
Abstract
Osler-Weber-Rendu syndrome, also known as hereditary hemorrhagic telangiectasia (HHT), is a rare inherited disorder characterized by the presence of systemic arteriovenous malformations, which most commonly affects the liver. One of the most serious complications of liver compromise is high output heart failure (HOHF). In this case study, point-of-care ultrasonography is utilized as a means to describe the diagnostic findings of an intensive care unit patient diagnosed with liver involvement of HHT and the development of HOHF.
Keywords
Osler-Weber-Rendu syndrome, also known as hereditary hemorrhagic telangiectasia (HHT), is a rare inherited disorder characterized by the presence of systemic arteriovenous malformations (AVM). Its incidence is one or two cases out of 100 000 subjects. 1 The Curaçao diagnostic criteria are used for diagnostic purposes and include four findings: spontaneous and recurrent epistaxis, multiple mucocutaneous telangiectases at characteristic sites, visceral involvement, and a first-degree relative with HHT. Depending on the number of criteria, the diagnosis is categorized as definite with three or more criteria, suspected with two criteria, or unlikely with one criterion.2,3 In patients with HHT, liver involvement is a common finding, these patients are typically asymptomatic, and it is more prevalent among females. 3 One of the most serious complications of liver compromise is the high output heart failure (HOHF) which has been reported to vary between 25% and 65%.1,4 In this case study, point-of-care ultrasonography (POCUS) is utilized as a means to describe the diagnostic findings of an intensive care unit (ICU) patient diagnosed with liver involvement of HHT and the development of HOHF.
Case Report
A 75-year-old woman with clinical history of diabetes, obesity, and HHT presented to the ICU with pneumonia and a tracheostomy. The patient was responding well to