disease, which can significantly reduce the quality of life, especially among teenagers and young people, the objective was to assess vertebral arteries, superficial temporal arteries, ICAs, external carotid arteries (ECAs), and common carotid arteries (CCAs) of patients with migraine disease, using sonography. By comparing the diameter of arteries, pulsatility index (PI), resistive index (RI), and peak systolic velocity (PSV), during migraine headache attacks and nonheadache intervals, the aim was to gain a better understanding of the vascular changes during active headaches. This would also allow clinicians to potentially improve diagnosis, treatment, and surveillance of these patients. This could lead to a greater value for patients if minor changes in diameter and PSV can be managed clinically, and thereby negate severe migraines.
Materials and Methods
The local ethics committee approved this case-control study, and informed consent was obtained from patients recruited to the study. The inclusion criterion was patients with migraine disease, within the last 5 years, based on the International Classification of Headache Disorder, third edition, criteria. 26 The exclusion criteria were patients with cardiovascular disease, patients with autoimmune disease with possible vascular involvement, such as giant cell arteritis, as well as patients with atherosclerotic plaques on assessed arteries, patients unable to cooperate during sonography, and the recent use of any vasoconstrictive drug, such as ergotamine, as a treatment for headaches. In total, a cohort of 223 patients with migraines were identified. Eight patients were excluded due to the presence of atherosclerotic plaques, mainly in ICAs and ECAs. An additional seven patients were excluded due to a medical history of cardiovascular disease. A total of 210 patients have been evaluated from March 2020 to April 2021. For some of these patients, this was the first time that the arteries had been assessed for the presence of migraine disease.
