
Abstract
Objective:
Funic presentation is a risk factor for umbilical cord prolapse. In the majority of cases, umbilical cord prolapse is an obstetric emergency. Currently there is no strategy to prevent umbilical cord prolapse in patients with funic presentation. Placing a third trimester cervical cerclage was proposed, as a mechanical barrier of prolapse, in women with funic presentation.
Materials and Methods:
Twelve patients with funic presentation, detected between 23 and 34 weeks of gestation, were included in the study. Patients were informed that although cervical cerclage have been widely used in obstetrics, it had not been offered in patients with funic presentation. Gestational age at delivery, mode of delivery, location of umbilical cord at birth, presence or absence of umbilical cord prolapsed, and neonatal condition at birth were recorded in all cases.
Results:
Patients’ age varied from 21 to 40 years, mean of 28 ± 6.2 years, and gestational age at the time of diagnosis of funic presentation varied from 26 to 34 weeks of pregnancy. All patients were seen weekly after the cervical cerclage placement to assess the umbilical cord location. Seven patients had vertex presentation, four had breech presentation, and one had transverse lie presentation. A follow-up sonogram of the umbilical cord revealed the following: funic presentation was persistent throughout the entire pregnancy in five patients, disappeared in four, and became intermittent in three. The delivery mode was as follows: cesarean section was performed in eight patients (five with persistent funic presentation, two with intermittent, and one with resolved funic presentation because of failure to progress in labor). There were five patients who delivered vaginally. Funic presentation was confirmed in all patients who underwent cesarean sections. None of the patients had had an umbilical cord prolapse.
Conclusion:
In view of high perinatal mortality of umbilical cord prolapses, placement of cervical cerclage could be added to obstetric armamentarium in patients with funic presentation, after proper counseling.
Umbilical cord prolapse has a prevalence of 1 in 400 births and carries up to 50% risk of perinatal mortality. 1 Funic presentation is a recognized risk factor for umbilical cord prolapse and was detected in 18% of women who later suffered prolapse of the umbilical cord. 2 In the majority of cases, an umbilical cord prolapse is an obstetric emergency and often manifests itself as a category III fetal heart tracing. Category III fetal heart tracing includes minimal variability, bradycardia, and recurrent decelerations, which can result in fetal oxygen deprivation.3,4 Standard treatment of the umbilical cord includes relief of pressure by displacing the presenting part upward, followed by cesarean section. Funic reduction has been reported in a small number of patients, with good outcomes. 5 Funic reduction is a replacement of the umbilical cord back to the uterus by sliding it above the presenting part of the uterus. 5 In one such case, the procedure of funic reduction was undertaken for a funic presentation before rupture of the fetal membranes. 5 The sonographic diagnosis of funic presentation has been reported by several authors, all of whom recommend cesarean section, as a management strategy.1–3
Currently, there is no strategy to prevent umbilical cord prolapse in patients with funic presentation. At present, the treatment for umbilical cord prolapse with a viable fetus is emergency delivery. 6 Delaying delivery for extremely premature fetuses with rupture of membranes has been reported in a few selected cases with a good outcome. 6 In 2000, Petrikovsky et al. 7 proposed a new approach to prevent umbilical cord prolapse in high-risk patients by placing a cervical cerclage as a mechanical obstruction preventing umbilical cord from sliding down. Current guidelines agree that cerclage is indicated in women with a history of spontaneous pregnancy loss or preterm delivery if the cervical length is 25 mm or less. 6 A 2011 meta-analysis that compared cerclage versus no cerclage in women, with a short cervix, showed a decrease in preterm births and a decrease in perinatal mortality and morbidity in the cerclage group. 8 Another systematic review of the literature showed that cervical cerclage placement was associated with an increase in neonatal survival and prolongation of pregnancy, when compared with conservative management. 9 All guidelines agree that cervical cerclage should be removed before the onset of labor, between 36 and 39 weeks of gestation. For women undergoing scheduled cesarean delivery, the American College of Obstetrics and Gynecology (ACOG) and Royal College of Gynecology (RCOG) guidelines recommend that removal of the cervical cerclage may be delayed until this time.6,10–12
Petrikovsky et al. 7 recently reported their experience with using cervical cerclage in patients with persistent funic presentation detected via prenatal sonography. 7 Not a single patient treated with cervical cerclage experienced umbilical cord prolapse. 7 Therefore, the objective was to extend the indications for preventive cervical cerclage to all types of funic presentation.
