
Abstract
Adventitial (adventitious) bursae occur as a pathological condition in areas between soft tissues and bone where abnormal friction arises due to professional, traumatic, or sport activity. An atypical localization of an adventitial bursa was noticed on the ulnar margin of the distal forearm in a woman with a mild bone misalignment, as a professional disorder. The clinical presentation was one of subcutaneous mass with mild pain and no local signs of inflammation. A 1-year follow-up visit noted the degeneration of the bursa into a cystic lesion, as proved with a grayscale sonogram, using a 14 MHz linear transducer. This was an unexpected chronic evolution. A quick literature search found either resolution or a chronic course with complications as fibrosis, infection, and ulceration of adventitial bursitis.
Bursae are fluid-filled sacs delimited by a synovial-lined wall, located in areas of friction between tendons, ligaments, muscles, and bones. This definition corresponds mainly to synovial bursae, situated in well-known areas and present at birth. Adventitial (adventitious) bursae appear in unexpected areas of increased friction between different structures during working, sportive, or traumatic events. Adventitial bursitis may resolve spontaneously or with conservative treatment, may embrace a chronic evolution, with fibrosis, suprainfection, fistulization, and so on. An unexpected chronic evolution is a cystic degeneration.
Case Report
In this journal, a case was presented of a woman, 46 years old, with a small subcutaneous lump on the ulnar margin of the distal forearm. 1 Her history recorded a distal radial epiphysis fracture 11 years prior, which had resulted in a radial deviation of the distal forearm and a small, painful lump on the ulnar side of the wrist 1 year prior. The sonogram revealed an adventitial bursitis. As she worked as a computer technician, with prolonged pressure of the ulnar margin of the forearm against the working table, the condition was considered as occupationally induced. 1
During the last year, she continued to work in the same manner, assuming the support position on the hard table for about 10 to 12 hours daily. The size of the tumor fluctuated a little over the time and the pain intensity oscillated between 1 and 5 on the visual analogue scale (VAS). The pain intensity used to decrease after a short working pause. There were no local inflammatory signs and no need for analgesic medication.
A grayscale sonographic examination was performed with a Toshiba Aplio ultrasound equipment system and a 14 MHz linear transducer. The area was examined with longitudinal and transversal views and the images were compared with those previously obtained 1 year ago. The purpose of comparing the acquired images with those obtained previously was to follow the structural pathologic evolution, in the involved area.
The first longitudinal sonogram, taken 1 year earlier (see Figure 1A), displayed an ovalar mass with poorly defined walls and an inhomogeneous hypoechoic content, over the distal ulnar epiphysis. The more recent sonographic image (see Figure 1B) revealed an ovalar mass in the subcutaneous tissue in the same position. The mass was anechoic with some fine hypoechoic parietal echoes and had well-defined margins. On sonopalpation, it demonstrated very little compressibility. There was no sign of hyperemia, during color Doppler examination.
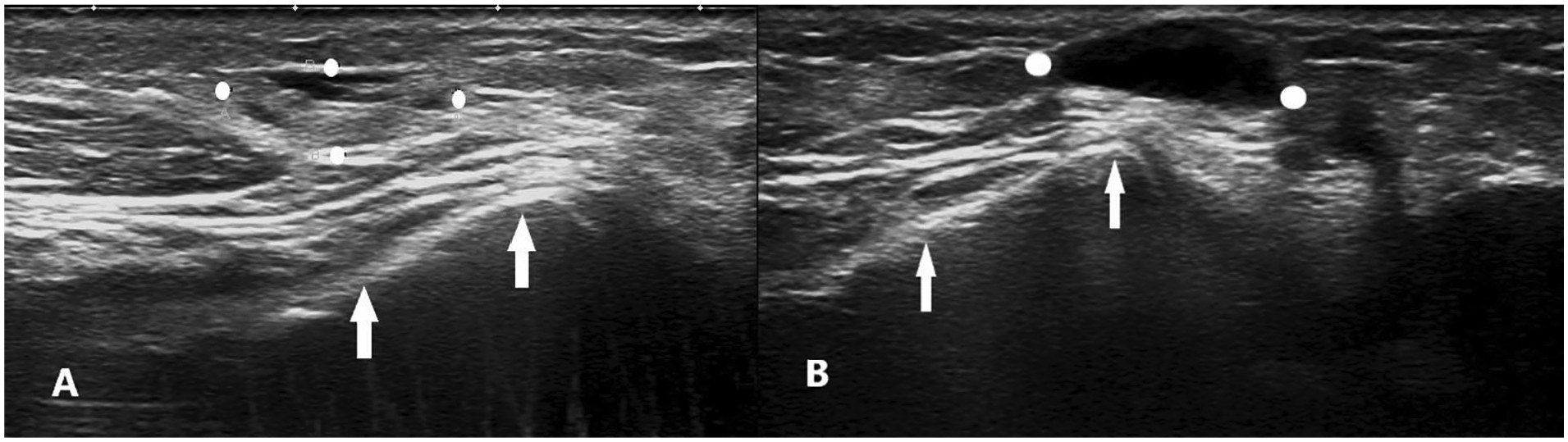
Longitudinal sonographic view on the ulnar side of the distal forearm: (A) 1 year prior: an hypoechoic inhomogeneous and poorly defined ovalar mass between the white dots and (B) current: an anechoic mass is visible between the white dots; distal ulnar epiphysis, white arrows.
