
Abstract
Objective:
To investigate the role of the uterine endometrial thickness and sonographic pattern as potential predictors for a pregnancy with an unknown location (PUL) and its possible outcomes.
Materials and Methods:
A convenient sample of 330 symptomatic extra preposition female patients were enrolled in this study with a diagnosis of PUL. The clinical variables of endometrial stripe thickness and endometrial sonographic pattern were determined with transvaginal sonography. These sonographic examinations (it seems that examination in this context is a countable noun) were conducted during the first 24 hours of referral, and their predictive values for PUL outcomes (normal intrauterine pregnancy (IUP), ectopic pregnancy (EP), and pregnancy loss) were assessed after clinical follow-up sessions provided a definite outcome. The statistical significance was set a priori at a P value < .05.
Results:
The mean initial endometrial stripe thickness among participants, with a normal IUP, was more than those patients with an abnormal pregnancy outcome (P < .05). The optimum cut-off value for predicting a an EP, compared to a normal IUP was 11 mm and had a sensitivity of 73.3% and specificity of 39% (P < .001). These results also demonstrated no statistically significant relationship between the PUL outcome and the categories of endometrial sonographic pattern (P = .15).
Conclusion:
In this large cohort of patients, the endometrial stripe thickness of more than 11 mm, among those who were symptomatic and deemed as PUL, had the potential to predict ectopic pregnancy as an unlikely diagnosis.
Key Takeaways
Among symptomatic women experiencing PUL:
Initial endometrial stripe thickness was significantly lower in those experiencing EP or early pregnancy failure compared to those who had normal IUP.
Endometrial stripe thickness of more than 11 mm measured by TVS during 24 hours of referral could make an ectopic pregnancy an unlikely diagnosis.
Endometrial sonographic pattern assessed by TVS during 24 hours of referral, showed no significant relationship with the PUL outcome.
The reduction of maternal mortality continues to be an important health issue in human society and has become a target within the United Nations’ Millennium Development Goal (MDG) framework. 1 An ectopic pregnancy (EP) is a gynecologic emergency and is defined by the implantation of a fertilized ovum out of the uterine cavity, mostly inside the fallopian tubes. 2 This condition is sometimes suspected in the context of a medical condition termed as a pregnancy with an unknown location (PUL). This is denoted as a condition that occurs when a gestational sac is not seen during transvaginal sonography (TVS) within the uterus, fallopian tubes, or abdominal cavity. This is accompanied with a patient experiencing a delayed or missed menstrual cycle and a positive qualitative serum human chorionic gonadotropin (β-hCG) test. 3
According to the World Health Organization, an EP accounts for 4.9% of all maternal mortalities. 4 It is a relatively prevalent complication of pregnancy, with varying incidence worldwide; though, estimations show that 1% to 2% of all pregnancies are ectopic, accounting for 0.48 maternal deaths per 100,000 live births. 5 Although the 2% prevalence rate may seem low, rises to 6% to 16% among women presenting to an emergency department with first-trimester vaginal bleeding, lower abdominal pain, or a combination of both. 6 Several risk factors have been described for EP some of which include: fallopian tube damage as a result of previous surgery or infection, smoking, older maternal age, and assisted reproduction techniques. 7
The estimated EP prevalence increased four-fold (from 0.5% to 2%) in the United States between the years 1970 and 2013, partly as a result of faster, easier, and more accurate methods of diagnosis. 6 Primary symptoms like lower abdominal pain or vaginal bleeding in women presenting with delayed or missed menstrual cycle, as most common symptoms of EP, should be taken seriously and need further workup. 2 Today, the serial serum β-hCG level checks, in conjunction with TVS, has become the preferred diagnostic method to assess EP among symptomatic pregnant women. 7 With the help of these para-clinical evaluations, an earlier and easier detection of EP has been achieved, and as nonsurgical treatment methods became more effective, concomitant maternal mortality rates have decreased worldwide. 8
An early sonographic finding of an ectopic pregnancy is widely explained within the literature; 9 however, evidence is still needed for those patients with clinical symptoms, suggestive of early pregnancy failure or ectopic pregnancy, with no extra or inrtauterine pregnancy (IUP) that can be visualized by TVS. As mentioned earlier, this condition can be classified as PUL, based on 3 clinical situations, which include an IUP, early pregnancy failure, or EP that is documented. 3
The decidual reaction during pregnancy results in the sonographic appearance of echogenic endometrium. As the decidual reaction and resultant endometrium thicken, due to elevated serum β-hCG levels, a thin endometrial stripe thickness may predict inappropriately low serum β-hCG levels and abnormal pregnancy outcomes, at an early onset. This is why some studies have focused on the role of endometrial stripe thickness and sonographic endometrial pattern, as predictors of an outcome with a PUL.10–16
This study aimed to investigate whether an endometrial stripe thickness during the initial sonographic evaluation of pregnancy, could predict the outcome of PUL and to determine the best cut-off point for initial endometrial stripe thickness, as a predictor of ectopic pregnancy. In addition, any association between ectopic pregnancy and sonographic endometrial patterns were assessed.
