
Abstract
A rare case of proximal focal femoral deficiency (PFFD) is presented due to concerns for a short fetal femur. A 32-year-old patient (G3P2002) was reviewed at 37 weeks of gestation. Sonography revealed an appropriately maturing female fetus, with a left femoral diaphyseal length of 36.1 mm (<1st percentile), while the right measured 71.4 mm (35th percentile). The proximal epiphysis, head, and trochanter of the left fetal femur were absent on 3D sonography, with significant overlap of the femur on the pubic bone. At delivery, the baby weighed 3240 g, with a lower limb-length discrepancy of 56 mm. A radiograph confirmed left-sided hypoplastic proximal femur, absent femoral head, and a poorly formed acetabulum. The baby was conservatively managed, with plans for possible surgery and limb prosthesis. A high index of suspicion and capacity building to facilitate prenatal diagnosis are essential for optimal care of babies with PFFD.
Proximal focal femoral deficiency (PFFD) is a rare cause of short fetal femur that occurs with a frequency of 1.1–2.0/100 000 live births and a male-to-female ratio of 1:2. The anomaly results from a failure of development of the proximal part of the femur, with or without acetabular dysplasia. 1 Clinically, PFFD ranges from femoral shortening with a coxa vara anomaly in the mild variant to the most severe forms in which only the distal femur, represented by a distal ossicle, is present. It is unilateral in 85% of cases, with resultant limb asymmetry.1,2 Prenatal diagnosis of PFFD is often missed due to its rarity and the tendency to measure just one femoral length during prenatal sonography.
Prenatally diagnosed PFFD should be appropriately classified for the purpose of prognostication and appropriate counseling of the expectant parents. The most used system is the Aitken classification, which involves types A–D. 3 In type A, the femoral head is attached to the shaft by the femoral neck with mild shortening of the femur. Type B is characterized by further shortening of the femur, a normal or mildly dysplastic acetabulum, and