Materials and Methods
Twelve patients with funic presentation, detected between 26 and 34 weeks of gestation, were included into the study. The imaging protocol was as follows: An initial sonographic examination and weekly follow-up studies were performed by ARDMS credentialed sonographers using a GE Voluson S10 (Waukesha, WI) ultrasound equipment system. Both a curvilinear transabdominal transducer (RAB6RS) and a transvaginal (RIC 5 GARS) transducer were used for performing the sonographic examinations. Funic presentation was detected during routine sonography. The following requirements were applied for the imaging of the umbilical cord presentation to confirm the diagnosis: (1) longitudinal and transverse images of the lower uterine segment, uterine cervix, and presenting part were obtained; (2) if a free loop or loops of umbilical cord below the presenting part were detected, a color Doppler was used to confirm the diagnosis.
All third trimester patients with funic presentation were counseled about the risk of umbilical cord prolapse and the lack of measures to prevent it. Risks and benefits of late cervical cerclage placement were discussed with patients. After counseling, all patients consented to the procedure. All patients signed an informed consent for the placement of cervical cerclage. None of the patients had noteworthy comorbidities or pregnancy complications. Gestational age at delivery, mode of delivery, location of umbilical cord at birth, presence or absence of umbilical cord prolapse, and neonatal condition at birth were recorded in all cases. The technique of the cervical cerclage was as follows: the uterine cervix was grasped at 6 o’clock with ring forceps. Then, a purse-string suture was inserted with bites of the needle deep enough to suture it to the cervical stroma. Four to six bites of the needle were required to encircle the cervix, depending on its thickness. 12 All patients were seen weekly after cervical cerclage placement by sonographers to assess the integrity of the cervical cerclage and umbilical cord location. All procedures were performed in an office setting.
Results
The patients’ age varied from 21 to 40 years, mean of 28 ± 6.2 years, and gestational age at the time of diagnosis of funic presentation varied from 26 to 34 weeks of pregnancy (mean 31 ± 3 weeks). Seven patients had vertex presentation, four had a breech presentation, and one patient had a transverse lie presentation. Follow-up sonograms of the umbilical cord location revealed the following: funic presentation was persistent throughout the entire pregnancy in five patients, resolved in four, and became intermittent in three patients (see Figures 1–3). Delivery mode was as follows: cesarean section was performed in eight patients (five with persistent funic presentation, two patients with intermittent funic presentation, and one with resolved funic presentation due to failure to progress in labor). Five patients had vaginal births. Funic presentation was confirmed in all patients who underwent cesarean sections. None of these patients experienced umbilical cord prolapse. Cervical cerclages were removed prior to the cesarean section in eight patients and at the onset of labor in five. All neonates were born in satisfactory conditions with Apgar scores at 5 minutes between 7 and 10.