Grayscale sonography and spectral doppler were used by a diagnostic radiologist with 20 years of experience in vascular sonography. The radiologist did not have access to the anonymized patient’s symptoms. The examinations were completed using a Samsung WS80A ultrasound equipment system (Samsung Electronics, UK Limited, Samsung Medison, Seoul, South Korea) equipped with a linear array transducer (5–10 MHz). This system was used for assessing vertebral arteries, superficial temporal arteries, ICA, ECA, and CCA. The diameter, PI, RI, and PSV of arteries were measured during migraine headache attacks. The patient completed the sonographic examination on the first day of the headache, before receiving any medication, and also during symptom-free intervals. The CCA was assessed in its middle third part, and ECA and ICA were assessed in the first third of the arteries. Vertebral arteries were assessed on the plane, which showed its bifurcation. The temporal artery was measured at the retromandibular area, in front of the ear auricle (see Figures 1–4).
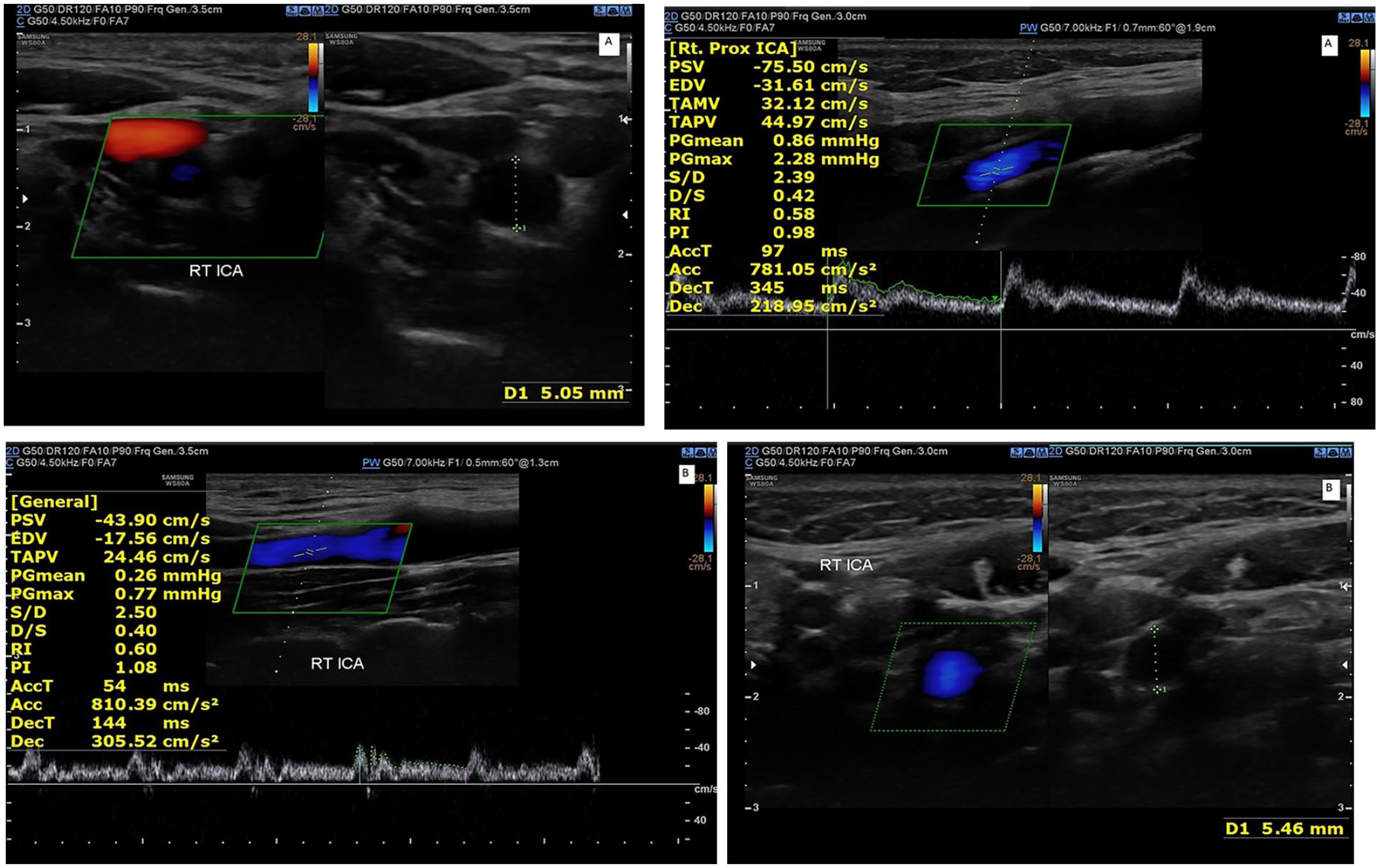
Comparing the diameter and PSV of the internal carotid artery in a patient during a non-headache interval (A1 and A2) and during an active headache (B1 and B2) using spectral Doppler. These images demonstrate an increased vessel diameter, and a decreased PSV, during the active headache phase. PSV, peak systolic velocity.
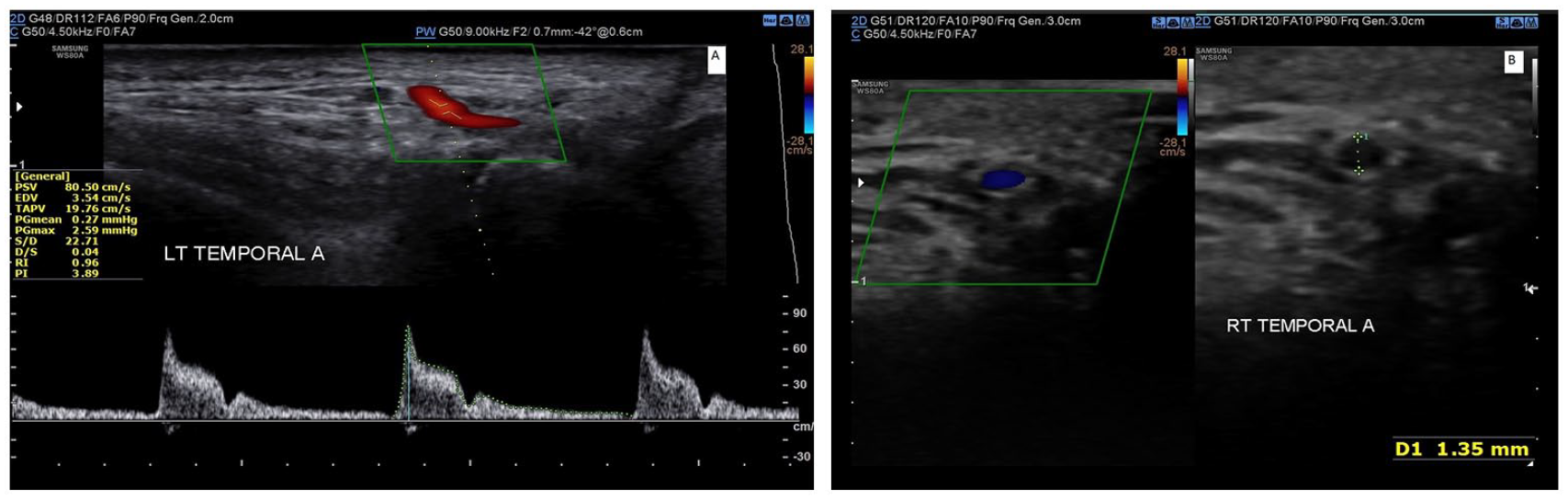
These images demonstrate measuring the peak systolic velocity (PSV), pulsatility index, and resistive index of the left temporal artery using spectral doppler, as well as the diameter of the right temporal artery with grayscale sonography.
