
Abstract
Objective:
The purpose of this study was to examine the effects of course delivery methods on examination grades and student perceptions in a sonography course.
Materials and Methods:
The participant included all sonography students (n = 103), enrolled at a Midwestern university, during the academic years (AY) of 2010–2021. A retrospective, convergent mixed-methods design was used to collect and analyze data, related to the course delivery method.
Results:
The highest overall mean examination score and course satisfaction rating resulted from the blended learning format and the lowest mean examination scores and course satisfaction resulted from the flipped learning format.
Conclusion:
Health professions students are a diverse group of learners. Pedagogical practices should include course design and delivery methods which educate all learners. Courses that balance both face-to-face learning with opportunities for self-directed learning improve student satisfaction which could lead to improved student outcomes and provide the foundation for students to become competent health care professionals.
Course delivery methods in higher education have evolved through the years with heightened awareness over the past 24 months, due to the COVID-19 pandemic. Educators and learners, with varying experience levels, quickly transitioned to a remote learning method for course delivery and education. As institutions return to campus, an opportunity exists for educators to pause and reflect on course delivery methods that better meet the needs of their learners. While the effectiveness of teaching methods has been researched extensively in higher education, little research has been conducted specific to course delivery methods in sonography education.
Current literature on health professions education emphasizes the value of problem-based, student-centered, and active learning in the classroom to better prepare students, for their role as health care professionals.1 –4 Applying the constructivist theory of student-centered learning allows educators to become facilitators of knowledge with educational activities designed to increase students’ ability to critically think at higher levels (analysis, synthesis, and evaluation), of Bloom’s taxonomy.5,6 This higher-order critical thinking is essential for providing patient-centered care in medicine, nursing, and other health care professions.7,8
Lecture is one of the oldest, most used, and most preferred course delivery methods.2,3 In this traditional learning approach, the instructor delivers knowledge while the student passively accepts the information. 9 Lecture format has proven to be an efficient teaching method, although the teacher-centered focus has disadvantages. Ge et al. 10 found a teacher-oriented pedagogy where students act as passive recipients of information encourages rote learning without understanding. Lecture does not provide opportunity for assessment of student learning at higher cognitive levels or promotion of student engagement in the classroom, both of which have been shown to improve student learning.5,11,12 As technology and pedagogical methods evolve, medical imaging education has begun to transition away from traditional, face-to-face didactic instruction.13,14
Online learning, synchronous or asynchronous, occurs when all course activity is completed in a web-based format, with no face-to-face or on-campus activity. 15 While online learning allows for more flexibility for students and instructors, students may need extra motivation, organization, and self-discipline to be successful. 16 In terms of quality, research in the field of online learning shows there is no significant difference in student outcomes when comparing online versus face-to-face courses, although research in health professions education notes inconsistencies in the outcomes.17 –19 Williams 19 conducted a comprehensive meta-analysis on research-based distance education literature, in allied health professions education. The study showed small, positive gains in achievement outcomes for distance students when compared with traditional education students. A more recent study conducted by Pei and Wu 18 evaluated online and offline learning in undergraduate medical students. The study concluded that online learning was at least as effective as offline learning for this group of students, although the authors note further research is still needed to confirm conclusions on the comparison. Specifically related to medical imaging students, a study by Bagley et al. 20 found lower student outcomes in a synchronous distance education anatomy course which enrolled sonography and radiography students. A limited study by Papillion and Aaron 13 found student perceptions of online radiologic science courses to be mixed, and only 58% of students said they would recommend an online course to a friend.
With a flipped learning format, foundational classroom lecture material is moved to prework and classroom time is transformed into an interactive learning environment where the educator guides students as they apply concepts and engage creatively in the subject matter.7,21 The flipped learning method is employed in two phases. The prework phase occurs outside the classroom and requires completion of a self-directed learning activity. The second phase occurs in the physical classroom and uses interactive activities designed for integration and application of phase 1 knowledge. The flipped learning format helps transition learners from passive transmission to active processing of information. 8 A meta-analysis conducted by Ge et al. 10 showed improved student performance and satisfaction, and increased opportunity for active learning in radiology education, when the flipped classroom was employed.
