
Abstract
Objective:
To study the utility of point of care ultrasound (POCUS) in the diagnosis and management of shock when performed by medicine residents.
Methods:
A retrospective, case-control study was carried out in the medical intensive care unit at a tertiary care hospital. Consecutive patients who had received bolus fluid for hypotension during the hospital stay were screened from the case sheets and recorded.
Results:
A total of 57 patients were recruited into the study. Baseline parameters were comparable in both groups. The median amount of fluid given by the physician was 1000 milliliters (500, 1500) in the inferior vena cava (IVC) group as compared with 1000 milliliters (500, 1000) in the clinical group which was similar between the groups (P = .51). The median quantity of fluid received in the first hour in the IVC group (500 milliliters; 75, 750) was significantly higher than in the clinical group (100 milliliters; 100, 125) (z = 2.98; P = .003). More improvement in heart rate (P = .0004), mean arterial pressure (MAP; P = .04), and Acute Physiology and Chronic Health Evaluation (APACHE; P = .0004) score was seen in the IVC group which was statistically significant.
Conclusion:
In this cohort, there was a significant increase in MAP, reduction in the APACHE II score, and heart rate in the IVC group when compared with the clinical group.
Point of care ultrasound (POCUS) has been defined as portable ultrasonography brought to the patient and performed “real time” by the provider. Recently, the use of POCUS has dramatically expanded in the areas of critical care, surgery, and emergency medicine.1–3 Because of the noninvasive nature of sonography and the feasibility to perform repeated quick assessment in sick patients, this modality has become the frontline diagnostic tool for emergency care.4–7 Point of care ultrasonography is increasingly being used to assess the fluid status of patients by measuring the inferior vena cava (IVC) diameter. Hence this retrospective study was conducted to determine the change in outcome with fluid management in patients where the IVC was assessed sonographically by postgraduate medical residents compared with those where fluid management was done on clinical grounds.
The aim was to study the utility of POCUS in the diagnosis and management of shock when performed by medicine residents. The attempt of this work was to achieve this by estimation of fluid given during resuscitation along with change in clinical parameters like the Acute Physiology and Chronic Health Evaluation (APACHE II) score and mean arterial pressure (MAP).
Methods
This retrospective case-control study was conducted at the All India Institute of Medical Sciences, New Delhi, India India. The institute provided ethical clearance for this particular research. The study was conducted using the data extracted from the medical records of admitted patients over a period of 1 year, August 2017 to August 2018.
Study Population
Study population was obtained from the medical records of patients admitted to the hospital’s department of medicine. The sample included patients admitted to the intensive care unit (ICU). A sample size of convenience was chosen with a total of 60 patients being enrolled. Inclusion criteria included hypotension at presentation or any time during the hospital stay, for which intravenous fluids were administered as initial resuscitative measure. Only those records complete with the required data were included in the study.
Exclusion criteria for recruiting patients included the following: prior abdominal procedures, abdominal sutures, pregnancy, history of cardiac disease, history of chronic lung disease like interstitial lung disease, history of chronic kidney disease, patients with acute kidney injury with reduced urine output, and patients admitted due to trauma.
Training
The medical residents within the department are trained in using the ultrasound machine at the inception of their residency. This training includes didactic sessions on the parts and working of the available machine. This is followed by practice of point-of-care sonographic techniques on clinically stable patients to identify and measure appropriate structures. This is done until the resident was confident in performing a rapid sonographic assessment of a patient. The measurement of the IVC is done using either the curvilinear probe or the phased-array probes, per the convenience of the resident.
IVC Measurement
The probe is placed over the epigastrium in the midline or slightly to the right with the transducer or marker pointing in the cephalad direction. The IVC is recognized as a horizontal collapsible vessel traversing the liver and draining into the right atrium. On this path, the IVC receives the hepatic vein as a tributary. The measurements of the IVC are carried out in its intra-hepatic part, 2 cm distal to the opening at the right atrium or 1 cm distal to the junction of the hepatic vein. Once identified, the measurements are classically made using M-mode imaging. Figure 1 depicts a still image of the M-mode tracing of the IVC at the point of interest as described above. During M-mode imaging, the largest diameter (IVCmax) is obtained during quiet expiration while the smallest diameter (IVCmin) is obtained during spontaneous deep inspiration.
