
Abstract
Purpose
To explore the association between the timing of cervical cerclage placement and postoperative outcomes.
Methods
We retrospectively analyzed postoperative outcomes in pregnant women who underwent cervical cerclage at our hospital between January 2020 and December 2023. Participants were divided into nonterm and term birth groups.
Results
Compared with the term birth group, the nonterm birth group had significantly shorter cervical length (10.02 ± 8.17 vs. 23.40 ± 10.93 mm; p < 0.001), wider cervical orifice width (7.50 ± 10.71 vs. 1.12 ± 4.79 mm; p < 0.001), longer duration of postoperative hospitalization (29.53 ± 22.76 vs. 18.12 ± 21.26 days; p < 0.001), longer administration period of tocolytics (28.13 ± 22.26 vs. 16.15 ± 21.30 days; p < 0.001), lower neonatal birth age (33.07 ± 3.27 vs. 38.32 ± 0.95 weeks; p < 0.001), lower neonatal birth weight (2081.40 ± 641.36 vs. 3266.30 ± 352.76 g; p < 0.001), and lower Apgar score at 1 minute (10 (3–10) vs. 10 (3–10); p < 0.001). Cervical length showed higher sensitivity in determining the timing of cervical cerclage placement (area under the receiver operating characteristic curve: 0.830 vs. 0.669), with a cutoff value of 17 mm (sensitivity: 83.33%, specificity: 71.43%).
Conclusion
Cervical cerclage may be beneficial in asymptomatic pregnancies where the cervical length is ≤17 mm or the cervix is undilated.
Introduction
The World Health Organization defines preterm birth (PTB) as the delivery of a baby before completing 37 weeks of gestation. 1 PTB constitutes a significant public health concern, exerting detrimental impacts on the lives of approximately 15 million infants, mothers, and families globally. 2 Annually, approximately 1 million neonatal deaths are attributed to adverse events resulting from prematurity. 3 The etiology of PTB is considered to be multifactorial, involving obstetric, environmental, demographic, and genetic factors, which may contribute individually or interactively to the pathophysiological process. 4 Cervical insufficiency is one of the causes of PTB and is associated with PTB, neonatal morbidity, and mortality. 5 It is defined as the inability of the cervix to maintain a pregnancy in the absence of uterine contractions. 6 The incidence of cervical insufficiency in pregnancies is estimated to range from 0.5% to 1%, and the risk of recurrence can reach 30%. 7 Cervical insufficiency is considered to be a structural deficiency, 6 characterized by cervical softening that results in an inability to maintain the structural integrity of the cervix. The processes of cervical softening in women with cervical insufficiency are intricately linked to cervical shortening and dilatation, ultimately leading to the occurrence of PTB.8,9 Cervical insufficiency is an independent risk factor for PTB. 10 Cervical cerclage placement is a surgical intervention employed to mechanically prevent PTB; this procedure has demonstrated efficacy in enhancing neonatal morbidity and mortality outcomes. 11 The Green-top Guideline No. 75 12 recommends the use of gestational week as the sole criterion for history-indicated cerclage, without considering the cervical condition. Cervical length (CL) is one of the parameters utilized in ultrasound-indicated cerclage. A short cervix, defined as a CL <2.5 cm measured by ultrasound during mid-pregnancy, is correlated with an elevated risk of spontaneous PTB. 13 A previous study 14 established a significant association between a short CL (<2.5 cm) on ultrasound and spontaneous PTB. However, cerclage placement may not always confer benefits to pregnant women with a CL <2.5 cm on ultrasound. Despite the implementation of cerclage placement in women with cervical insufficiency, they remain at elevated risk of PTB. 15 According to the Green-top Guideline No. 75, cervical cerclage is recommended exclusively for pregnant women with a history of PTB and a short cervix. 12 However, no specific recommendations have been established for pregnant women with a short cervix but no history of PTB. Only a few relevant studies have been conducted, providing insufficient evidence. Striking a balance between optimizing the benefits for pregnant women with cervical insufficiency and mitigating the adverse consequences of cervical cerclage is imperative. This study aimed to identify a correlation between the timing of cervical cerclage placement and postoperative outcomes. The optimal timing of cervical cerclage placement was confirmed to provide benefits for pregnant women with cervical insufficiency.