Materials and Methods
Patient Selection and Study Design
This prospective study was conducted between August 2019 and August 2020 and was approved by the Ethics Board of the Radiology department. Patients who were referred to the host tertiary care centers and had a positive quantitative serum β-hCG test were invited to the study. In addition, the patients had to fulfill the following inclusion criteria: (1) abdominal pain or vaginal bleeding, (2) no visible gestational sac, adnexal masses, and intraperitoneal free fluid, on the sonogram, performed during first 24 hours of referral. The exclusion criteria of being hemodynamically unstable was used. For those patients that formed the convenient sample, written informed consent was obtained. Demographic data were collected for each consented patient.
Clinical Management
All participants were checked with serial quantitative serum β-hCG levels and a TVS every 48 hours. These diagnostic tests continued until a definite diagnosis of IUP, ectopic pregnancy, or early pregnancy failure was established. 17 Finally, for those student patients with completed diagnostics, they were categorized into the following 3 groups:
IUP.
EP.
Early pregnancy failure.
Sonographic Examinations
All the patients underwent TVS. A GE Voluson Expert 730 ultrasound equipment system (GE Electric Medical System, Milwaukee, WI, USA) was used with a transvaginal transducer of 6.5 to 8 MHz. All these specific examinations were conducted by a radiologist with greater than 10 years of experience in obstetric sonography. Any challenging case was resolved by a senior radiologist with 25 years of experience in obstetrics and gynecology sonography.
The endometrial stripe thickness was measured for each patient. An endometrial sonographic pattern was also noted. The endometrial stripe thickness was measured in the mid-sagittal plane, perpendicular to the endometrium longitudinal axis, at its thickest part. The endometrial sonographic pattern was divided into either a hyperechoic monolayer or a trilaminar pattern (see Figure 1A and 1B).
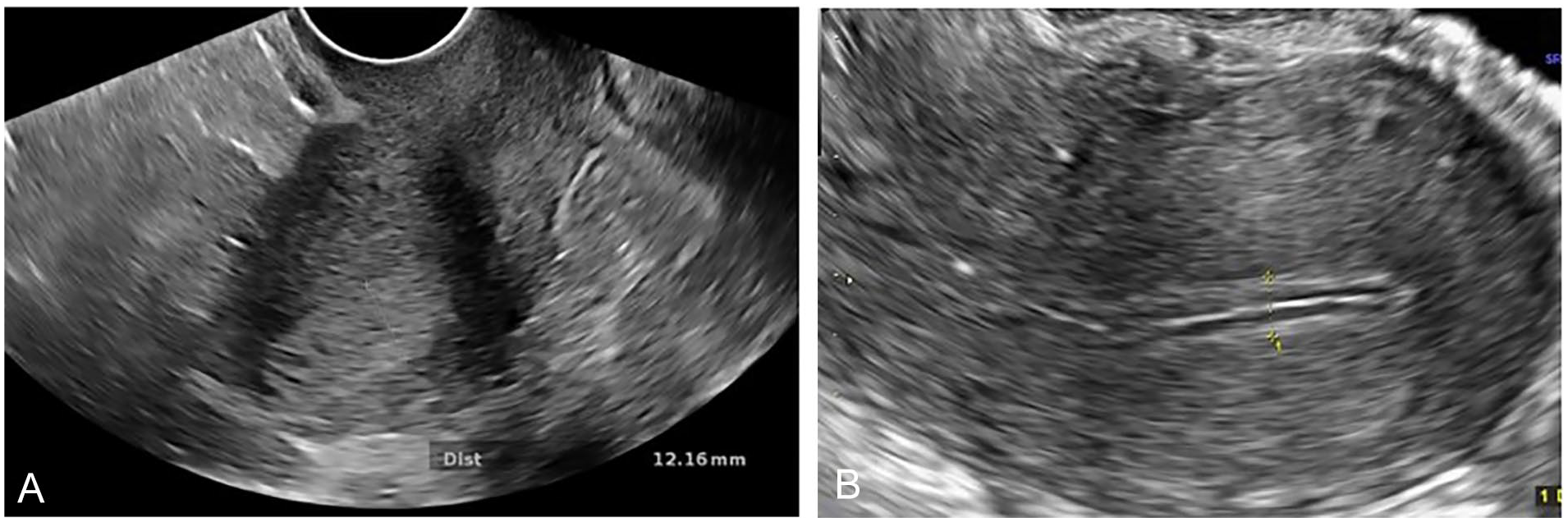
(A) Transvaginal sonogram in a 20-year-old woman with the final diagnosis of intrauterine pregnancy shows hyperechoic monolayer pattern of endometrial layer. (B) Transvaginal sonogram in a 25-year-old woman finally diagnosed as ectopic pregnancy, shows trilaminar pattern of the endometrial stripe.