A blended learning format allows educators to incorporate multiple teaching and learning activities into the course including online coursework, face-to-face instructional activities, lectures, discussions, flipped learning, labs, and/or other learning activities. 15 Blended learning may be more conducive to health professions education as foundational knowledge and clinical reasoning can be taught online, while examination and procedural skills require direct contact.1,22 Bleiker et al. 22 conducted a small-scale study of blended learning to teach patient care to radiography students. While students expressed positive feedback regarding the format, student outcomes were not evaluated. A scoping review by Arora et al. 12 found a blended or hybrid learning format to be highly effective in providing opportunities for meaningful learning; learners were able to tailor their educational experiences according to their needs and objectives. Vavasseur et al. 23 further supported the blended classroom. The study noted a statistically significant change in pre- to post-test scores when using a blended approach to teach radiology to medical students. Ninety-nine percent of the students rated the experience as above average to excellent, 95% felt they improved their knowledge, and 99% would recommend the learning format in other medical imaging fields. 23
The purpose of this retrospective, convergent mixed-methods study was to examine the effects of different course delivery methods on examination grades and student perceptions in a sonography course. The following research questions were explored in this study:
Materials and Methods
A retrospective, convergent mixed-methods study was conducted at a Commission on Accreditation of Allied Health Education (CAAHEP)-accredited ultrasound program, at a Midwestern academic health science center. A convergent mixed-methods study design allows for quantitative and qualitative data to be collected in parallel, analyzed separately, and then merged. This type of study provides a more in-depth understanding of the data, the research problem, and the research questions. 24 The study focused on a one semester credit hour sonography course, offered in the second semester, of a bachelor of science sonography program. The course met weekly and included 13 classes and three unit examinations. Over a 12-year period, the course had been taught using four different delivery methods, each 3 years in duration, and included traditional lecture, online asynchronous, flipped learning, and blended learning. Although the format of delivery differed during the 12-year period, the overall course content and examinations remained consistent, with minor corrections to grammar/spelling errors and updates to sonograms. The variation in course delivery method was initially not intentional but evolved based on programmatic circumstances (faculty availability and student time on campus), and the desire to use innovative and evidence-based practices to improve the course and provide an optimal learning environment.
The study population (n = 103) included all sonography students, who completed the course between academic years (AY) 2010 and 2021. All students enrolled in the program had completed a minimum of 21 hours of college prerequisites and an accredited radiography program.
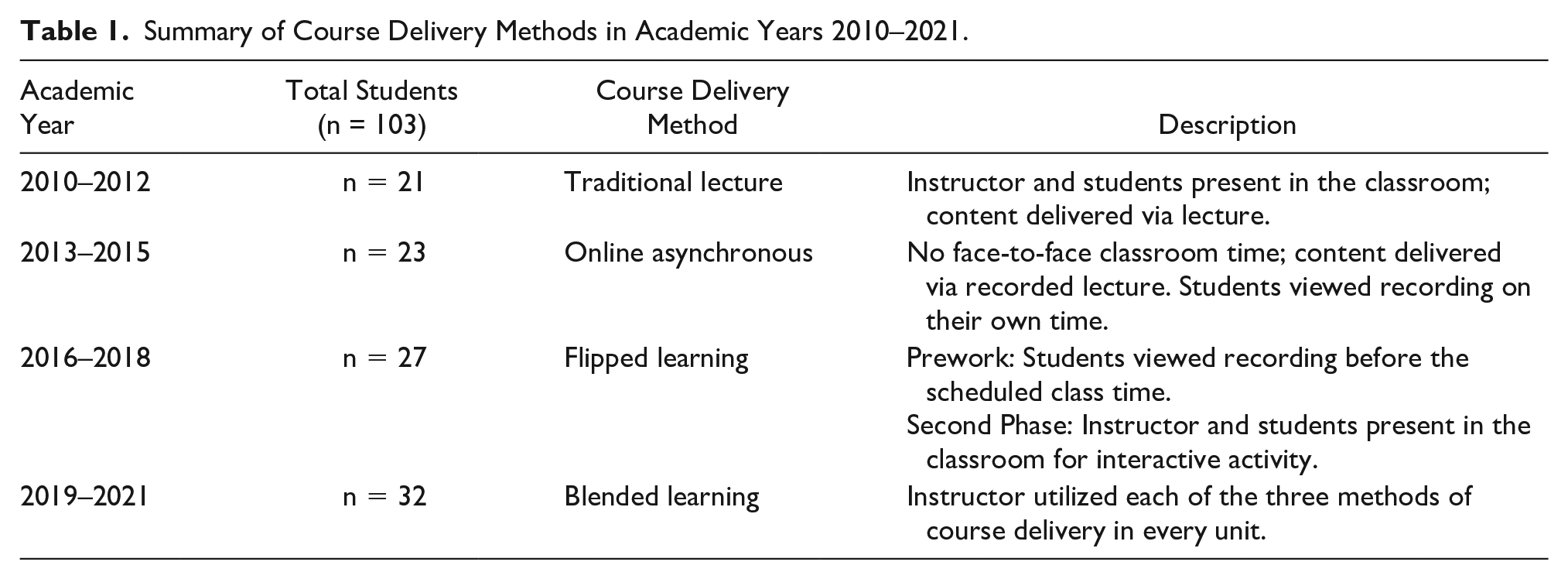
During AY 2010–2012, the 13-lecture course used a traditional lecture format with both the instructor and the students in the classroom, and course content delivered by the instructor using a PowerPoint presentation. In AY 2013–2015, the course transitioned to an online asynchronous format where the instructor posted a weekly recorded PowerPoint lecture and quiz to the learning management system (LMS). Designated office hours were available to answer student questions about the content. Academic years 2016–2018 transitioned to flipped learning. Students reviewed weekly recorded lectures posted to the LMS prior to in-class sessions that reinforced the lecture content through application or class interaction. The final 3 years of the study (AY 2019–2021) used blended learning with each of the three course units incorporating a combination of all delivery methods, traditional, online asynchronous, and flipped learning. All examinations were computerized and proctored either in the face-to-face setting or via video conferencing (see Table 1).
Summary of Course Delivery Methods in Academic Years 2010–2021.