The transverse sonogram, captured 1 year earlier (see Figure 2A), showed a poorly defined structure with hypoechoic and inhomogeneous internal structure, situated in the vicinity of the tendon of flexor carpi ulnaris, on its ulnar side. The current sonographic image (see Figure 2B) displayed the round aspect of the same mass, the same position, with an anechoic aspect and well-defined walls.
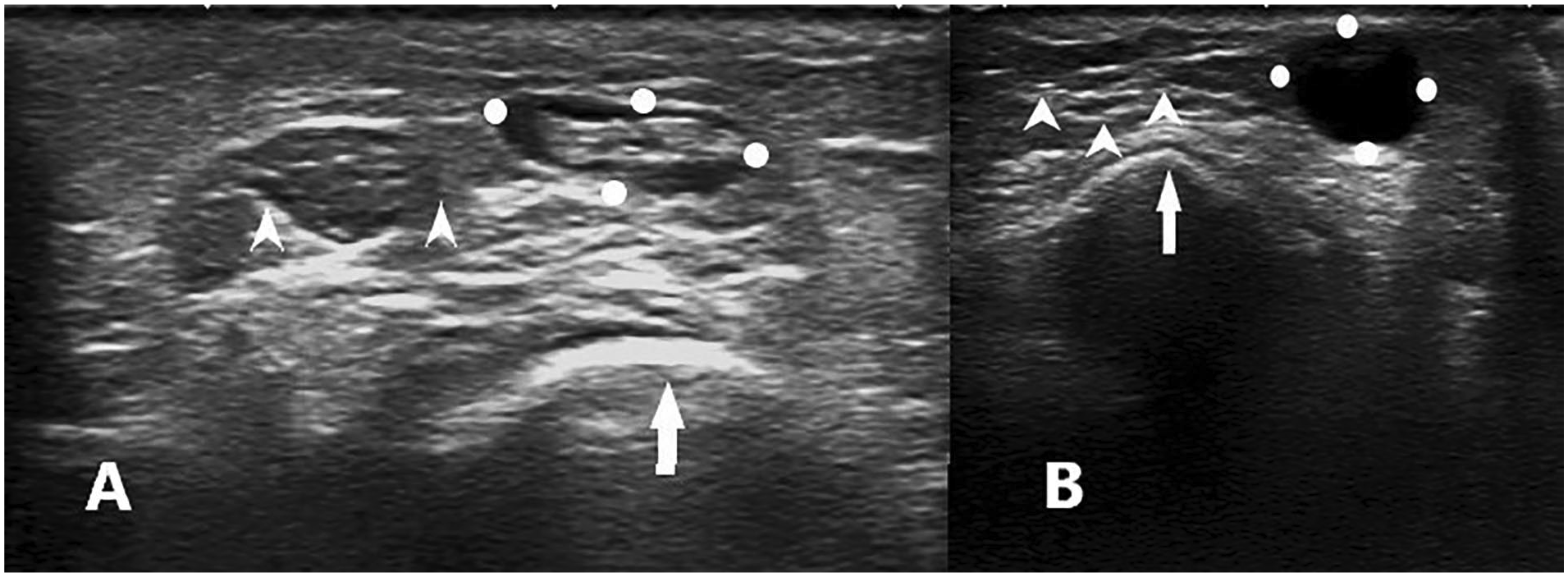
Transverse sonographic view on the ulnar side of the distal forearm: (A) 1 year prior: an ovalar, hypoechoic, inhomogeneous and poorly defined mass between the white dots and (B) current: a round anechoic mass is delimitated between the white dots; distal ulnar epiphysis, white arrow; flexor carpi ulnaris tendon, white arrowheads.
None of the current and previous color Doppler examinations displayed any signs of hyperemia.
Discussion
Bursae are synovial-lined sacs located at areas of friction to facilitate the gliding of tendons, ligaments, and muscles one over the other or over the bone. This is the definition of synovial bursae that are present at birth in certain anatomic locations. Inflammation of the bursa is called bursitis.
Apart from synovial bursae, there is another type of bursa, adventitial or adventitious, to develop in places where abnormal friction occurs. It is rather a pathological condition, as it becomes manifest only on special situations. Adventitious bursae represent mucoid and myxomatous degeneration of the connective tissue, with no endothelial synovial lining. The histologic process begins with the coalescence of small fluid spaces in the loose connective tissue. The walls differentiate from the adjacent tissue but they lack the mesothelial lining and the resulting cavity filled with fluid takes the ultrasonographic aspect of a well-delineated anechoic mass. The evolution of the adventitious bursitis over time is of interest for the clinician, as he may catch an intermediary aspect. The localization into the superficial connective tissue in areas with increased pressure or shear forces, the local signs and the sonographic appearance guide diagnostic and follow-up.
