
Abstract
A case report is presented of a 72-year-old woman with monophasic synovial sarcoma of the buttocks, diagnosed four years before. The tumor was treated with surgical removal followed by radiotherapy. The patient regularly underwent follow-up examinations and the last chest computed tomogram (CT) showed a left-sided pleural mass and ipsilateral effusion. The patient was admitted in hospital to obtain a specific histological diagnosis before treatment of chest pathology was initiated. An ultrasound (US)-guided fine needle aspiration biopsy (FNAB) of the pleural lesion and US-guided thoracentesis with drainage of blood serum pleural fluid were performed. The pathological examination of the lesion revealed a definitive diagnosis of synovial sarcoma of the pleura. For pleural-based lesions, the diagnostic accuracy of US-guided biopsy is similar to that of CT-guided biopsy, with a lower complication rate, the absence of radiation exposure to patients, and a significantly reduced procedural time. The presence of pleural effusion creates a favorable acoustic window for US-guided biopsy of pleural lesion, which is useful for the diagnosis.
Synovial sarcoma is a rare tumor of the soft tissues. Despite its name, it is not related to the synovial membrane, but originates from multipotent stem cells that differentiate into mesenchymal and/or epithelial structures. This tumor has a low incidence, the most frequent place of occurrence being the lower extremities in young adults. There are two main histological types, monophasic (most common) and biphasic, both of which show features of poor differentiation. It has a tendency for late recurrence and metastases, particularly in case of large tumors. 1 The pleura is not a commonly affected secondary site. An ultrasonographic examination is a cost-effective imaging modality that permits to obtain information about pleuropulmonary pathologies without the risk of exposure to ionizing radiation and provides the examiner with real-time and immediate results. Its ease of use, along with its portability to the patient’s bedside and accurate examination of the pleural space, has allowed for safer pleural procedures such as ultrasound (US)-guided thoracentesis and US-guided fine needle aspiration biopsy (FNAB), with the goal of establishing rapid diagnosis with these minimally invasive procedures.
Case Report
This is the case of a 72-year-old woman with monophasic synovial sarcoma of the buttocks diagnosed four years ago and treated with surgical removal followed by adjuvant radiotherapy. The patient regularly underwent follow-up examinations. The last chest computed tomogram (CT) showed a left-sided pleural lesion with ipsilateral pleural effusion (see Figure 1).
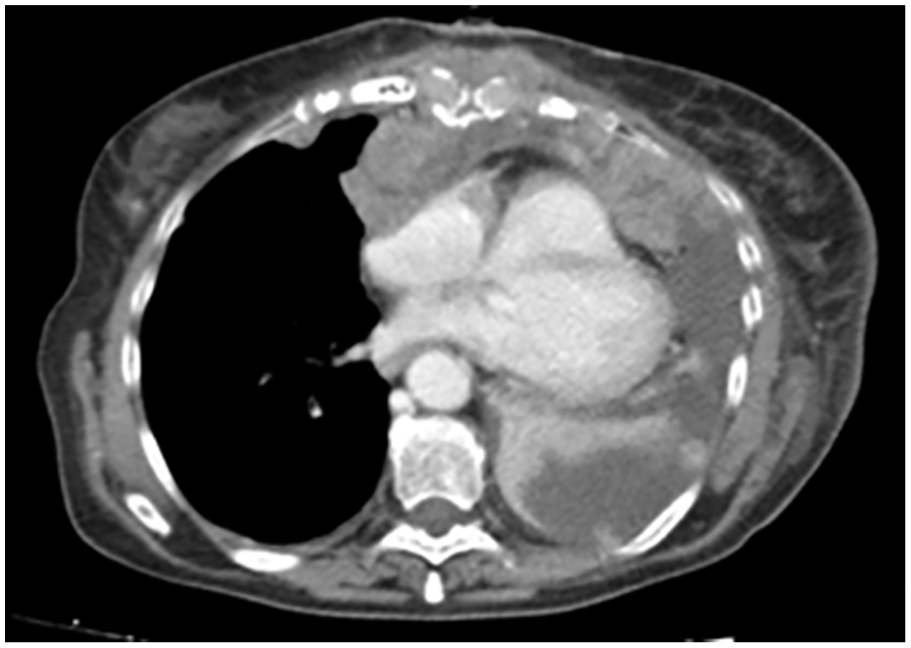
A chest computed tomogram shows a pleural lesion in the upper lobe of the left lung.