Quantitative data included the three unit examination scores from each year and data from the end-of-semester course survey. All examination data were anonymized using a key created by the program director. End-of-semester surveys were administered through the LMS and anonymous. Qualitative data were gathered from the final open-ended question on the end-of-semester survey which asked for “additional comments about the course.” Responses to the open-ended question were cleaned, organized, and then analyzed independently by two members of the research team using a preliminary exploratory analysis followed by coding, and finally organized into themes. Inconsistencies between the researchers were discussed until agreement was reached. Results were presented to the research team for agreement. The study was classified as exempt educational, behavioral, and social science research (IRB # 014-16-EX).
Statistical Analysis
Examination scores and prerequisite grade point averages (GPA) were analyzed using descriptive statistics, including means and standard deviations. An analysis of variance model was used to compare prerequisite GPA across teaching modalities. Linear mixed effects models were used to model the outcomes of the individual examination scores and mean examination scores by course delivery method. The models also included fixed effects for prerequisite GPA. To account for year-to-year and instructor variation, the models included random effects for year which was nested within course delivery method and captures the random effects of the instructors.
Differences in responses to semester end survey questions across course delivery methods were evaluated using generalized linear mixed models for the ordinal responses to the questions. For each model, classroom type was a fixed effect, year (within classroom type) was a random effect, and a multinomial distribution was assumed for the outcome. All analyses were done using SAS v9.4 (SAS Institute, Cary, North Carolina) A priori the statistical significance was set at a P value of <.05.
Results
Quantitative Phase
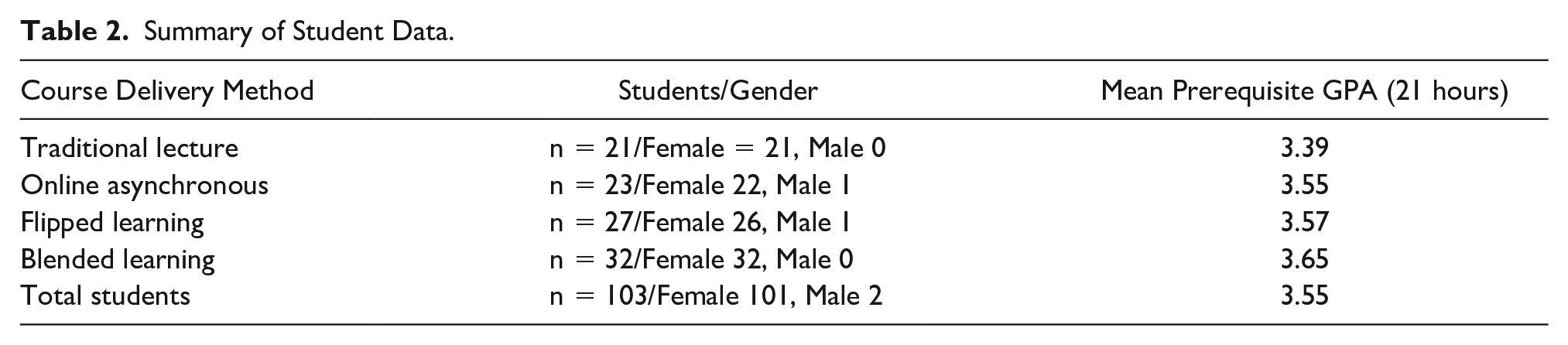
Study participants were predominantly female (n = 101, 98%). Male students (n = 2) were represented only in the online asynchronous and flipped learning delivery classrooms. The overall mean prerequisite GPA for all students was 3.55 with students in the blended delivery cohort having the highest mean GPA at 3.65 and students in the traditional lecture cohort having the lowest GPA at 3.39. Mean prerequisite GPAs for the flipped learning cohort (3.57) and the online cohort (3.55) ranked between these two groups, respectively. The traditional lecture cohort GPA was significantly lower than the flipped learning cohort (P = .04) and the blended learning format (P = .002) (see Table 2).
Summary of Student Data.