Materials and methods
Reporting method
We adhered to the relevant Cervical Cerclage Green-top Guideline No. 75 while conducting this study. This guideline was published by the Royal College of Obstetricians & Gynaecologists in February 2022. The reporting of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 16
Study design and population
We used PASS, version 21 (NCSS, LLC, Kaysville, Utah, USA), to calculate the sample size. We anticipated a sample size of 16 cases when the area under the receiver operating characteristic (ROC) curve (AUC) was 0.90.
This retrospective study included pregnant women with cervical insufficiency who underwent cervical cerclage and delivered at our hospital from January 2020 to December 2023. The inclusion criteria were as follows: (a) singleton pregnancies between 12+0/7 and 27+6/7 weeks of gestation; (b) pregnant women with a history of miscarriage in the second trimester or painless cervical shortening or dilatation; and (c) pregnant women with a CL <25 mm before 24 weeks of gestation. The exclusion criteria were vaginal bleeding, threatened PTB, preterm premature rupture of membranes, fetal congenital malformations or aneuploidy, and maternal pre-existing medical conditions that can influence the prognosis of pregnancy. Participants were categorized into two groups, namely, term birth group and nonterm birth group, based on their gestational age at delivery. The present study was conducted in accordance with the Declaration of Helsinki (2000) of the World Medical Association and approved by the Medical Ethics Review Committee of our Hospital (202402128). The ethics committee agreed to waive the requirement for written informed consent due to the retrospective nature of the study. All patient details have been de-identified.
Data collection
The timing of cervical cerclage placement was assessed using two parameters: CL and cervical orifice width (COW). Parameters for postoperative outcomes included duration of postoperative hospitalization (DOPH), administration period of tocolytics (APOT), neonatal birth age (NBA), neonatal birth weight (NBW), and Apgar score at 1 minute.
The following maternal variables were recorded: age, weight, gravidity, parity, gestational week at operation, delivery gestational age, CL at operation, COW at operation, exposed fetal membranes at operation, DOPH, and APOT. Clinical data of neonates including live births, stillbirths, NBA, NBW, and Apgar score at 1 minute were collected.
Cervical measurement and cerclage
Ultrasound examinations were conducted using an Aixplorer ultrasound machine (SuperSonic Imagine, SA) with a 3–5 MHz convex array probe. CL was measured via transperineal ultrasound by placing a probe on the perineal body. The shortest measurement was recorded when dynamic cervical changes were observed. COW was measured through vaginal speculum examination. Shirodkar cervical cerclage was performed for all patients.
Statistical analyses
Statistical analyses were conducted using SPSS version 27 (IBM Corp., Armonk, NY, USA). Categorical variables were expressed as percentages (%), while continuous variables were presented as mean ± SD or median (range). Data conforming to a normal distribution were analyzed using a t-test, whereas data with a skewed distribution were analyzed using the Mann–Whitney test. Chi-square test was used for analyzing categorical variables. Spearman analysis was performed to analyze the relationship between the parameters of the timing of cervical cerclage placement and postoperative outcomes. Regression analysis was conducted to assess the relationship between the parameters of the timing of cervical cerclage placement and postoperative outcomes, determining the independent association of variables with postoperative outcomes. The diagnostic accuracy of the timing of cervical cerclage placement for postoperative outcomes was expressed as the AUC. Sensitivity, specificity, and predictive values of the parameters were determined using ROC curves, with the cutoff value calculated based on the Youden index. All statistical tests were two-tailed, and a p-value less than 0.05 was considered to indicate statistical significance.
Results
In total, 198 pregnant women with cervical insufficiency who underwent cerclage at our hospital were enrolled in the study, among whom 188 delivered their baby at our hospital. The participants were categorized into two groups: nonterm birth group and term birth group, based on their gestational age at delivery. Overall, 90 women were included in the nonterm birth group and 98 in the term birth group. Figure 1 illustrates the flowchart of pregnant women with cervical insufficiency included in the study. The pregnant women in the nonterm birth group delivered 90 preterm live neonates, whereas those in the term birth group delivered 98 term live neonates.