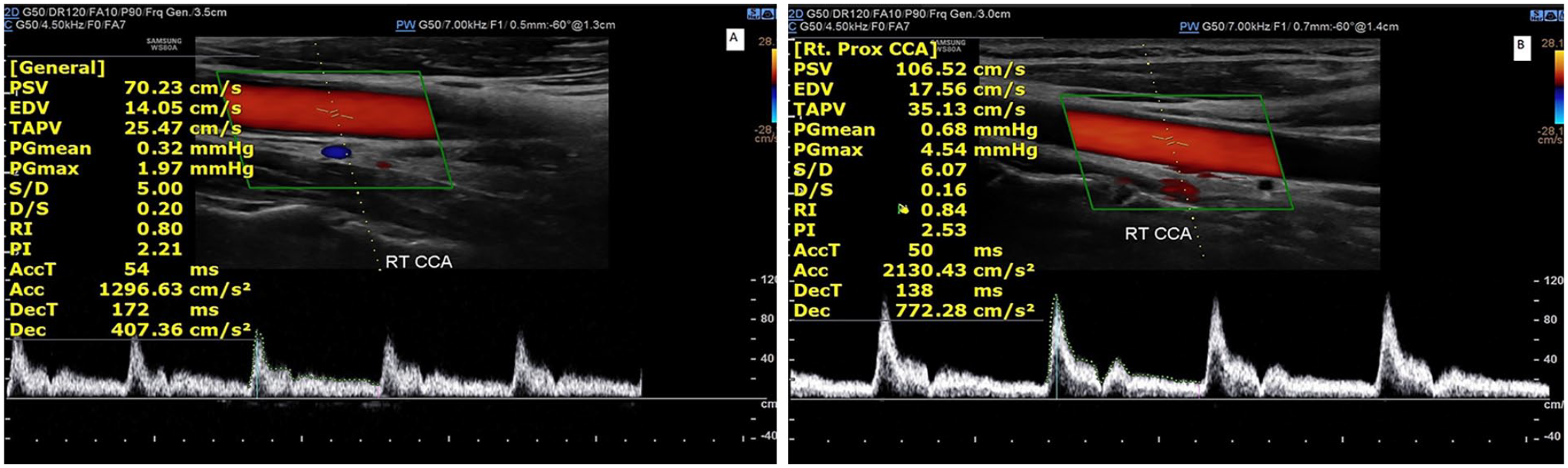
An image demonstrating the measurement of the PSV, pulsatility index, and resistive index, within the right common carotid artery, using spectral doppler for a patient with an active headache (A) and during a non-headache phase (B). This demonstrates how the velocity measurements show a decreased PSV during an active headache phase. PSV, peak systolic velocity.