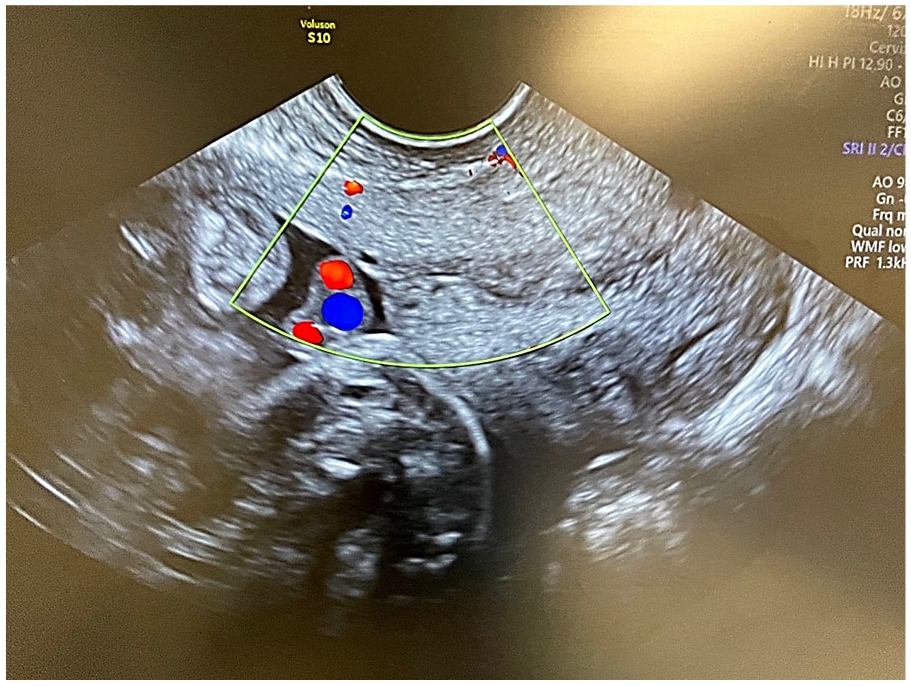
A color Doppler image of a funic presentation. The sonogram also demonstrates a cross-sectional view of the umbilical cord.
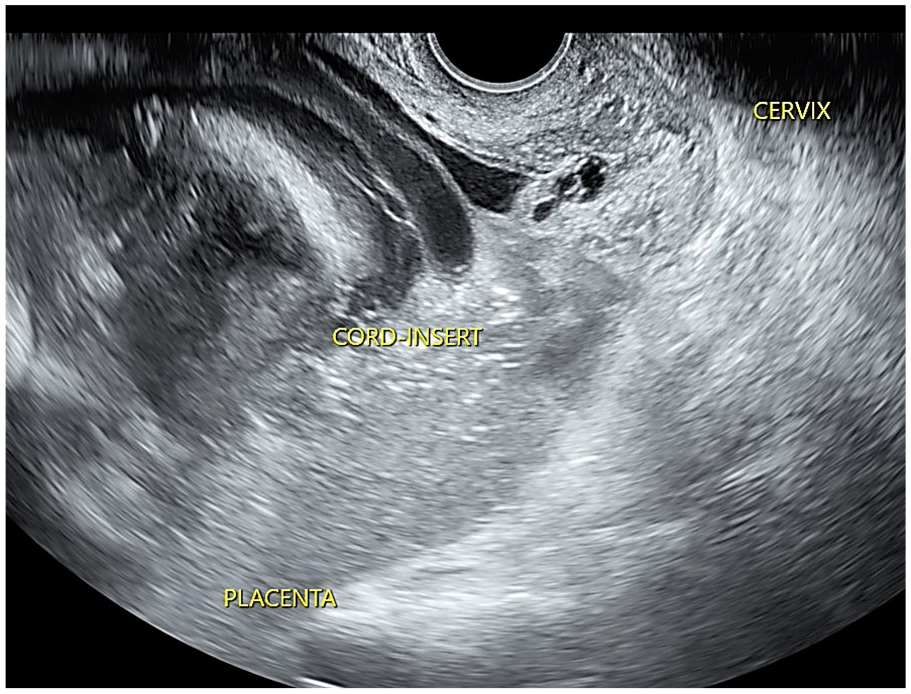
A sonographic transvaginal demonstration of a transient funic presentation. This also provides a sagittal view of the cervix.