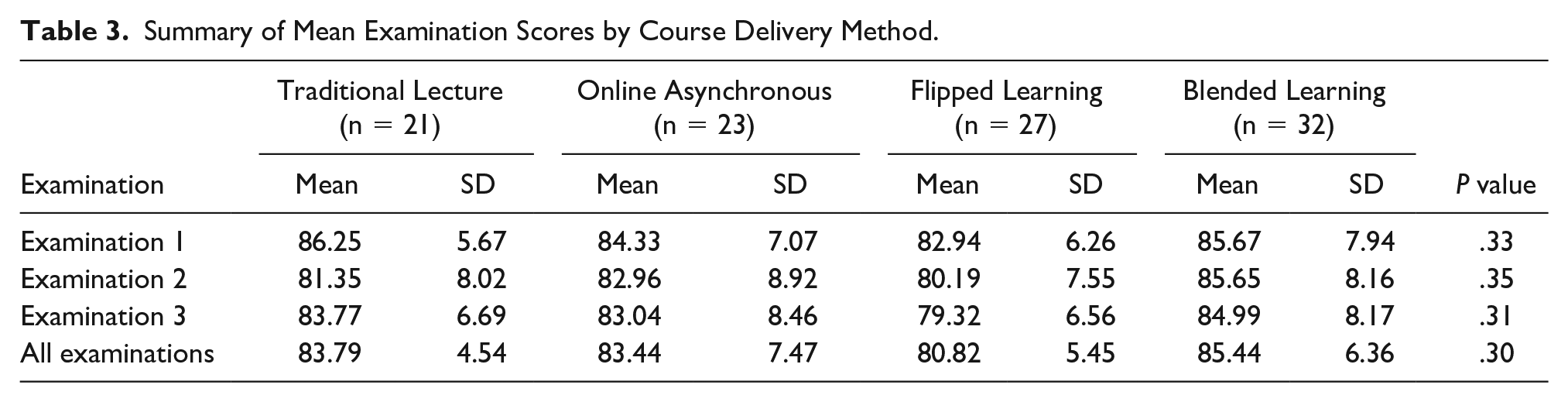
Three unit examinations were included in the course each year. Although not significant, the mean examination average was highest with the blended learning format followed by the traditional lecture, online asynchronous, and flipped learning, respectively. Overall, the highest mean examination score for any examination occurred in examination 1 (86.25) in the traditional lecture format. The blended learning format showed the highest mean examination scores for examination 2 (85.65) and examination 3 (84.99). The flipped learning delivery method consistently had the lowest mean scores for each examination and the overall lowest mean examination score (80.82). Overall, the course delivery method was not a significant predictor of examination score after adjusting for the other measures (see Table 3).
Summary of Mean Examination Scores by Course Delivery Method.
When examining mean examination scores and mean prerequisite GPA, the highest mean score and GPA were found in the blended cohort. Although the lowest GPA occurred in the traditional lecture format, the mean examination scores for this cohort ranked second highest among the four groups. Mean GPA and mean examination scores in the online cohort ranked third in each category. Interestingly, the cohort with the second highest mean GPA, flipped learning, had the lowest mean examination score overall and for every examination.
At the end of each semester, students were asked to complete a course survey. Of the 103 participants, 94.1% (n = 97) completed the anonymous survey. Survey completion rate ranged from 100% in the traditional lecture format to 74.2% in the flipped learning format. Data from two survey questions related to the research study. The first question, The format for this course was appropriate, included response choices of “strongly agree,” “agree,” “disagree,” “strongly disagree,” and “does not apply” (see Graph 1). All participants in the traditional lecture delivery format strongly agreed (42.9%) or agreed (57.1%) with this statement. This was the only delivery format to have no “disagree” or “strongly disagree” responses. Almost one-third (27.3%) of the online asynchronous participants disagreed and almost half (47.8%) of the flipped learning participants disagreed with the appropriateness of the course delivery format. Agreement with the format for the blended method almost returned to match that of the traditional delivery method with more than 90% of the participants reporting “strongly agree” (45.2%) or “agree” (45.2%). In summary, student responses reflected a preference for the traditional lecture and blended learning format over the online asynchronous and flipped learning formats. Although there was a difference in the distribution of responses between the course delivery formats, it did not reach significance (P = .085).
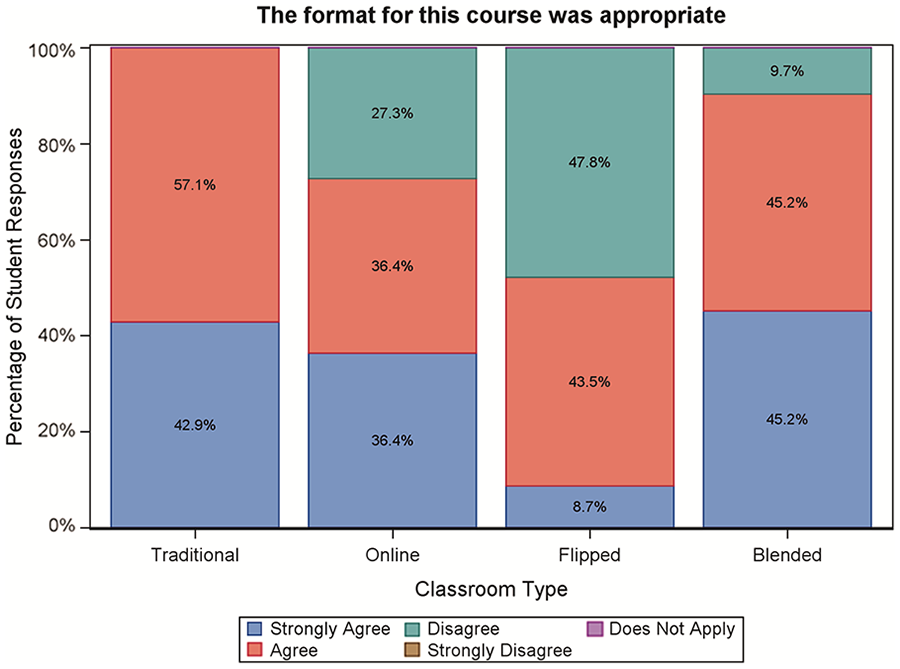
Summary of survey responses to “The format for this course was appropriate.”