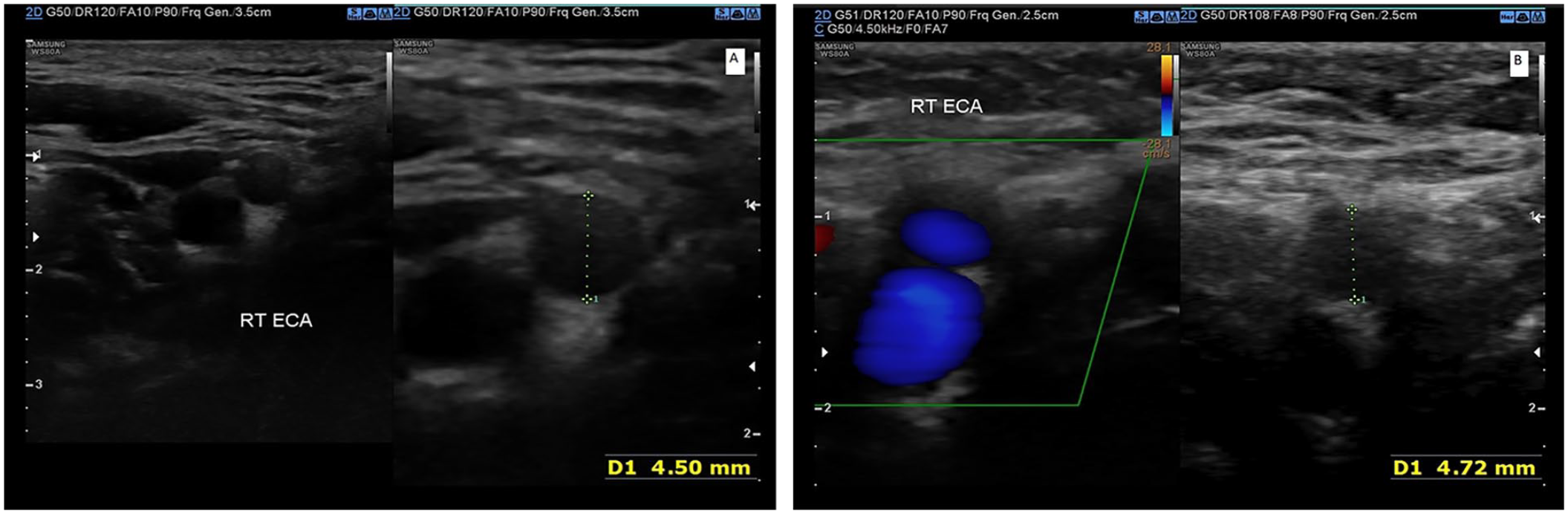
This set of images demonstrate the measurement of the diameter of the right external carotid artery using sonography in a patient during a non-headache interval (A) compared to an active headache (B). This set of images demonstrate an increased diameter during the active headache phase.
Statistical Analysis
The imaging data were reported and analyzed using a paired t-test, as well as calculating means and frequencies. The analysis was completed using SPSS version 24 (SPSS Inc., Chicago, IL, USA). The statistical significance was set a P < .05, a priori.
Results
Two hundred ten consecutive patients with migraines were included in this cohort study. The mean age of patients was 34.75 years. Patients' age was between 22 and 48 years. Of the 210 patients studied, 106 had right-sided headaches, and 104 had left-sided ones. Ninety-eight (46%) patients were male, and 112 (53%) were female.
Vertebral Artery
In this cohort, during active headaches, the mean PSV of vertebral arteries was 44.17 cm/s, and during non-headache periods, it was 49.67 cm/s (P = .008). The mean diameter of this artery during active headaches and non-headache intervals headaches was 2.91 mm and 3.43 mm, respectively, which was statistically significant (P = .009) (see Tables 1 and 2).
The Cohort Mean of Grayscale Sonography and Spectral Doppler in Assessing Extracranial Arteries During Active Headaches and non-Headache Intervals for Patients With Migraine Disease.