Statistical Analysis
The final collected data were entered into SPSS 25 (Chicago, SPSS Inc.). All quantitative data were reported as mean ± standard deviation (SD), and the qualitative ones were reported as percentages and counts. A 1-way analysis of variances (ANOVA) test was used to determine if endometrial thickness had significant difference among the following 3 patient groups: (1) women with normal IUP, (2) patients suffering an ectopic pregnancy, and (3) patients suffering an early intrauterine failure. The receiver operating curve (ROC) was used to determine the best cut-off value for endometrial thickness in millimeters (mm), which can predict normal IUP rather than EP. To conclude the possible predictive value of an endometrial sonographic pattern, for early diagnosis of EP, a κ2-test and a Fisher’s exact test were used. The statistical significance for this study was established a priori at a P value < .05.
Results
Three hundred and thirty women, with a mean age of 32.8 ± 5.1 years, were included in this study. The participants had a minimum and maximum age of 22 and 47 years, respectively. There were 186 (56.4%) cases of IUP, 102 (30.9%) cases of EP, and 42 (12.7%) cases of an early pregnancy failure. The mean endometrial stripe thickness in all participants was 12.7 ± 5.07mm. Three-hundred and seventeen (96.1%) patients had hyperechoic monolayer endometrial pattern, and 13 (3.9%) had a trilaminar endometrial pattern.
Table 1 shows the mean endometrial stripe thickness and the different types of pregnancy outcomes. Table 2 is provided and illustrates the distribution of endometrial sonographic patterns and varied types of pregnancy outcomes.
The Mean Endometrial Thickness Given Different Types of Pregnancy Outcomes.
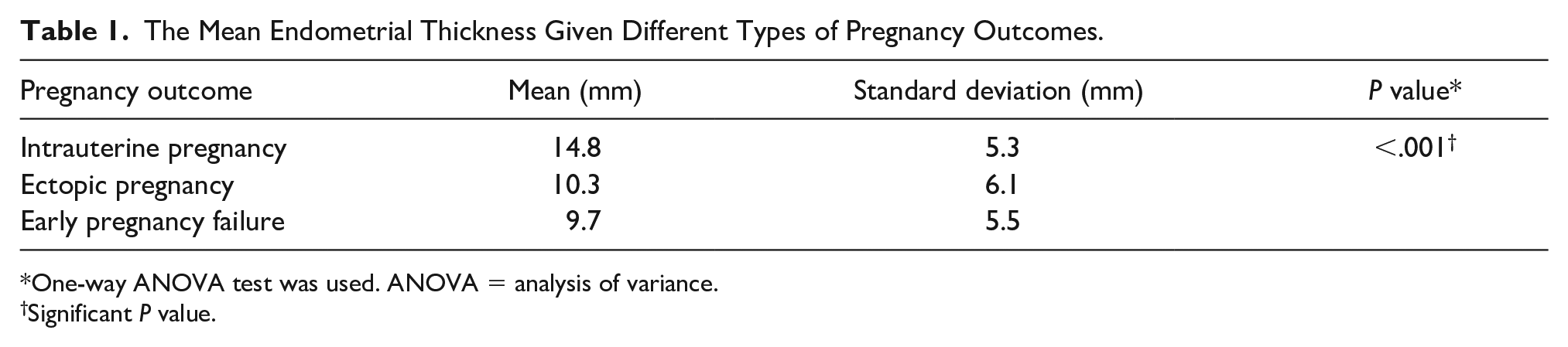
One-way ANOVA test was used. ANOVA = analysis of variance.