antibiotic treatment but required mechanical ventilation support. After presenting with hypoxemia, a POCUS was performed demonstrating bilateral B lines in the lungs comparable with alveolar-interstitial syndrome (see Figure 1), preserved biventricular systolic function, impaired left ventricular filling pattern with E/e′ ratio of 38, biatrial enlargement, and dilated cardiomyopathy (see Figures 2 and 3).
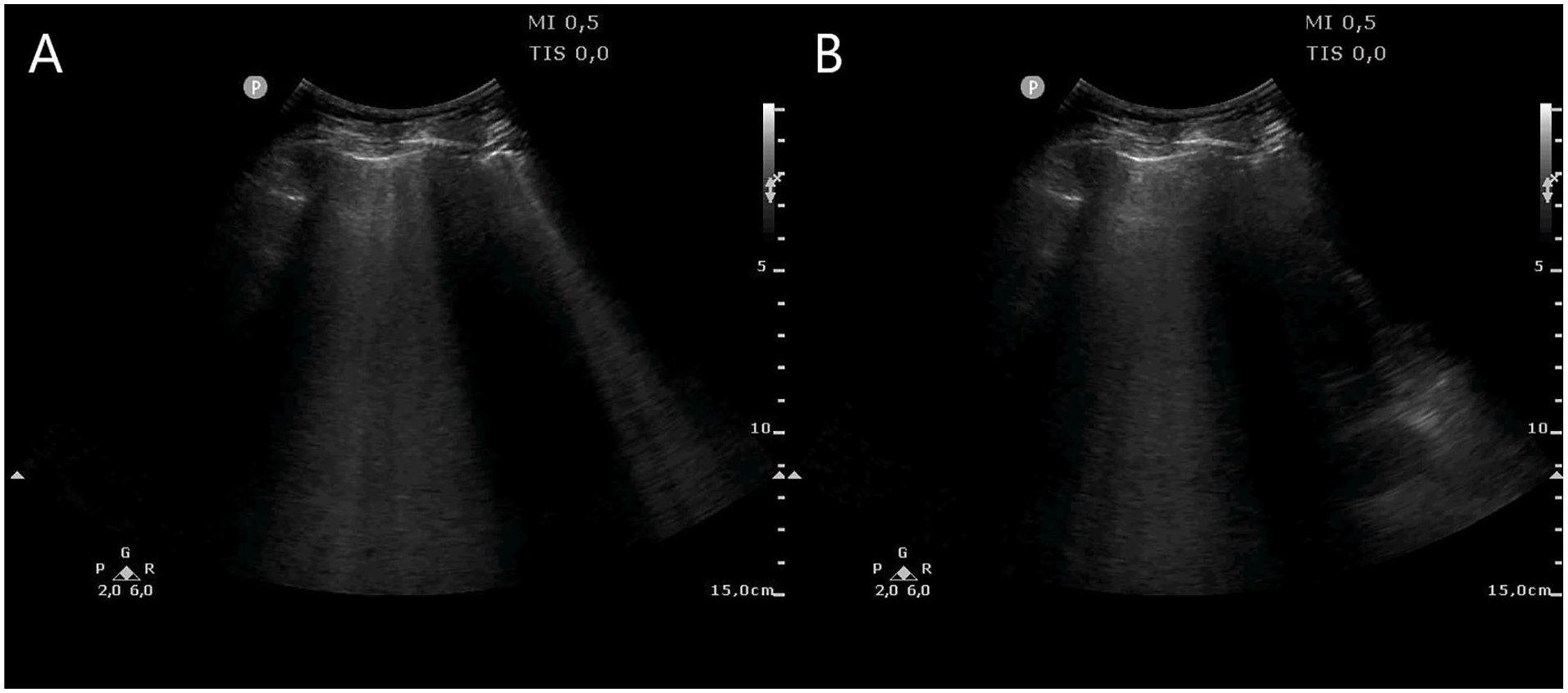
Lung sonogram with multiple B lines in the right (A) and left (B) hemithorax compatible with alveolar-interstitial syndrome.
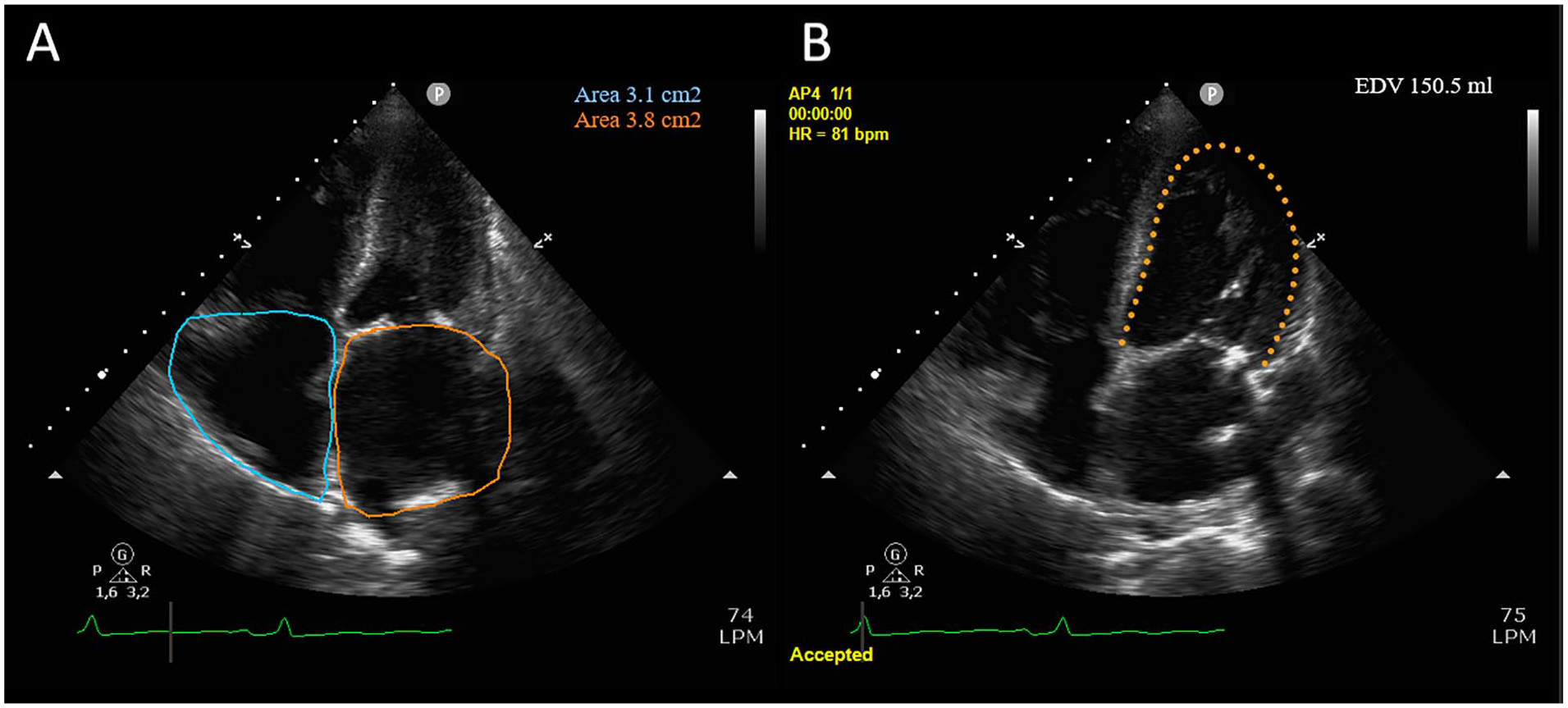
Echocardiography in an apical 4-chamber view showing biatrial enlargement (A) and dilated left ventricle with a end-diastolic volume of 150 mL (B).
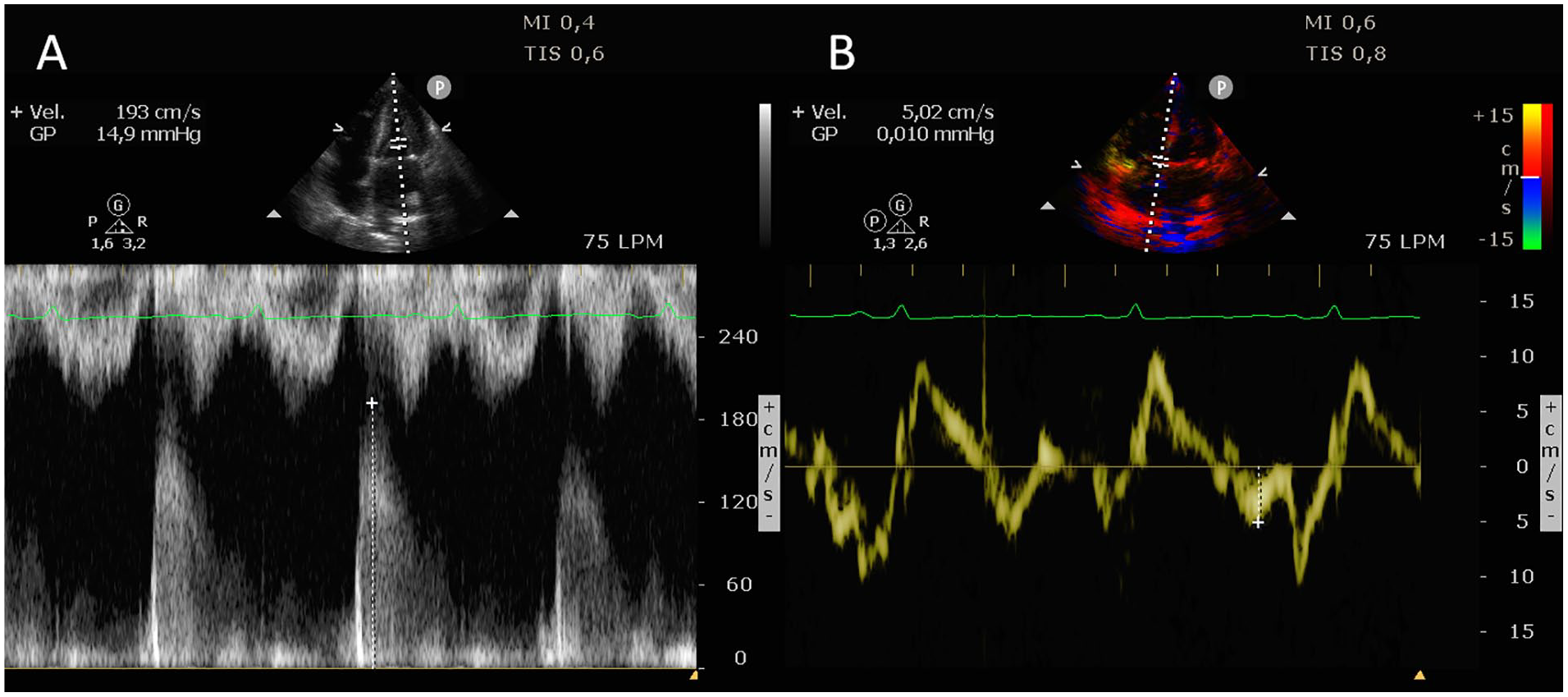
Echocardiography in an apical 4-chamber view measuring the E wave of 193 cm/s (A) and the e′ wave with tissue Doppler of 5 cm/s (B), resulting in a E/e ratio of 38.