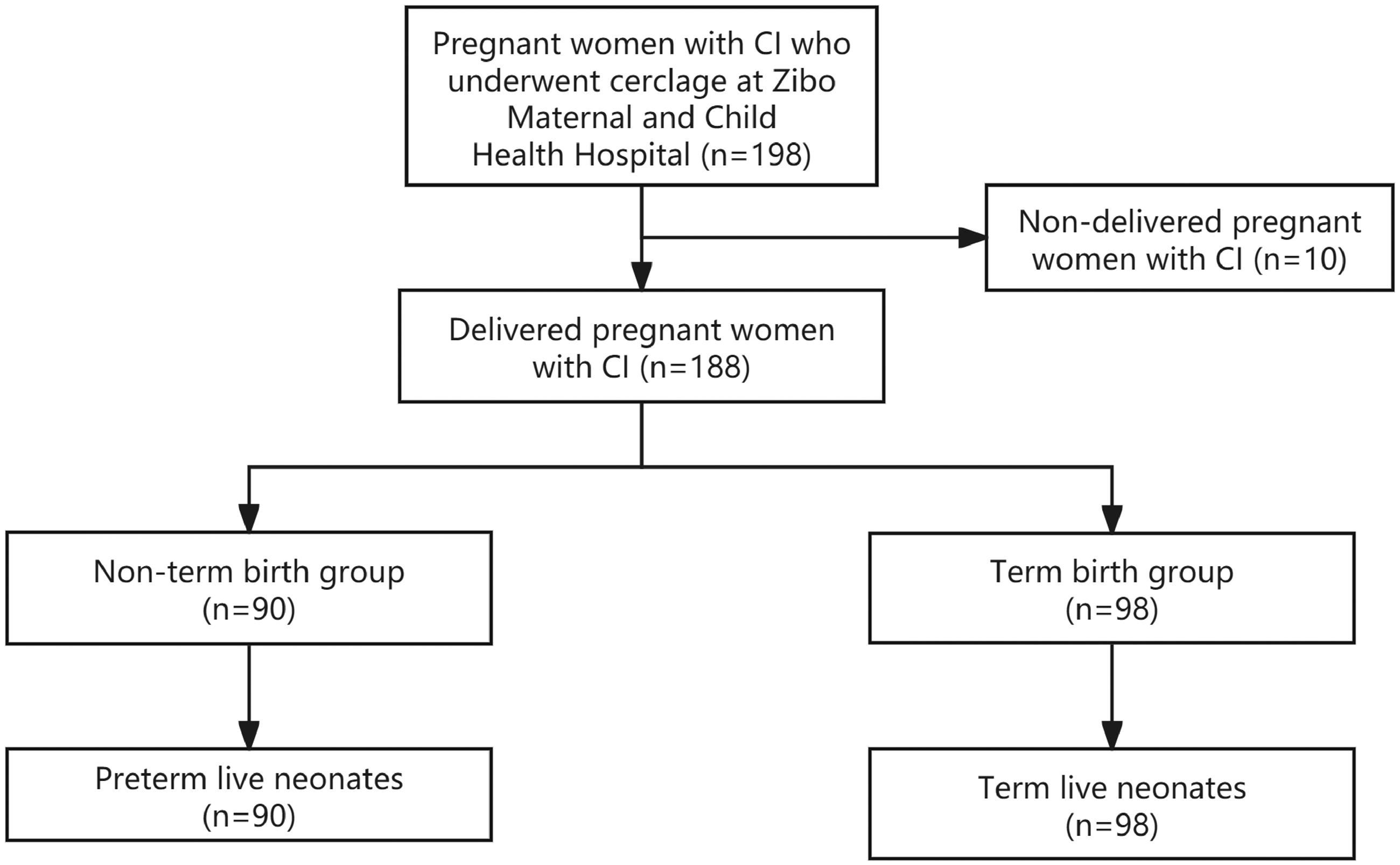
Flowchart of pregnant women with cervical insufficiency included in the study.