The patient was scheduled for a US-guided FNAB of the pleural-based intrathoracic lesion. Before the procedure, the coagulation profile (prothrombin time, partial thromboplastin time, and platelet count) was checked and a written informed consent was obtained. The patient was placed in a comfortable position, sitting upright and embracing a pillow. The exploration of the chest was conducted with intercostal longitudinal and transverse images, using a curved array transducer with 5 to 8 MHz. Once the lesion was located, its longitudinal and transverse dimensions were measured, depth from the skin surface was marked, and Doppler was used to certify the absence of blood vessels in the biopsy path. Chest wall invasion by the tumor was assessed by observing its movement with respiration and the direct extension into the chest wall. Images were recorded on a flash drive located on the US unit. The US-guided FNAB was performed by an interventional sonologist with 30 years experience using a “modified Menghini” technique.2,3 The biopsy site was disinfected with iodopovidone. The patient was instructed to suspend respiration and a semi-automatic 18-gauge Menghini-type needle was advanced in real time through the guide of a dedicated holed transducer (3.5–8 MHz). The syringe plunger was then released, removing the stylet and applying suction. 3 This allowed for obtaining a tissue frustol. Subsequently, US-guided thoracentesis was performed. An 18-gauge needle was attached to a three-way stopcock, placing a 50 mL syringe on one port and attaching a drainage tube to the other port. The needle was inserted along the upper border of the lower rib of the appropriate intercostal space with drainage of blood serum pleural fluid. Needle insertion and lung re-expansion during drainage were followed the entire time by real-time US guide 4 (see Figure 2).
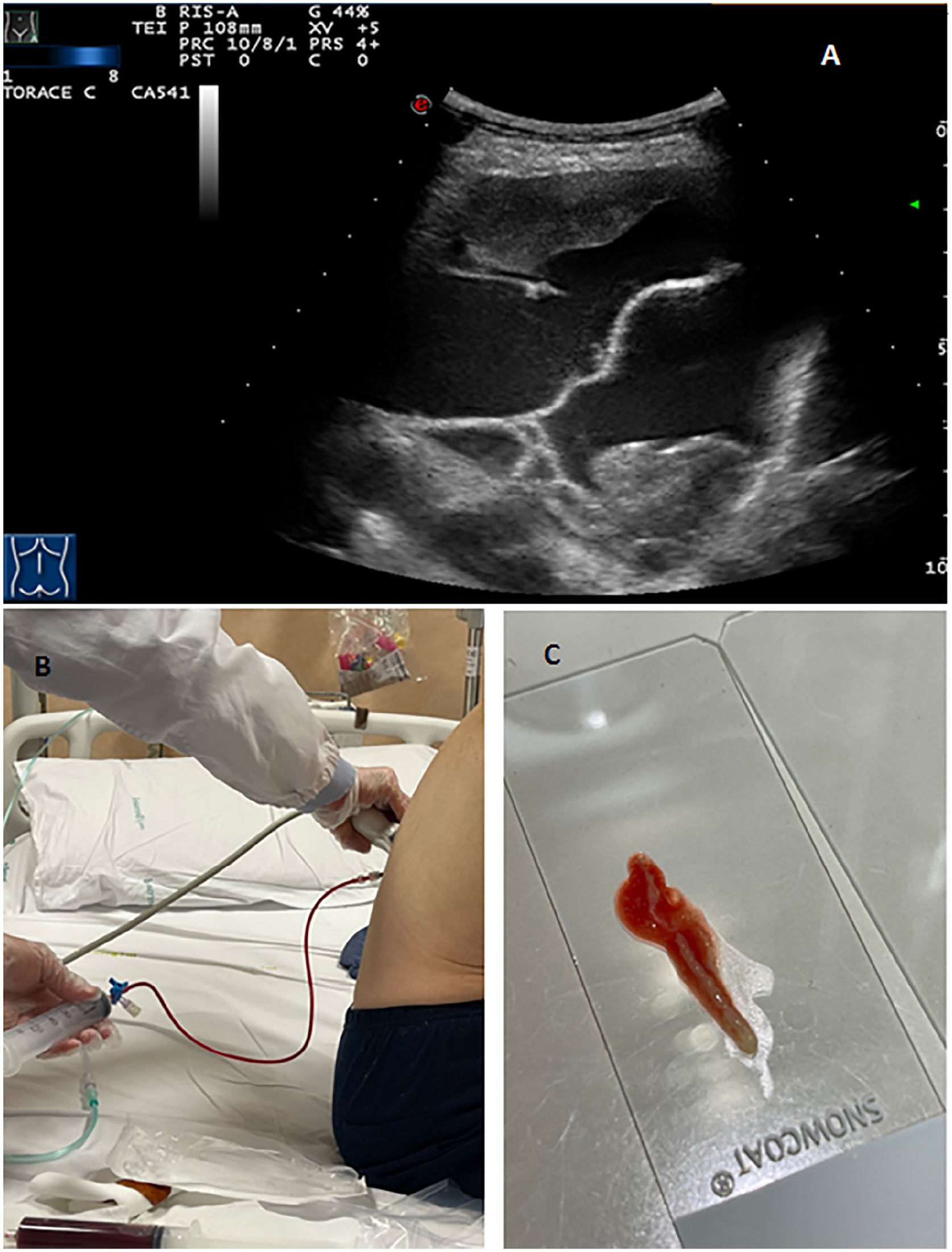
(A) An ultrasound examination showing the pleural lesion and a septated pleural effusion. (B) A thoracentesis procedure showing the collection of hematic pleural fluid. (C) A biopsy sample from the pleural lesion.