On a sonogram, bursitis appears as well-delineated and compressible fluid collection. Researchers have identified some unusual features for an adventitious bursitis and these are defined walls, with variable echogenicity, as well as the aspect of a tumoral superficial mass. 2 Clinically, it may remain asymptomatic or may be present as a painful mass.3-5
The most frequent areas for acquired adventitious bursae are the plantar aspect of the foot, over the stump of an amputated limb, at the superomedial and inferior angles of the scapula, on the lateral premalleolar surface of the ankle, and on the fibular aspect of the lower leg. 6 The adventitious bursitis of the plantar aspect of the foot is found on the calcaneal and the metatarsal heads fat pad, sites with increased friction and pressure forces. Runners, dancers, high heels, and longstanding exposed individuals are at risk. 7 Some adventitious bursae were found under chronic ulceration of the Charcot foot. 8
Sonography is an important tool in the diagnosis of different types of bursal abnormalities.
The clinical and imagistic evolution of an adventitial bursa is poorly discussed in the literature. Some adventitial bursitis may resolve spontaneously when ceasing the traumatic event or padding the involved area. It is the typical resolution of adventitial bursitis on fibular aspect of the lower leg.
For the diabetic foot, adventitial bursitis occurs frequently at the metatarsal heads and leads to ulceration. 9 There have been rare complications reported of an adventitial bursa of the foot, synovial chondromatosis. Synovial chondromatosis is a benign and rare synovial neoplasm affecting the large joints, originating from a synovial metaplastic process and producing cartilaginous and calcified loose bodies. There are only a few cases of synovial chondromatosis of the foot bursa localized near the first metacarpophalangeal joint. 10
Adventitious bursitis around scapulothoracic area affects the superomedial and the inferior angles and may produce painful scapular crepitus. Patients relate a history of trauma or overuse due to sport or work activities with constant movement of the scapula on the posterior thorax. The evolution may be chronic, with scarring and fibrosis. 11 Non-operative treatment consisting of rest, systemic non-steroidal anti-inflammatory drugs, activity modification, and shoulder rehabilitation should lead to resorbtion of the bursa. 12
This case was presented of a chronic adventitial bursitis with a mild clinical evolution, consisting in occasional pain of low intensity. The sonographic examination revealed the evolution into a cystic image, resembling more to a synovial bursitis, with clear anechoic structure and well-defined walls.
Based on a brief review of the literature, this was the only reported case of a cystic degeneration of an adventitious bursa. As it occurs at the site of abnormal friction between bone, superjacent soft tissue, and the hard-working table, it may be considered a professional condition. In case of missing the history of the patient, the occurrence of a cystic mass around the wrist would guide the differential diagnosis toward other conditions: ganglion, sarcoma, lipoma, hamartoma, abscess, and tumors. There are some reported cases of plantar fat pad adventitious bursitis that resembles a tumoral mass and the biopsy confirms the diagnosis. 2
The treatment varies from a conservative approach to a more invasive one. The conservative strategy aims at reducing the mass dimensions and inflammation, as lowering stress, padding, and physical therapy could be more efficient in the early stage. The cyst-like appearance is subject to needle evacuation, preferable on ultrasound guidance or open surgical evacuation.
Conclusion
A case study was provided of a patient with an adventitial bursitis on the ulnar margin of the distal forearm, as a result of prolonged pressure against a hard table. The bursitis evolved over 1 year into a cystic mass and had an important change of the sonographic features.
The actual discussion with the patient proposed two alternatives. The first alternative was a conservatory one, with proper local padding, a soft support for the wrist when working on the hard surface of the table. As the pain was intermittent and of low intensity, local non-steroidal anti-inflammatory drugs were recommended. She agreed to 10 days of physical therapy. The next follow-up visit was scheduled on 6 months if nothing unexpected would have happened. The second alternative was a more invasive, aiming at removing the cystic mass, either by evacuation of the content, that is, punctioning and aspirating it, or by surgical intervention. The patient declined this therapeutic alternative, at that time.
The importance of the presented case resides in clinical and therapeutical issues. The diagnosis of a solid mass in the subcutaneous tissue has to include an adventitial bursitis, even if the sonographic aspect is not the most typical one; it could be an unusual aspect or a transitory one, during the evolution toward a cystic appearance. Follow-up visits are necessary for mass description and therapy adjustments. The professional aspect of the mass occurrence is also important, as the underlying bones misalignment and longstanding pressure are predisposing to chronic evolution. As a consequence, the initial management is conservatory with padding and cushioning to relieve pressure, but on long term, the more invasive management should be considered, as the mass evolution may become complicated. The main complications to arise are increasing pain, infection, and fistulization. Follow-up diagnostic visits, at 6 months or when new events arise, would be considered mandatory.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.