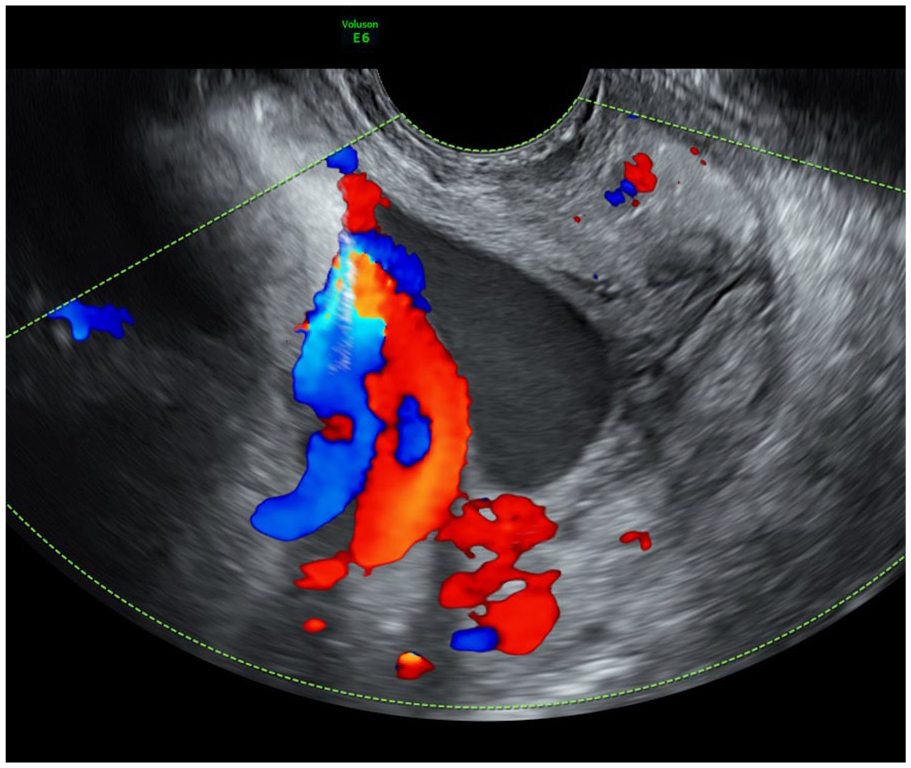
A sonographic transvaginal demonstration of a funic presentation with color Doppler imaging. This also provides a sagittal view of the cervix.
Discussion
Funic presentation, the main risk factor of umbilical cord prolapse is diagnosed when the umbilical cord is located below the presenting part. 5 It may be a transient phenomenon and usually considered clinically insignificant in the second trimester of pregnancy. It becomes concerning if it persists past that date. Ezra et al. 2 reported that relative risk of umbilical cord prolapse in cases of funic presentation is 50 times higher than in ones without funic presentation. Umbilical cord prolapse is diagnosed when the umbilical cord protrudes into the cervix and/or vagina. Umbilical cord prolapse is an obstetric emergency because of the risk of umbilical cord compression, umbilical artery, or vein obstruction, all of which may lead to fetal demise. Most commonly, umbilical cord prolapse presents with an abrupt onset of sustained fetal bradycardia or repetitive, severe variable decelerations in a patient with previous category I tracing. Diagnosis is made based on visualization or palpation of the umbilical cord located in front of the presenting fetal part. Patients are usually informed on the risk of umbilical cord prolapse in cases of funic presentation, which causes extreme maternal anxiety. 8 Current recommendations for management of umbilical cord prolapse include delivery by a cesarean section at 37 to 38 weeks of pregnancy. 8 However, delivery at 37 to 38 weeks does not solve the problem in all cases since the majority of umbilical cord prolapses occur prior to this time.3,4 Recently, Petrikovsky et al. 7 proposed to perform a third trimester cervical cerclage to prevent umbilical cord prolapse in patients with persistent funic presentation defined as a presence of umbilical cord below the presenting part at two consecutive ultrasound examinations at least a week apart. 7 None of these patients developed complications from cervical cerclage placement. 7 None of the patients presented in their original report had developed umbilical cord prolapse after the cervical cerclage placement. 7 Therefore, the objective was to extend the indications for cervical cerclage for all patients with funic presentations (persistent or transient).10–12
Risk factors for umbilical cord prolapse are numerous, and besides funic presentation, include footling breech (15% risk), complete breech (5% risk), and frank breech (0.5% risk), among others. 13 Umbilical cord prolapse has been divided into three types: (1) overt cord prolapsed, (2) funic presentation, and (3) occult prolapse.6,13 With an overt prolapse, the umbilical cord descends through the cervix into the vaginal canal after the rupture of amniotic membranes. Funic presentation is defined as a condition when a loop or loops of the umbilical cord lie between the fetal presenting part and the still-intact fetal membranes. Occult umbilical cord prolapse occurs when the umbilical cord is located alongside the presenting part, but it is not detectable by the examiner. 13 The following conditions are included into the differential diagnosis of funic presentation: marginal insertion of the umbilical cord, vasa previa, and umbilical cord cyst. Marginal cord insertion is a condition when umbilical cord attaches on the side of the placenta instead of the middle of the placenta. It occurs in 9% of all pregnancies. 