After each procedure, an US examination of the lung and a confirmatory chest radiograph were performed to rule out a pneumothorax. The final diagnosis was confirmed by histological analysis of the FNAB specimen that showed a malignant neoplasm, compatible with pleural synovial sarcoma.
Discussion
Peripheral nodules and masses are frequently encountered by pulmonary physicians and pose a diagnostic challenge, as the yield of bronchoscopy and sputum cytology is low for such lesions. Diagnostic options include percutaneous biopsy with image guidance (CT, fluoroscopy, and US), video-assisted thoracoscopy (VAT), or limited thoracotomy. 5 US-guided percutaneous biopsy of malignant peripheral pulmonary lesions has been shown to have a diagnostic accuracy comparable with that of CT scan-guided biopsy, with the addition of several advantages over CT guide.6,7 There is no radiation exposure. The US is portable, allowing for performing the procedure at patient’s bedside, if needed. It is less expensive, less time-consuming, and more readily available than CT. The procedure can be performed with the patient and the physician in a comfortable position: The physician does not have to wear a lead jacket, which allows for greater freedom of movement. A significant advantage of US is real-time guidance that allows for dynamic evaluation of the target lesion, for monitoring of the needle tip throughout the procedure, and for fine adjustments that can be made quickly and precisely.2,8 It is noteworthy that some small peripheral lesion may be visible only in one phase of the respiration: Real-time guidance allows for the biopsy to be conducted in the respiratory phase during which the lesion is most accessible with breath holding.8,9 Blood vessels can be assessed by Doppler US and can be avoided in real-time guidance. 7 Regarding methodological issues, the use of a dedicated probe with a central hole for the introduction of the needle set optimizes the procedure, as the US image is exactly on the line of the target lesion and the transducer. 10 The employment of an atraumatic 18-gauge Menghini-type needle allows to obtain specimens suitable for histological diagnosis, minimizing at the same time the occurrence of complications, which appear to be more frequent with needles of higher caliber (i.e., 14–16 gauge). 2 The US examination allows for assessment of chest wall’s invasion by the tumor better than CT.8,11 As limitation, some elements are needed so that an US-guided FNAB can be primarily performed: The patient has to be cooperative; there is no known bleeding tendency or coagulopathy; the lesion has to be pleural-based and the acoustic window is favorable to US assessment.3,12 In particular, the presence of ipsilateral pleural effusion, as in this case, allows an optimal view of the lesion to be biopsied as well as the differentiation between its pleural and pulmonary origin. 12
Conclusion
For pleural-based lesions, the diagnostic accuracy of US-guided biopsy is similar to that of CT-guided biopsy, with a lower complication rate and a significantly reduced time to the procedure. 7 The greatest advantage of the US-guided procedure is the real-time evaluation of the target lesion and of the needle tip during sampling.3,8 Some technical devices, such as the employment of a dedicated probe with a central guide for the bioptic needle insertion and of an atraumatic 18-gauge Menghini-type needle, can optimize the procedure.2,10 The presence of pleural effusion positively influences the diagnostic yield of the US-guided transthoracic biopsy in pleuropulmonary lesions, as it creates an adequate acoustic window that allows to better highlight the lesion itself. 12 In addition, US-guided thoracentesis may promote the safe drainage of the associated effusion through the monitoring of lung re-expansion during the procedure. 4 The US appearance may also suggest the probable nature of the effusion, guiding in advance the choice of the needle’s caliber to be used for thoracentesis: For example, a transudate (i.e., generally an anechoic effusion) will require a 20-gauge needle, whereas a corpusculate effusion (i.e., a septated or homogeneously echogenic effusion) will require the use of a larger 18-gauge needle. 13 Considering that US does not imply exposure to ionizing radiation and is easily performed at patient’s bedside, it should be the preferred approach in the presence of adequate skills.
Footnotes
Patient Consent Statement
The patient signed a written informed consent for all the procedures performed and provided the informed permission for the images publication. The images have been anonymized to protect patient’s privacy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.