Significant P value.
The Distribution of Endometrial Sonographic Patterns, With Varied Types of Pregnancy Outcomes.

κ2-test was used.
A one way ANOVA test demonstrated that the initial endometrial stripe thickness had a statistically significant relationship with PUL outcome (P < .05). The least significant difference test, showed that mean initial endometrial stripe thickness in women with normal IUP was more than those with abnormal pregnancy outcomes; either EP or early pregnancy failure (P < .05); However, it did not show a statistically significant value between EP and early pregnancy failure groups (P = .5).
The ROC curve analysis, for the initial endometrial stripe thickness, demonstrated that the area under the curve was 0.735 (standard error of 0.052; 95% confidence interval between 0.67–0.79; see Figure. 2). The optimum cut-off value for predicting EP rather than normal IUP was 11 mm, with a sensitivity of 73.3%, specificity of 39%, a positive predictive value of 56%, and a negative predictive value of 85.5% (P < .001).
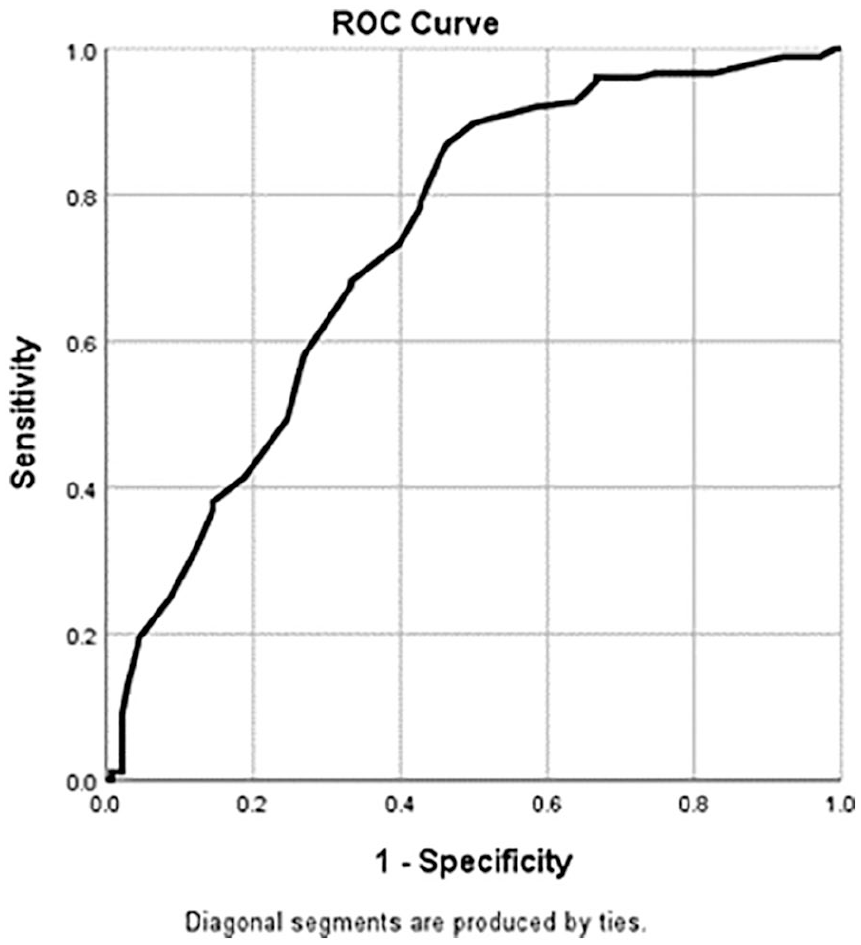
The receiver–operating characteristics (ROC) curve of endometrial stripe thickness for predicting ectopic pregnancy.
The κ2-test demonstrated that PUL outcome did not have a statistically significant relationship with the endometrial sonographic pattern (P = .15).
Discussion
This study was devised to investigate a discriminatory initial endometrial stripe thickness to predict early pregnancy outcome, for symptomatic women with a positive quantitative serum β-hCG test, as well as those without a sonographic finding of IUP or EP. Also, the association between ectopic pregnancy and endometrial sonographic pattern was assessed.