14 Velamentous cord insertion is a condition when the umbilical cord comes out of fetal membranes. Vasa previa is defined as unprotected umbilical blood vessels, which run through the amniotic membranes in the vicinity of the cervix. Vasa previa is detected in 2500 births and puts the fetus at risk of bleeding. 14 Color Doppler imaging helps in making the diagnosis. In funic presentation, the entire loops of the umbilical cord are seen while in vasa previa, only the blood vessels are seen. Two types of vasa previa have been reported. 15 Type I is when there is a velamentous insertion of the umbilical cord and fetal vessels run freely within amniotic membranes overlying the uterine cervix. Type II is when the placenta has a succenturiate lobe or is multilobed and fetal vessels run between two placental lobes. When the amniotic membranes rupture, it results in fetal hemorrhage. Major risk factors for vasa previa are velamentous cord insertion and multilobed placenta. 16 Vasa previa should be suspected in case of vaginal bleeding combined with category III fetal heart rate tracing. 15 Umbilical cord cysts are fluid-filled structures located within the umbilical cord itself. Unlike funic presentation, umbilical cord cysts do not contain blood vessels. 15
Limitations
The limitation of this study was the relatively small number of participants. The obvious explanation for this limitation is low prevalence of funic presentation. The strength of the study was the introduction of a new indication for cervical cerclage to prevent umbilical cord from prolapsing. In view of high perinatal morbidity and mortality of umbilical cord prolapse, placement of cervical cerclage after proper counseling should be added to obstetric armamentarium in patients with funic presentation. A search for umbilical cord loops below the presenting part should be a part of a third trimester sonographic examination. More research is needed to clarify the role of associated conditions (polyhydramnios, multifetal pregnancies, among others), which may lead to funic presentation and ultimately, an umbilical cord prolapse. More research data may justify an American Institute of Ultrasound In Medicine (AIUM) recommendation to include search for funic presentation as a routine part of third trimester sonographic examination. Although this study has a limited number of participants because of the rarity of funic presentation, the fact that no participant experienced umbilical cord prolapse or complications from cervical cerclage is very promising.
Conclusion
Cervical cerclage represents the first attempt to prevent umbilical cord prolapsing in patients with high-risk factors. Until now, the investigators concentrated their efforts on the management of umbilical cord prolapse once it already occurred. This manuscript addresses the issue of preventing the prolapse of the umbilical cord in patients with identifiable risk factors, for example, funic presentation. Cervical cerclage provides a mechanical barrier preventing the umbilical cord from sliding down the cervical canal. The current study, with limited number of patients, demonstrated the efficacy and safety of this approach. None of these patients experienced umbilical cord prolapse or complications from cervical cerclage. Future studies should address the usefulness of cervical cerclage in other conditions, for example, unstable lie, which may also lead to umbilical cord prolapse.
Footnotes
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because cervical cerclage is an accepted surgical procedure during pregnancy.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the study.
Trial Registration
Not applicable.