a discontinuity between the proximal femoral shaft and the head. In type C, there is an increased degree of acetabular dysplasia, absence of the femoral head, and disconnection with the severely dysplastic acetabulum, with a short and tapered femoral segment proximally. Type D represents the most severe form of PFFD that entails the absence of the acetabulum and proximal femur, with a severely shortened femoral segment. 3
While a suspicion of skeletal dysplasia or femoral abnormality can arise prenatally, during fetal sonography, accurate diagnosis of PFFD is challenging due to the rarity of femoral abnormalities and the wide spectrum of skeletal dysplasia. 1 The case of a prenatally diagnosed PFFD at a Nigerian teaching hospital is hereby presented.
Case Report
A 32-year-old patient (G3P2002) was reviewed, at 37 weeks of gestation, due to the report of a shortened femur, of unknown laterality, on a previous sonogram. There was no history of maternal chronic illness or exposure to teratogens. The new sonogram revealed a female fetus, at the 45th percentile of weight expected for gestational age. The left femoral diaphyseal length, however, measured 36.1 mm (<1st percentile), while the right measured 71.4 mm (35th percentile), with a ratio of 0.51 (Figure 1). The proximal epiphysis, head, and trochanter of the left femur were absent on 3D sonogram, while the right femur appeared normal (Figure 2). The length of the other long bones ranged between the 35th and 48th percentiles as expected, without bowing or fracture. The chest circumference was normal, with a cardiothoracic ratio of 41%. The patient was counseled on the diagnostic findings, and a delivery plan was made.
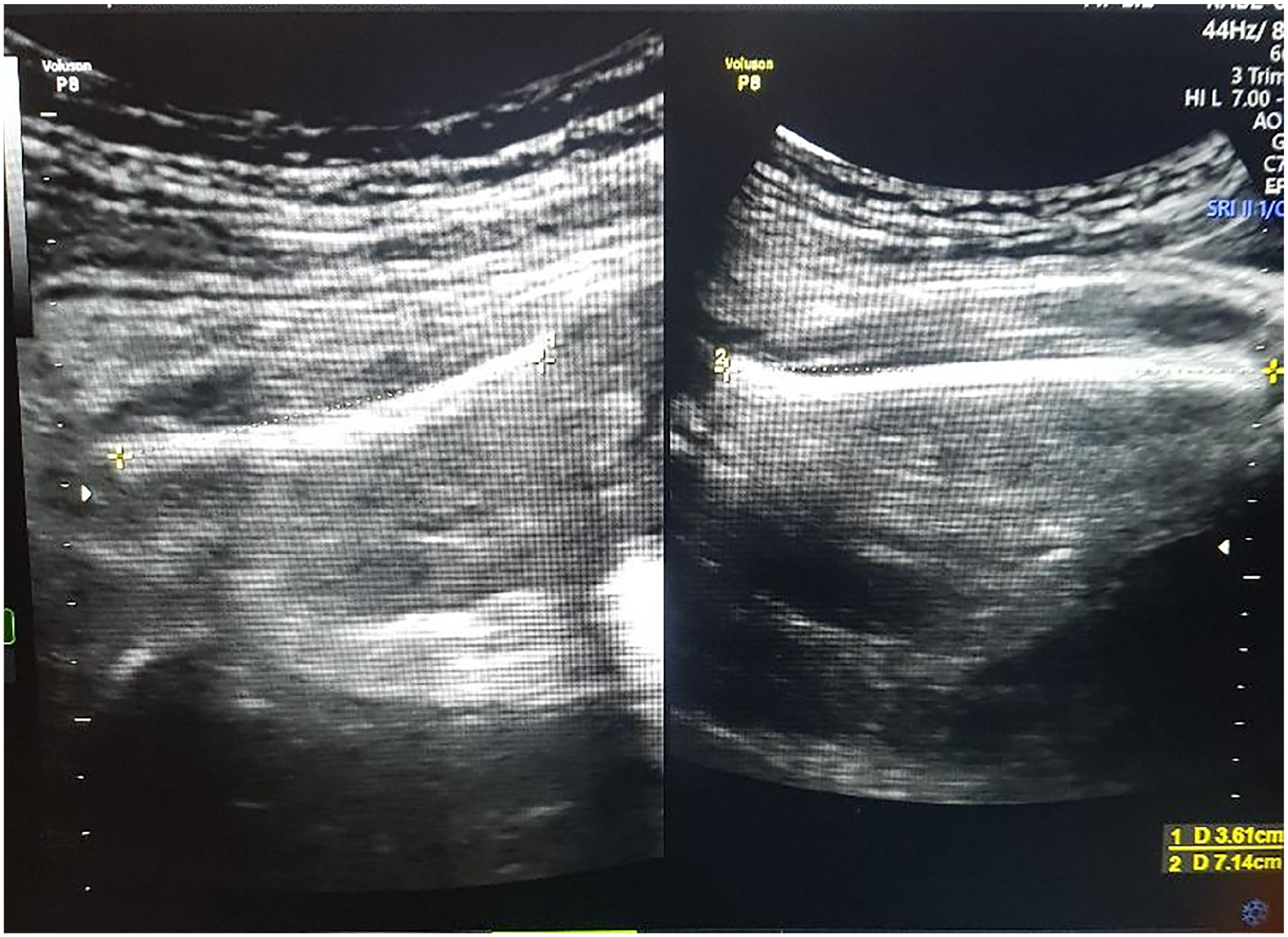
Prenatal sonogram of the short femur (left) and the normally developed contralateral femur (right) of the fetus and their measurements.
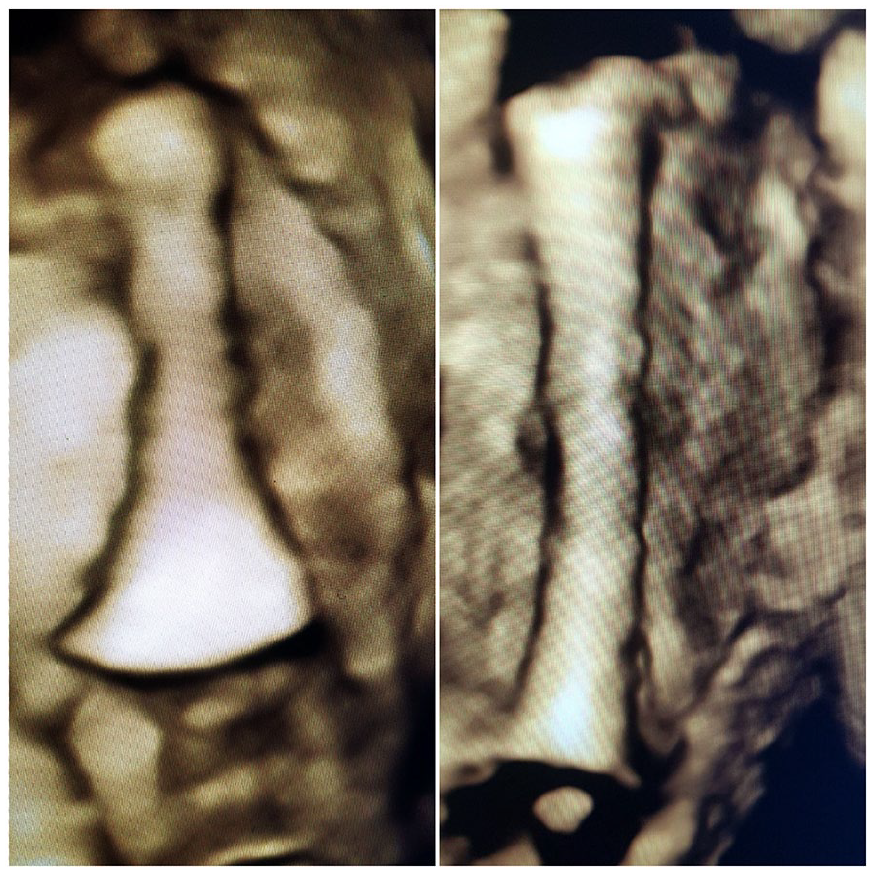
Three-dimensional sonographic rendering of the short femur with hypoplasia of the proximal part (left) and the normally developed contralateral femur (right) of the fetus.