An abdominal sonogram was also performed after lab work diagnosed the patient with hyperbilirubinemia. The abdominal sonogram demonstrated the presence of multiple tubular structures within the liver. These tubular structures demonstrated aliasing with color Doppler mode (at a Nyquist limit of 18). Spectral analysis of these vessels demonstrated a low resistive flow pattern and the peak systolic velocity measured 180 cm/s (see Figure 4). The combination of these findings was interpreted as HOHF with a hepatic arteriovenous shunt secondary to HHT. Furosemide, a common diuretic, was administered in order to begin treatment.
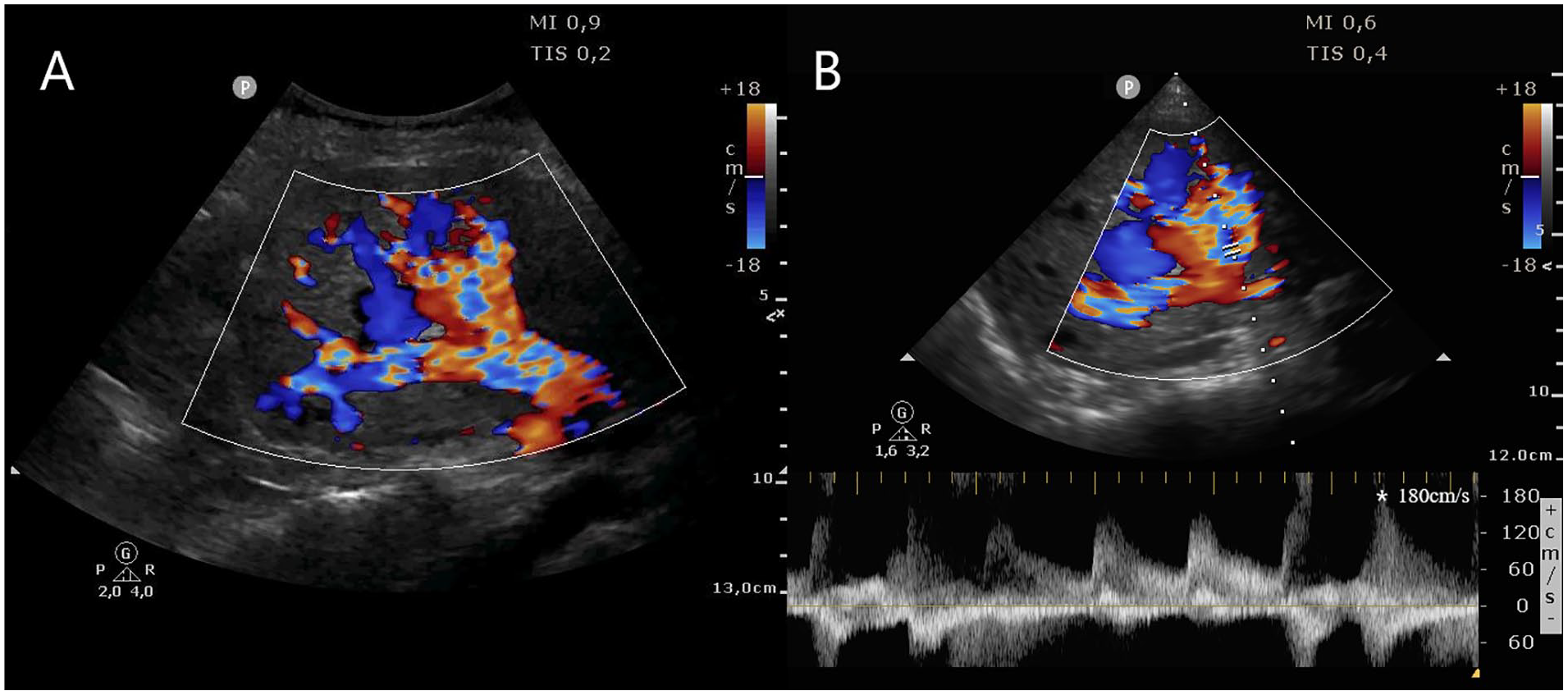
Abdominal sonogram with a coronal view of the liver which showed multiple tubular structures compatible with arteriovenous malformations (AVM) in B and color Doppler mode (A), and in pulsed wave Doppler mode with high-velocity flow and low resistance flow pattern (B).
During the subsequent hospital stay, the patient rapidly progressed to multiorgan failure and died 24 hours later.
Discussion
Liver involvement with HHT is typically diffuse and heterogeneous, or it can be variable, depending on the shunting related to hepatic AVM. Liver telangiectasis are early manifestations that may progress to vascular malformations and shunts. Two major shunt patterns are observed, which lead to different clinical presentations: arteriosystemic (hepatic artery to hepatic vein) and arterioportal (hepatic artery to portal vein). In the presence of an arteriosystemic shunt, the direct communication between the hepatic artery and the hepatic vein causes arterial blood to drain directly into the venous system leading to the right atrium of the heart, generating an increase in the preload and stroke volume of the heart, which can lead to HOHF. The arterioportal shunt pattern leads to presinusoidal portal hypertension as the portal veins are subjected to the high pressures of arterial blood flow. 3