A comparison of the two groups is presented in Table 1. The gestational age at operation in the nonterm birth group was significantly higher than that in the term birth group (22.49 ± 3.64 vs. 18.48 ± 4.69 weeks; p < 0.001), while the gestational age at delivery was significantly lower in the nonterm birth group (31.90 ± 4.69 vs. 38.34 ± 0.95 weeks; p < 0.001). Regarding the parameters of timing of cervical cerclage placement, the CL at operation in the nonterm birth group was significantly shorter than that in the term birth group (10.02 ± 8.17 vs. 23.40 ± 10.93 mm; p < 0.001), and the COW at operation was significantly wider in the nonterm birth group (7.50 ± 10.71 vs. 1.12 ± 4.79 mm; p < 0.001). The number of pregnant women with exposed fetal membranes at operation in the nonterm birth group was significantly higher than that in the term birth group (36 vs. 6; p < 0.001). Postoperative outcomes were also compared between the two groups. In the nonterm birth group, the DOPH (29.53 ± 22.76 vs. 18.12 ± 21.26 days; p < 0.001) and APOT (28.13 ± 22.26 vs. 16.15 ± 21.30 days; p < 0.001) significantly exceeded those in the term birth group. NBA in the nonterm birth group was significantly lower than that in the term birth group (33.07 ± 3.27 vs. 38.32 ± 0.95 weeks; p < 0.001). Additionally, in the nonterm birth group, the NBW (2081.40 ± 641.36 vs. 3266.30 ± 352.76 g; p < 0.001) and Apgar score at 1 minute (10 (3–10) vs. 10 (3–10); p < 0.001) were lower than those in the term birth group.
Comparison of the characteristics of mothers and neonates.

As shown in Table 2, the CL at operation was negatively correlated with DOPH (R = −0.530, p < 0.001) and APOT (R = −0.570, p < 0.001), whereas it was positively correlated with NBA (R = 0.596, p < 0.001), NBW (R = 0.581, p < 0.001), and Apgar score at 1 minute (R = 0.300 p < 0.001). The COW at operation was positively correlated with DOPH (R = 0.354, p < 0.001) and APOT (R = 0.387, p < 0.001), whereas it was negatively correlated with NBA (R = −0.436, p < 0.001), NBW (R = −0.407, p < 0.001), and Apgar score at 1 minute (R = −0.332, p < 0.001).
Correlation analysis of the parameters of the timing of cervical cerclage placement and postoperative outcomes.
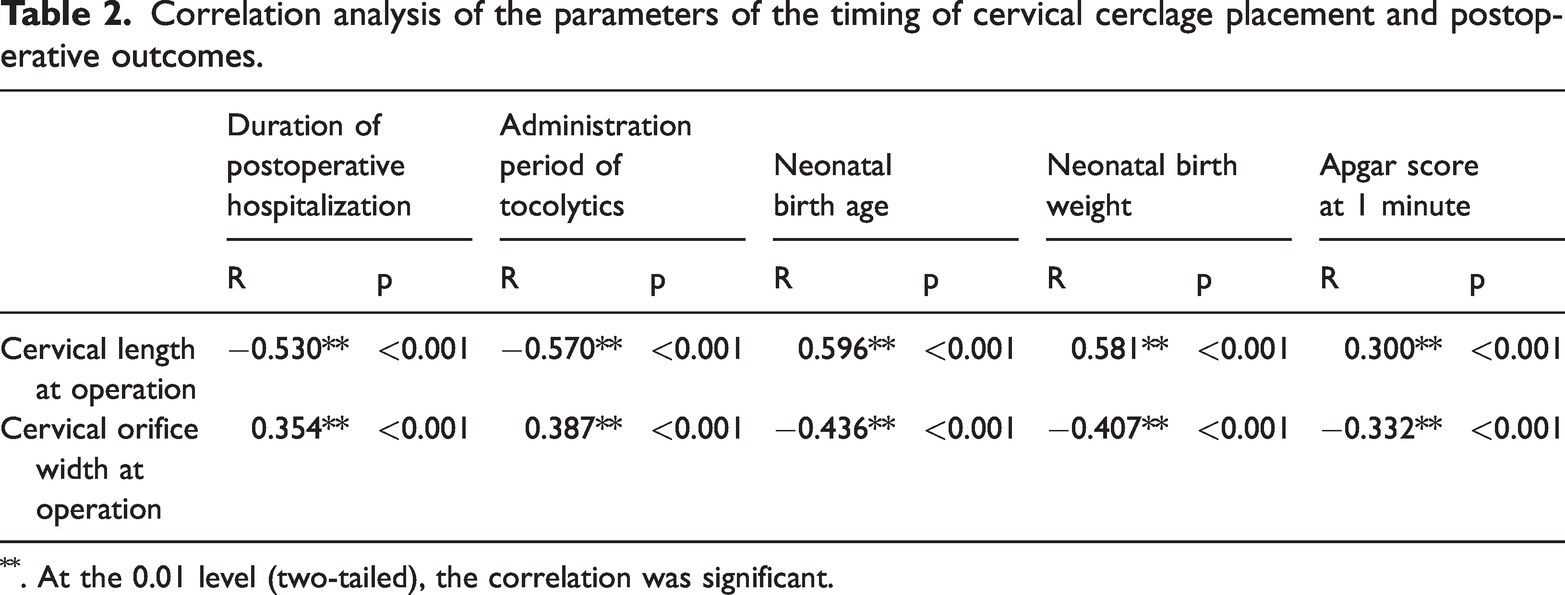
. At the 0.01 level (two-tailed), the correlation was significant.