The second survey question analyzed, Overall, I would rate this course, and included response choices of “Outstanding,” “More than Satisfactory,” “Satisfactory,” “Less than Satisfactory,” and “Completely Unsatisfactory” (Graph 2). Data showed all course delivery formats, except flipped learning, were rated by the participants as “Satisfactory” or higher. The traditional format received the highest percentage (33.3%) of “Outstanding” responses, and the blended learning format reported the highest percentage (51.6%) of “More than Satisfactory” responses. Although the flipped learning format received the highest percentage of “Satisfactory” responses (47.8%) among the four delivery formats, it was the only one that received “Less than Satisfactory” (17.4%) and “Completely Unsatisfactory” (4.3%) responses. Overall, students rated all formats as satisfactory except for the flipped learning delivery format. The difference in response distributions between the course delivery methods did not reach statistical significance (P = .061).
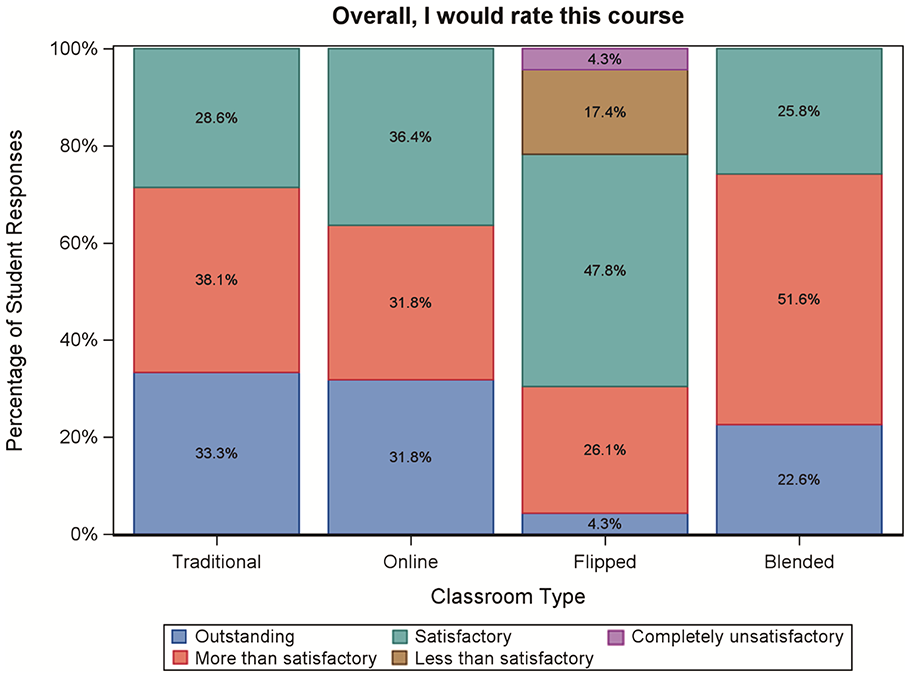
Summary of survey responses for “Overall, I would rate the course.”
Qualitative Phase
The final open-ended question on the course survey, please use this space for additional comments about the course, allowed the study participants to share additional comments about the course. A total of 62% (n = 60/97) of participants completing the survey added comments to this question and this varied by course delivery format. Comments specific to course format were analyzed and coded by course delivery method into positive and negative themes with subthemes of Mode, Time, and Importance, emerging in some delivery methods.
The flipped learning surveys had the highest percentage of student comments (87.0%) and most of these were negative themes (90%, n = 18/20). In this format, students were required to come to class ready to apply information learned in the recorded lecture. Comments fell into all three subthemes of Mode, Time, and Importance. In the Mode subtheme, students reported diminished learning based on teaching themselves or completing activities that did not help to understand the information. For the Time subtheme, students expressed dissatisfaction with the prework time required to prepare for class and the perception of wasted time as they did not feel they learned the material. The importance of the course and the information presented was questioned as the activities were viewed as “busy work” and often the prework was not completed before class. One participant did report a neutral comment for the Mode subtheme stating the in-class activities were beneficial to learning.
For the online asynchronous format, 68% (n = 15/22) of students included comments with the majority revealing negative themes (66.7%) over positive themes (20%). In this delivery format, students were responsible for reviewing the weekly recorded lectures when it best suited their schedule. Subthemes related to Mode reported a desire to return to traditional lecture as the online format was not conducive to learning difficult and/or critical information. The Time subtheme referred to the impingement on “their time” after they left campus or clinic. Concerning the subtheme of Importance, students expressed the online format lowered the priority of the course relative to other classes and the coursework was overlooked during the week. Twenty percent (n = 3/15) of participants did like the format but did not expand on why they liked it.
For the blended learning format, 64.5% (n = 20/31) of students added comments to the survey with the majority reflecting a positive theme (70%). Blended learning varied the weekly format course delivery but included each format in every unit. Subthemes for Mode found improved learning, enjoyment of the in-class activities, and the ability to apply information as part of the flipped learning approach. The option to balance some of the learning on their own time was appreciated (subtheme Time), and the coursework became important as students were motivated to prepare for competitive games (subtheme Importance). Fewer negative comments, 20%, were reported; these comments related to the subtheme of Mode and were in response to confusion with the weekly change in delivery formats.