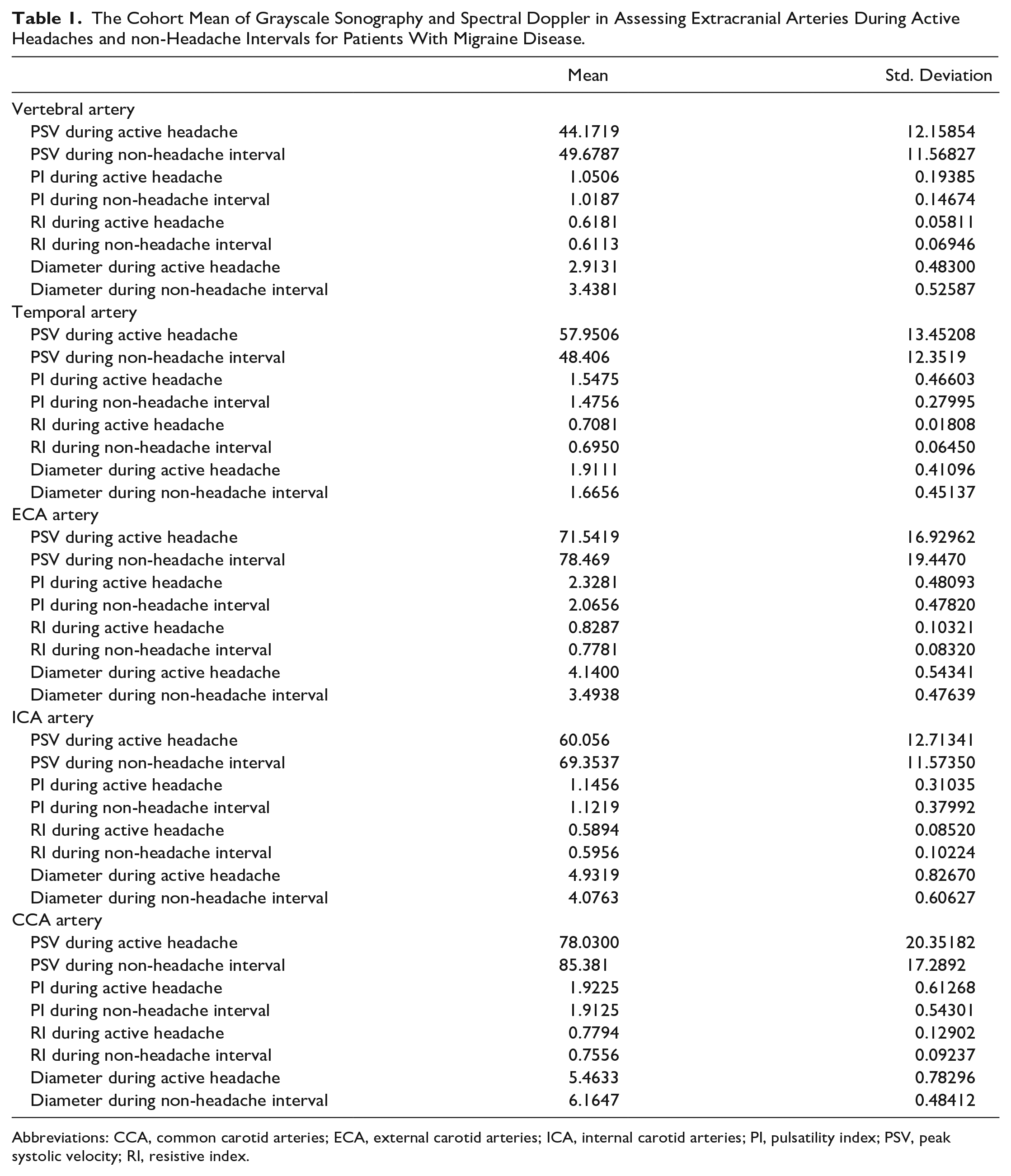
Abbreviations: CCA, common carotid arteries; ECA, external carotid arteries; ICA, internal carotid arteries; PI, pulsatility index; PSV, peak systolic velocity; RI, resistive index.
The Comparison Between Grayscale Sonography and Spectral Doppler Data for Assessing Extracranial Arteries During headache and non-headache intervals Among Patients With Migraine Disease.