The results of logistic regression analysis, as shown in Table 3, demonstrate the association between the parameters of the timing of cervical cerclage placement and postoperative outcomes. The CL at operation was significantly associated with extended DOPH (p < 0.001, 95% confidence interval (CI): −1.065 to −0.560) and APOT (p < 0.001, 95% CI: −1.084 to −0.586). Additionally, the CL at operation was significantly associated with extended NBA (p < 0.001, 95% CI: 0.123 to 0.196), increased NBW (p < 0.001, 95% CI: 29.833 to 45.419), and a higher Apgar score at 1 minute (p < 0.001, 95% CI: 0.013 to 0.046). The COW at operation was significantly associated with extended DOPH (p = 0.003, 95% CI: 0.197 to 0.928) and APOT (p < 0.001, 95% CI: 0.259 to 0.981). Furthermore, the COW at operation was significantly associated with reductions in NBA (p < 0.001, 95% CI: −0.239 to −0.139), NBW (p < 0.001, 95% CI: −48.613 to −25.980), and Apgar score at 1 minute (p < 0.001, 95% CI: −0.075 to −0.032).
Logistic regression analysis of the parameters of the timing of cervical cerclage and postoperative outcomes.

ROC curves were generated to determine the optimal timing of cervical cerclage placement based on the CL and COW at operation. The results are presented in Table 4 and Figure S1. For CL at operation, the AUC was 0.830 (95% CI: 0.769 to 0.881), with a sensitivity of 83.33% and specificity of 71.43%. The COW at operation had an AUC of 0.669 (95% CI: 0.597 to 0.736), sensitivity of 40.00%, and specificity of 93.88%. ROC curve analysis demonstrated that the timing of cervical cerclage placement was significantly associated with the CL at operation (p < 0.0001). However, the timing of cervical cerclage placement was not significantly associated with the COW at operation (p < 0.0001). The cutoff value for CL at operation, as determined using the Youden method, was 17 mm.
ROC analysis of the parameters of the timing of cervical cerclage.

ROC: receiver operating characteristic; AUC: area under the receiver operating characteristic curve.
Discussion
The results of this study demonstrate that the CL at operation was negatively correlated with DOPH and APOT and was positively correlated with NBA, NBW, and Apgar score at 1 minute. Additionally, the CL at operation was shorter in the nonterm birth group than in the term birth group, with longer DOPH and APOT being observed in the nonterm birth group. In addition, the COW at operation was positively correlated with DOPH and APOT but negatively correlated with NBA, NBW, and Apgar score at 1 minute. The COW at operation was wider in the nonterm birth group than in the term birth group. Pregnant women with exposed fetal membranes at operation were more likely to experience preterm labor.
This study determined the optimal timing of cervical cerclage placement through ROC curve analysis. The CL at operation was identified as a sensitive parameter for determining the optimal timing of cervical cerclage placement, while the COW at operation lacked such sensitivity. We suggested that cervical cerclage provides the greatest benefits to pregnant women with cervical insufficiency when the cutoff for CL is 17 mm.