She delivered a female baby with a birth weight of 3240 g and APGAR scores of 8 and 10 in the first and fifth minutes, respectively, at 39 weeks of gestation. There was a lower limb-length discrepancy of 56 mm, with the deficit on the left femur. There was no fracture or inflammation on the thigh. The spine, knee joints, legs, feet, and neurovascular structures were intact. The radiograph taken revealed a left-sided hypoplastic proximal femur, absent femoral head, and a poorly formed acetabulum (Figure 3). The skull, rib cage, and other long bones were normal. This confirmed the sonographic finding of a dysplastic left hip socket with disarticulation of the hip joint.

The radiograph of the newborn demonstrating the short left femur (arrow) relative to the right femur.
The baby was managed by the multidisciplinary team and discharged home on the third day, with plans for a possible surgery and limb prosthesis. She was clinically stable, with limb discrepancies of 52 mm and 49 mm on the 6th-week and 12th-week outpatient visits, respectively, (Figure 4).

A physical examination, after delivery, for comparison of the two lower limbs.
Discussion
The etiology of PFFD is not known with certainty, although the pathogenesis entails defective chondrocyte proliferation and maturation in the proximal femoral growth plate. 1 In utero exposure to thalidomide, radiation, toxic chemicals, and trauma has been suggested as possible contributors. 4 Aneuploidies, especially trisomy 21, as well as alterations in the genes that regulate central and appendicular skeletal developments, such as the paralogous gene families Hox 9, 10, 11, 12, and 13, may be involved.4,5 The other families of genes that may be implicated in the pathogenesis of PFFD include TBX4, FGF, FGFR, TP63, and WNT7A.3,6,7 It is proposed that the phenotypic expression of PFFD may be directly proportional to the number of mutated alleles in these family of genes. While most cases are sporadic, rare cases of familial occurrence are possible.5,6 In the present case study, there was no identifiable risk factor.
A femoral diaphyseal length that is less than the 5th percentile for the gestational age, with sonography, should raise suspicion for PFFD. A tapering proximal femur and asymmetry of the two femurs could further support the diagnosis. Accurate sonographic measurement of the femoral diaphyseal length requires strict compliance with quality-assurance measures, as recommended by the International Society of Ultrasound in Obstetrics and Gynecology. 8 A prenatal diagnosis of PFFD may be further improved upon by using advanced ultrasound equipment systems such as 3D sonography, with skeletal rendering, as done in the present case study. Four-dimensional sonography may aid in a detailed assessment of the range of motion of the affected limb. 9 Using the Aitken classification, 3 the index case was classified as PFFD type C because the femoral head was absent, the proximal femur was poorly developed, and the acetabulum was dysplastic. 3 Although the Amstutz classification is an alternative classification system, 10 the Aitken system was used in this case, as the Amstutz system may not be used for babies less than a year old.
The differential diagnoses of PFFD included congenitally short femur, which is always bilateral. In addition, femoral-fibula-ulna syndrome was considered, given that it involves the femur, ulna, and fibula. Finally, femoral-facial syndrome was also a diagnostic consideration, which involves the femur, associated lip, nose, and palatal dysgenesis, with or without micrognathia. Some other disorders of skeletogenesis include thanatophoric dysplasia, osteogenesis imperfecta, chondroectodermal dysplasia, and achondroplasia, all of which tend to involve the appendicular bones globally.3,4,7 The diagnosis of PFFD was, however, made in the present case study as the anomaly was confined to the left fetal femur and acetabulum.
If uncorrected, PFFD may predisposed to gait disabilities with scoliosis, leading to severe, early-onset back pain. The management may include surgical rotationplasty, limb lengthening, total hip replacement, and prosthetic support, with the aim of synchronizing the limb lengths, as well as stabilizing the hip joint and feet.11,12 Optimal adjustment to physical activities and improvement in the quality of life following these interventions have been described. 8
Proximal focal femoral deficiency is not commonly reported in medical literature due to the rarity of the condition.2,13 Consequently, only few cases of PFFD have been reported in Nigeria,4,5 and none of these was diagnosed prenatally; documentation of this patient case was, therefore, necessary. In addition, the prenatal ultrasound images of PFFD as presented may facilitate the recognition of the condition by other practitioners. The late diagnosis of short femur at 37 weeks of gestation, as in this case, underscores the need to improve on the general pattern of delayed recognition or non-recognition of congenital anomalies.
Conclusion
PFFD is a rare congenital anomaly of the femur, which is often missed prenatally due to its rarity and the wide spectrum of skeletal dysplasia. A high index of suspicion and capacity building to facilitate prenatal diagnosis are essential for optimal patient care.
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because the case was anonymized, and appropriate measures were taken to ensure the rights of the patient were respected.
Informed Consent
A written informed consent was obtained from the patient.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.