Diagnostic methods include ultrasonography (US), computed tomography, magnetic resonance imaging, and angiography. US is considered the first-line diagnostic tool to detect liver involvement because of its safety and low cost. 5 In grayscale sonography, a hepatic AVM presents as multiple tubular structures with spectral Doppler characteristics of high velocities and low resistive index.3,6 US can also detect manifestations of portal hypertension such as splenomegaly and ascites. If cardiac involvement is suspected, the heart can be evaluated by transthoracic echocardiography, assessing the systolic function in B-mode, mainly by visual estimation of its ejection fraction, and the diastolic function measuring the E wave using the pulsed-wave Doppler at the transmitral flow, and tissue Doppler imaging at the mitral annulus to obtain the E/e′ ratio. Also, the stroke volume can be estimated through the measurement of the left ventricular outflow tract velocity-time integral. 7 In addition, pulmonary edema due to heart failure can be detected with lung ultrasound by the presence of multiple B lines in both hemithoraxes, which is characteristic of alveolar-interstitial syndrome. 8 Supportive care is the primary treatment of this disorder, and early recognition of major organ involvement is fundamental in managing complications. 1 In this patient, POCUS allowed a holistic evaluation in order to achieve the diagnosis of heart failure associated with liver involvement of HHT. Based on a limited review of the literature, this may be the first case in which the use of hepatic, cardiac, and pulmonary ultrasonography for the diagnosis of this pathology has been described.
Conclusion
This case study demonstrates the usefulness of POCUS in diagnosing liver involvement in patients with Osler-Weber-Rendu syndrome and thus allowing the implementation of early treatment.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Approval for this case study was waived in accordance with the local regulations because this study is a case of a single patient and did not include protected health information, data analysis, or testing of a hypothesis, and was de-identified.
Informed Consent
Written consent was obtained from the patient before the publication of this case study.