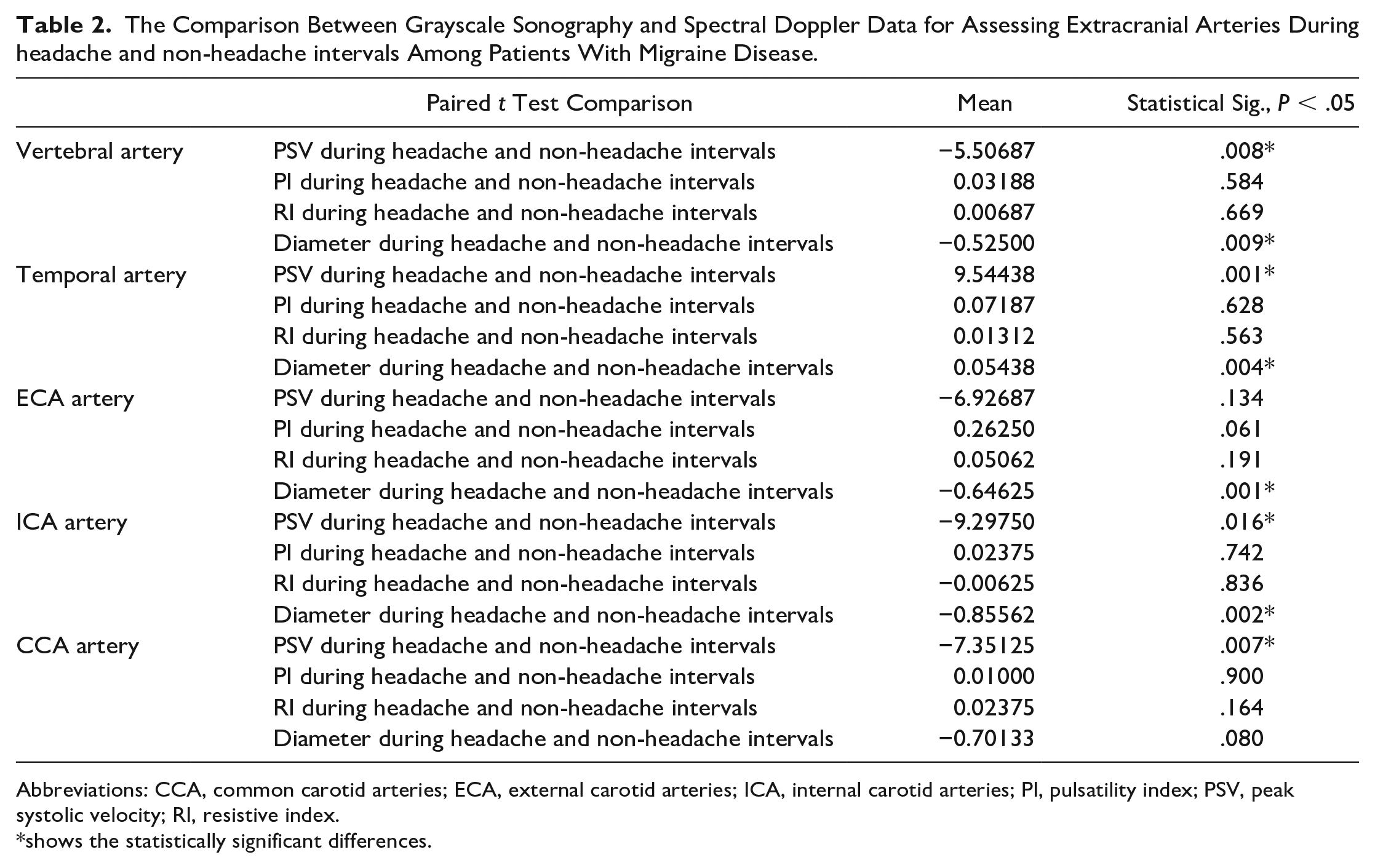
Abbreviations: CCA, common carotid arteries; ECA, external carotid arteries; ICA, internal carotid arteries; PI, pulsatility index; PSV, peak systolic velocity; RI, resistive index.
shows the statistically significant differences.
Superficial Temporal Artery
The cohort mean PSV within the superficial temporal artery during active headaches (57.95 cm/s) was more than that during inactive headaches (48.40 cm/s), which was also statistically significant (P = .001). The mean diameter of this artery during active headaches was 1.91 mm (increased), and during the inactive headache period, it was 1.66 mm and was statistically significant (P = .004).