This study was conducted over 330 symptomatic pregnant women, diagnosed as PUL, during their first sonographic evaluation. This large cohort was later categorized into 3 distinct groups, based on their final and definite pregnancy outcomes during follow-ups visits: (1) IUP, (2) EP, and (3) an early pregnancy failure. Statistical analyses showed that initial endometrial stripe thickness had a statistically significant relationship with PUL outcome, which was in concordance with previous studies.10–16 This study demonstrated that there was no statistically significant difference between EP and early pregnancy failure groups. These results are similar to those reported by Mehta et al, 15 who also did not find a significant difference in initial endometrial stripe thickness between the EP and early pregnancy failure groups. Moschos and Twickler, 13 reported a directly proportional association between initial endometrial stripe thickness and the probability of normal IUP, among women experiencing PUL, during their first sonogram. That study also, concluded that an initial endometrial stripe thickness was significantly higher in EP patients compared to those with early pregnancy failure.
In this study, a cut-off point was determined for an initial endometrial stripe thickness, to predict EP. These results demonstrated that an initial endometrial stripe thickness measured less than 11 mm, in patients experiencing PUL, could be used as a predictor of EP with a sensitivity of 73.3% and specificity of 39%. This sensitivity and specificity for such a high-risk group cannot support specific predictions but could suggest an endometrial stripe thickness more than which the probability of EP is negligible, rather than normal IUP. The cut-off initial endometrial stripe thickness in this study was higher than those studies that have suggested ranges from 8 to 10 mm thick.10–12,16 Interestingly, an endometrial stripe thickness of close to 11.2 mm was introduced by Reid et al. 18 According to Yadav et al, 11 the variation in the endometrial stripe thickness cut-offs among different studies may be due to different measurement techniques, which necessitates using a standardized method.
The work of Yadav et al 11 suggested that the combination of endometrial stripe thickness and an endometrial sonographic pattern was a sensitive and specific way of predicting pregnancy outcome. They suggested the cut-off point of 9.8 mm for initial endometrial stripe thickness, which differentiated EP from IUP. Also, the most sensitive and specific endometrial echo patterns for diagnosis of EP were concluded to be heterogeneous hyperechoic and trilaminar patterns, respectively. In the most recent study, Chu et al 10 estimated the critical point of 10 mm for initial endometrial stripe thickness, less than which can predict abnormal pregnancy outcome. Also, some echo characteristics of the endometrium during sonography, like high-echogenicity and trilaminar echo pattern, were discovered in 72.60% and 27.40% of tubal EP patients, respectively.
Also in this study, it was concluded that there was no significant relationship between endometrial sonographic pattern and the outcome of PUL, which was in contrast with the findings of Chen et al, 12 Yadav et al 11 and Chu et al, 10 which all concluded that trilaminar and heterogeneous hyperechoic patterns were significantly more prevalent among patients, who suffered abnormal pregnancy outcomes. Maybe, subjective interpretation of endometrial echo pattern and different measurement techniques among different studies, can explain the incongruent results. A representative image is provided from a case with the final diagnosis of EP, whose endometrial echo pattern was hyperechoic monolayer (see Figure 3).

Transvaginal sonogram during the first 24 hours of referral is provided for a 31-year-old woman complaining of abdominal pain and vaginal bleeding, following a missed period. An initial endometrial stripe thickness of 8.6 mm and hyperechoic monolayer endometrial sonographic pattern was noted. An ectopic pregnancy was the final diagnosis, at the conclusion of the follow-up session.
Limitations
Some limitations are inherent in this study, given the research design was pre-experimental and the convenient sample of patients. Additionally, limitations exist for conducting a study only among symptomatic patients who were referred to tertiary care centers. This design makes the epidemiologic results unrepresentative for the normal community, as well as the lack of ethnicity variation. Also, it would be better if the quantitative serum β-hCG level of each patient was recorded and analyzed separately and in a model with endometrial appearance and thickness.
Conclusion
In this large cohort of patients, the endometrial stripe thickness of more than 11 mm, among those who were symptomatic and deemed as PUL, has the potential to predict ectopic pregnancy as an unlikely diagnosis. The findings of this study are not generalizable; however, they could be used as an option for early diagnosis of abnormal pregnancies. Replication of this study and a meta-analysis of these findings could help a medical system to prioritize patients based on their risk of developing poor outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Research Ethics Board of the Radiology Department in Isfahan University of Medical Sciences and the national research ethics committee (code: IR.MUI.MED.REC.1398.480).
Informed Consent
Informed consent was obtained from all individual participants included in the study. Informed consent to publish images (Figure 1A and ![]() ) has been obtained from those participants.
) has been obtained from those participants.