Cervical cerclage emerges as the primary intervention in pregnancies with identifiable risk factors for PTB, consistently demonstrating efficacy in PTB prevention. 17 A shortened CL observed during ultrasound examination is correlated with an elevated risk of PTB. 18 Ultrasound-indicated cerclage is currently recommended for patients presenting with a short CL and a history of PTB. 19 Furthermore, observational studies and systematic reviews have reported a favorable role of cervical cerclage in pregnancies with an extremely short cervix (<10 mm), as measured using ultrasonography. 20 However, the efficacy of cerclage in reducing the risk of PTB may not be consistent across patients with a short cervix of varying lengths. The study showed that the CL in the nonterm birth group was shorter than that in the term birth group. A shorter cervix indicates a higher risk of PTB. Therefore, relevant interventions, such as cervical cerclage, should be performed assertively when the cervix exhibits a reduction in length rather than waiting until the CL is <10 mm.
In addition, relevant studies have previously demonstrated associations between a wider endocervical canal and cervical insufficiency. 21 Chen et al. also demonstrated a wider endocervical canal in women with cervical insufficiency during the first trimester. 22 In our study, the COW was not a sensitive parameter for determining the timing of cervical cerclage placement. Dilation of the cervical orifice occurs when the cervix is shortened until it disappears. Ocal et al. believed that when cervical cerclage is performed in pregnant women with prolapsed fetal membranes, it can prolong the interval between diagnosis and delivery, improve neonatal survival rates, and increase the likelihood of deliveries occurring after 28 weeks of gestation. 23 In our study, the proportion of exposed fetal membranes at operation in the nonterm birth group was higher than that in the term birth group. Therefore, cervical cerclage should be performed before the cervical orifice dilation progresses to the point where the fetal membranes are exposed.
The implementation of cerclage effectively prolongs gestation and enhances pregnancy outcomes. 23 Berghella et al. 24 first reported cerclage as an effective treatment option for women with singleton pregnancies and a short CL (<25 mm), reducing the risk of PTB before 35 weeks of gestation, regardless of a history of PTB. D'Antonio et al. 25 believed that performing emergency cerclage in women with cervical dilation or a short CL (<15 mm) may help lower the PTB rates and improve perinatal outcomes. We determined the optimal cutoff value for CL to be 17 mm based on ROC curve analysis. Therefore, we believed that cervical cerclage confers the greatest benefits to pregnant women with cervical insufficiency when the CL was ≤17 mm or the cervix was undilated. These benefits encompass diminished rates of PTB, enhanced pregnancy outcomes, shortened DOPH, and reduced APOT.
Our study had certain limitations. The sample size was relatively small, and data were collected from a single center, limiting the generalizability of the findings. The relatively small sample size also resulted in excessively wide ranges of two CI estimates. CL analysis should be conducted for twin pregnancies. Paredes et al. 26 argued that most of the existing literature emphasizes on pregnancy outcomes, whereas a relatively fewer studies have addressed the prevention of complications associated with Mersilene tape erosion. Our research exclusively focused on the timing of cervical cerclage placement and its effects on pregnancy outcomes; however, we did not address the complications related to the procedure.
Conclusion
Cervical cerclage may provide benefits to women with asymptomatic pregnancies who had a CL ≤17 mm or an undilated cervix. These benefits encompass diminished rates of PTB, enhanced pregnancy outcomes, shorter DOPH, and reduced APOT.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251367409 - Supplemental material for Association between the timing of cervical cerclage placement and postoperative outcomes: A retrospective study
Supplemental material, sj-pdf-1-imr-10.1177_03000605251367409 for Association between the timing of cervical cerclage placement and postoperative outcomes: A retrospective study by Lirong Zhao, Xueli Dai, Xu Chen and Yingchun Yu in Journal of International Medical Research
Footnotes
Acknowledgements
Not applicable.
Author contributions
Lirong Zhao contributed to the study design, performed statistical analysis, and drafted the manuscript. Xueli Dai and Xu Chen participated in data acquisition and analysis. Yingchun Yu contributed to the study design and performed statistical analysis. All authors have read and approved the final manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this manuscript.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The study was approved by the Medical Ethics Review Committee of Zibo Maternal and Child Health Hospital. The requirement for informed consent was waived by the Medical Ethics Review Committee of Zibo Maternal and Child Health Hospital because of the retrospective nature of the study.
Funding
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.