Only 23.8% (n = 5/21) of students left comments for the traditional lecture format. The comments were unrelated to both course format and the three subthemes of Mode, Time, and Importance. The lack of comments could be explained by the students’ familiarity and comfort with this format of delivery.
In summary, while the qualitative findings show the blended learning format resulted in predominantly positive survey responses, and the highest percentage of positive comments, examination outcomes did not show significant difference between delivery methods. The online asynchronous and flipped learning delivery format had the lowest overall mean examination scores and were the least preferred based on survey data and student comments. The traditional lecture format had the second highest overall mean examination scores, and positive survey responses, although the qualitative data were not sufficient to assist in explaining course outcomes.
Discussion
The pedagogy of teaching is a dynamic and evolving science. For the instructor, the primary goal is to deliver information to the learner in a way that effectively and efficiently promotes analysis, understanding, and application of the information. For the learner, the goal may be narrower, focusing on the acquisition of information necessary to pass the examinations and complete the course. The method of delivery may not be the learner’s primary concern unless it differs significantly from previous experiences or requires more time outside of the classroom.
The traditional lecture format reported the highest mean examination score in the study and an overall high satisfaction rate with the course. All participants reported the course format was appropriate and none of the survey comments referred to the delivery format. It is important to note that the traditional lecture format data were gathered during AY 2010–2012, and at that time, the lecture format was still at the forefront of higher education, particularly health professions education.3,13 Participants most likely were familiar and comfortable with this passive method of learning based on educational experiences. In addition, all other courses in the ultrasound program were delivered in this format which may have further promoted comfort levels and format acceptance. While traditional lecture format is one of the oldest methods of course delivery and is known to be an effective and efficient method of delivery, it is not learner-centric and may not promote higher levels of thinking, such as application and analysis which are important for health care professions.3,11,25
Between 2013 and 2015, the course was delivered in an online asynchronous format through the LMS. The move away from the traditional lecture format course was based on faculty availability, and course and student schedules. It was the only course in the program’s curriculum to not be delivered in the traditional format. When compared with traditional delivery, the overall mean examination score dropped slightly with the online asynchronous format. Although all participants rated the course as satisfactory or higher, almost one-third disagreed with the delivery format and this disagreement was also reflected in the survey comments. Participants knew the course had previously been delivered in traditional format and cited a need to return to that format. In addition, participants questioned the importance of the course relative to other courses due to it being the only course delivered using an online format. A lack of motivation and engagement in the course was reported which may have emerged based on the perception of reduced importance and/or the new responsibility of self-directed learning.
The literature notes the importance of student perceptions when evaluating online courses. Students who are dissatisfied with the course format tend to be less motivated and less engaged. Motivation and willingness to engage with the information and in the classroom are crucial to the success of the course delivery method.5,11,25 Age, maturity, and academic aptitude have also been implicated as reasons for success and failure when comparing methods. 20 For this cohort of students, the experience may have been their first exposure to an online course which could explain their preference for instruction during a scheduled class time with content delivery occurring at this time. It may also suggest undergraduate ultrasound students are developing as self-directed adult learners and may prefer to remain passive listeners in a teacher-oriented pedagogy. Before introducing a new course delivery method, it is important for faculty to assess learner readiness and provide orientation to the new format.26,27
A new faculty hire with an interest in educational innovation moved the course to a flipped learning format in 2013. All lectures were delivered in the flipped format and in-class engagement activities were created using modified examples from the literature. Although participants were oriented to this pedagogy prior to starting class, course outcomes and evaluations showed limited student buy-in and commitment. Although participants should have spent twice the amount of time engaged with the material each week (pre-course work and in-class application activity), mean examination grades were the lowest with this delivery method. The end-of-semester survey reported the highest levels of disagreement with this delivery format, and the greatest overall course dissatisfaction, noted by negative comments. Table 4 provides a representative example of a flipped learning unit.
Example of Flipped Learning Format (Unit 1; 2018).