External Carotid Artery
The mean PSV, PI, and RI in this artery were 71.54 cm/s, 2.32 cm/s, and 0.82 cm/s, respectively, during an active headache and 78.46 cm/s, 2.06 cm/s, and 0.77 cm/s, respectively, during non-headache periods; however, the differences noted were not statistically significant (P > .05). The mean diameter of ECA during active headaches was 4.14 mm (increased), and during non-headache periods, it was 3.49 mm and statistically significant (P = .001).
Internal Carotid Artery
The mean PSV, within the ICA, during an active headache was 60.05 cm/s, which was lower than that in the non-headache period at 69.35 cm/s (P = .016). There were no statistically significant differences between the PI and RI of this artery during active headaches and non-headache periods (P > .05). A statistically significant difference was detected between the diameter of the ICA during active headaches (4.93 mm) and that during non-headache periods (4.07 mm) (P = .002).
Common Carotid Artery
The mean PSV of the artery during an active headache was 78.03 cm/s, and during non-headache periods, it was 85.38 cm/s; the difference noted was statistically significant (P = .007). The mean diameter of CCA during active headaches was 5.4 mm, which was less than that during non-headache periods, at 6.1 mm, which was not statistically significant (P = .080).
Discussion
This study investigated the diagnostic role of grayscale sonography and spectral Doppler within the extracranial arteries in a cohort of patients with migraine disease. This study showed that the diameter and PSV of the vertebral artery during active headaches were less than those during non-headache periods; however, previous studies did not assess this artery during migraine headache attacks or non-headache periods. Nevertheless, in a comparative study, there was an association between vertebral artery hypoplasia and migraine disease. 31 The vertebral arteries feed the posterior circulation, and the fact that they are narrower may suggest that this distribution is usually spared in migraines, so no compensatory dilatation is required.
A migraine causes brain swelling and a mild increase in intracranial pressure, which, without compensation, causes vasospasm in the intracranial arteries. A compensatory mechanism would be dilatation of the inflow vessels to the brain, such as the ICA, to get as much blood to the central vasculature as possible, during the migraine headache. The present study results demonstrated an increased diameter of the temporal artery during active headaches, consistent with previously reported studies.32,33 Spectral Doppler of the ECA, during an active headache, revealed an increased diameter of the artery as well. This finding was similar to previously published work using magnetic resonance angiography (MRA).17,23 The present study results did not demonstrate a significant difference in the PSV within the ECA, between active migraines and symptom-free intervals. This was in contrast with the findings by Kalashnikov et al 29 that showed significantly lower velocity of the artery during active headaches.
In assessing the ICA, a significant difference was detected between the PSV and the diameter of the artery during an active headache and symptom-free intervals, which showed the increased diameter of the artery during attacks. These study results were consistent with the published findings in previous studies.23,24 Based on the present study results, the PSV of CCA during active headaches was significantly lower than that during non-headache periods; however, this artery has not been assessed previously.
Limitations
This cohort study has limitations. The limited number of patients may bias the results. In this study, ultrasonography findings of patients had not been assessed based on subtypes of migraine such as migraine with or without aura..
Conclusion
This cohort study represents a first diagnostic attempt to use various criteria of spectral doppler to assess different extracranial arteries. The present study results showed that during a migraine headache, the diameter of the superficial temporal artery, ICA, and ECA were increased, and the diameter of the vertebral artery was decreased. Additionally, the decreased PSV within the vertebral artery, ICA, and CCA were in contrast to the increased PSV within the temporal artery, noted during active headaches. These findings warrant further investigation with larger cohorts and using other diagnostic imaging modalities, such as MRA and sonography, for more confirmatory results. Furthermore, future studies might demonstrate the effectiveness of extracranial artery sonography during specific time intervals. For instance, monthly intervals for assessing the diameter and PSV of arteries for tracking any minor changes which could predict the onset of future migraine headaches. Therefore, knowing the approximate time of a pending headache might allow for better medical management and negating severe migraine headaches.
Footnotes
Author’s Note
Neda Akhoundi is also affiliated to Radiology Department, Hillcrest Hospital, University of California San Diego, CA, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because the local ethics committee approved this case-control study, and informed consent was obtained from patients.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
Not applicable.