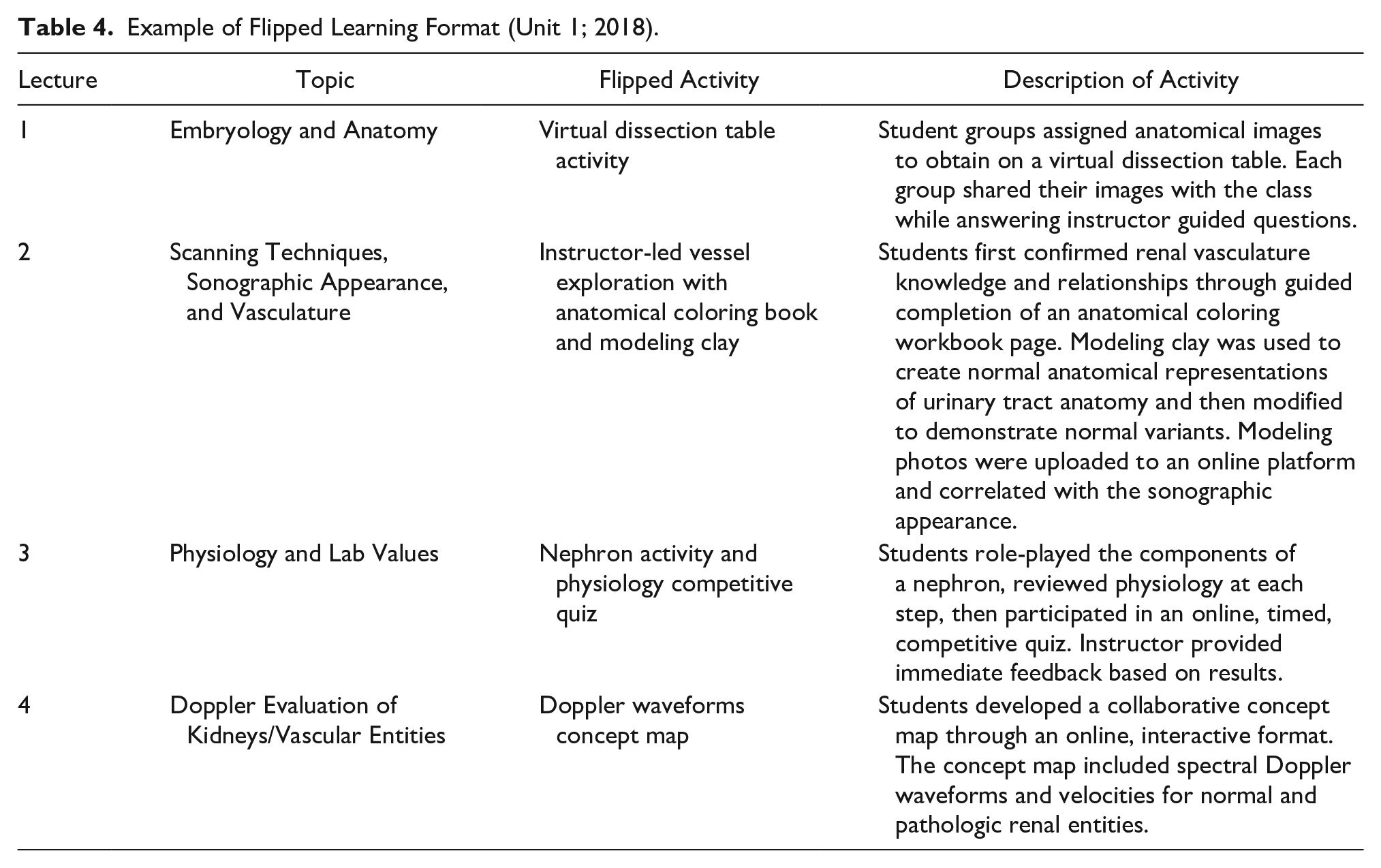
Implementation of the flipped learning approach requires a substantial time commitment for both faculty and students.7,8,10,26 For this cohort, the pre-course work time requirement was a particular concern and was described as extra work even though it should have reduced the amount of examination study time. Although in-class activities such as online quizzing and the use of a virtual anatomy platform increased discussion and engagement, other activities, such as the anatomy color book and the vascular modeling clay activity, were perceived as “busy work” and not relevant to information application.This perception could have been related to failure to complete the preparatory work or poor correlation of the activity with the material presented. Participants again questioned the importance of the course material based on the delivery format varying from other courses.
The study findings do not support published data showing the flipped learning format improved student outcomes or improved course satisfaction.7,25,26 It is recommended for faculty implementing a flipped learning approach to consider easing into the method versus flipping an entire course. Instructors should investigate the course topics which are more conducive to the format and flip those first. Communicating clear expectations along with the benefits of the flipped learning method to students prior to the beginning of the course will assist faculty in gaining greater acceptance of the flipped learning method.7,8,10,26
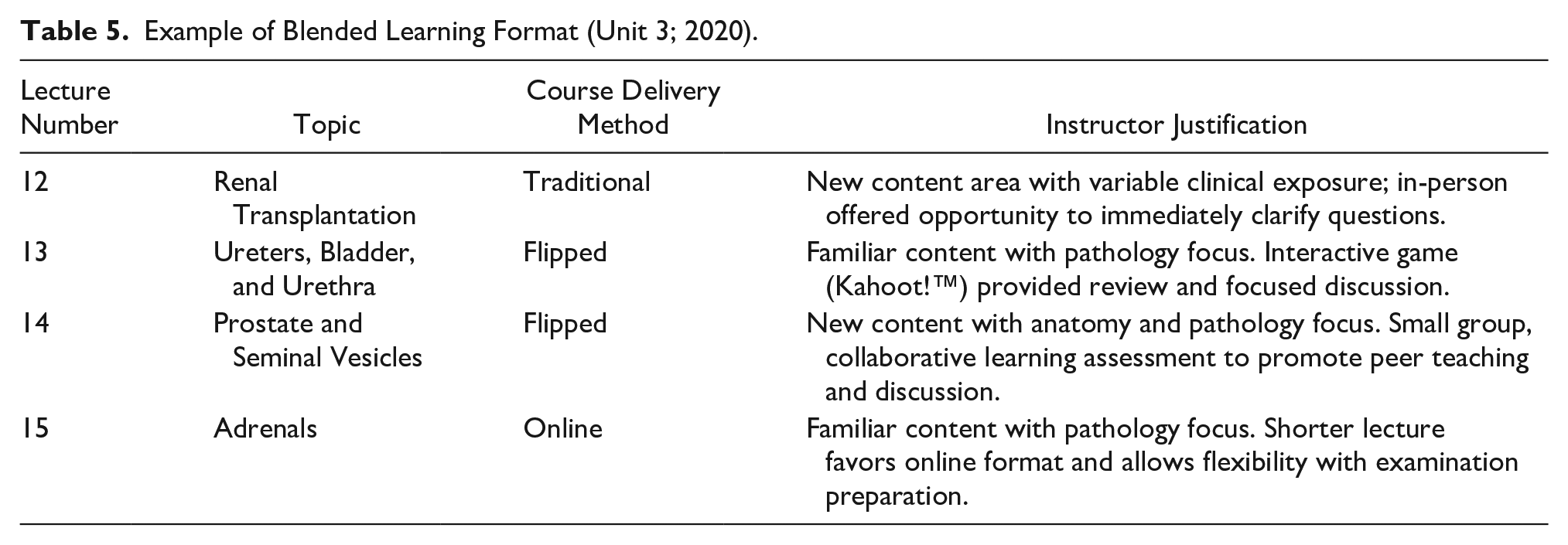
The blended learning format produced the best combination of outcomes with the highest overall examination average. While not significant, these findings support the body of literature showing student engagement in the classroom correlates with higher levels of Bloom taxonomy and students should score higher in courses having a more interactive (flipped/blended) format.5,6,11 Study findings also correlate with pedological practices which show inclusion of active teaching strategies improves student outcomes, increases student attendance, and promotes engagement.5,11,25 The blended learning format purposefully incorporated each type of delivery format into each unit. To optimize active learning and a student-centered classroom, two lectures per unit used the flipped learning format. Matching of lecture content to delivery format was guided by the instructor’s experiences in the final year (2015) of the flipped learning format. Table 5 provides a representative example of a blended learning unit.
Example of Blended Learning Format (Unit 3; 2020).
The favorable outcomes were supported by the qualitative data, and delivery formats previously viewed as negative were seen in a more favorable light. The online asynchronous class now offered a break from the designated class time and no comments suggested an infringement on student time. The flipped learning activities were competitive, team-based, and included in the syllabus. These changes may have eliminated the perception of “busy work,” justified the outside pre-work time, and created a learning environment that fit the participants’ competitive spirit. With three of the four class periods now meeting in a face-to-face setting, the course resembled a more traditional method of delivery similar to others in the curriculum. Survey comments on the importance of the course disappeared. The incorporation of all delivery formats paired with a course topic improved examination outcomes and course satisfaction.
Limitations
This study’s main limitation was the research design. In addition, the study population included students from only one health profession program which limits the generalization of findings to other student populations. The study occurred over a 12-year period and the type of learners may have evolved over this time based on learning experiences in secondary and postsecondary courses. A pre-course survey to assess participants’ prior exposure to course delivery methods would have added to the understanding of research findings.
The study was only conducted in one course which improved internal validity, but a different course may produce different results. Over the 12-year period, the course had five different instructors. One instructor taught all 3 years of the traditional lecture format, one instructor taught all 3 years of the online asynchronous format, three different instructors taught each year of the flipped learning format, and one instructor taught all 3 years of the blended learning format. It is important to note the instructor for the blended learning format also taught the final year of the flipped learning format which allowed for adaptation of the course delivery methods over time. Instructor variability, teaching experience, and comfort level with a course delivery method may have affected outcomes and satisfaction particularly in the flipped and blended learning formats.
In 2015 (flipped learning format), a satellite site was added to the program. After this time, all program courses were delivered synchronously via videoconferencing with the in-person classroom located at the satellite campus. In 2020 (blended learning format), the course moved to remote learning during the COVID-19 pandemic. The instructor was able to maintain the scheduled course delivery format outlined in the syllabus. The continuity of the schedule and the elevated level of course engagement may have added some normalcy during an uncertain time and positively skewed course outcomes. The impact of remote learning was lessened based on the instructor and student’s comfort with the videoconferencing technology.
Conclusion
Health professions students are a diverse group of learners. Pedagogical practices should include course design and delivery methods which educate all learners. When adopting a new course delivery method, it is important for faculty to assess students’ prior experience with the format along with their readiness to implement the format. Courses that balance both face-to-face learning with opportunities for self-directed learning improve student satisfaction which could lead to improved student outcomes and provide the foundation for students to become competent health care professionals.
Expansion of this research, to include other health professions programs on the efficacy of course delivery formats along with the evaluation of outcomes related to educational pedagogy, is still needed. In addition to looking at course examination outcomes, future studies might evaluate performance on credentialing examinations to include examination pass rate and performance on item-specific outcomes. Research on how course delivery methods affect problem-solving, and critical thinking would also be beneficial in health professions education.
Footnotes
Ethics Approval
The study was classified as exempt educational, behavioral, and social science research (IRB # 014-16-EX).
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
NA
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
NA
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Joseph C. Anderson, MD, and Darlene Anderson Distinguished Professorship of Imaging Sciences.