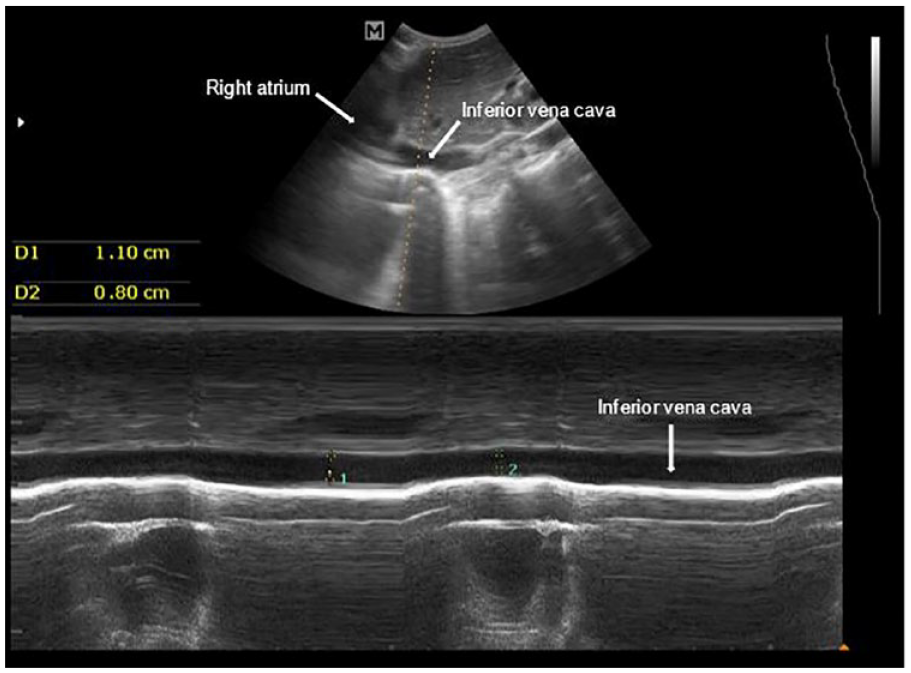
M-mode image of the IVC at the point of interest. The IVC and right atrium have been marked by white arrows. The maximum IVC diameter (IVCmax) is represented by Measurement 1 (D1), and the minimum IVC diameter (IVCmin) is represented by Measurement 2 (D2). IVC, inferior vena cava.
The IVC shows respiratory variation due to varying intrathoracic pressures. During inspiration, the negative intrathoracic pressures draw blood from the abdominal veins into the right side of the heart, this shift of blood leads to a collapse of the IVC during inspiration. It has consistently been found that if this collapse is >50% of the diameter of the IVC during expiration, it correlates to a central venous pressure of <5 cm of water, indicating hypovolemia.
Patient Categorization
The records included in the study were divided into two groups: the IVC group and the clinical group.
The IVC group participants had medical records that indicate hypotension was assessed initially using collapsibility index of the IVC. This was calculated as given in the formula below, with maximal diameter (IVCmax) being the largest IVC diameter attained during quiet expiration. The minimum IVC diameter (IVCmin) was the smallest IVC diameter measured during spontaneous deep inspiration by the patient. Intravenous fluids (at the resident’s discretion) was administered if the patient was considered to be volume responsive (IVC collapsibility index > 50%). This was continued with regular IVC assessment until the IVC collapsibility index was <50%, or until hypotension resolved; whichever criteria was met earlier.

The clinical group participants included those medical records indicating that intravenous fluids were administered for hypotension without the use of sonography (at the resident’s discretion). This was continued until a maximum volume of 30 milliliters/kg of fluids or until hypotension resolved; whichever criteria was met earlier.
Data
Data were extracted into a predesigned proforma managed on a Microsoft excel database. The baseline characteristics and admitting diagnosis of the patients were extracted to determine inclusion into the study. This was followed by collection of vital parameters and APACHE II score before and within 60 minutes of fluid resuscitation. Details regarding type of intravenous fluids, fluid quantity, and rate were also documented. The primary outcome was change in blood pressure, MAP, respiratory rate, heart rate, and APACHE II score (pre- and post-resuscitation) in the two groups.
Statistical Analysis
Statistical analysis was performed using Stata v.12.0 (StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP). Normality of data was assessed. Normal data are represented as mean (standard deviation), while skewed data are presented as median (interquartile range). Independent group student t test was used to compare normally distributed data. Skewed data were compared using the Wilcoxon Rank-sum test. Significance was considered at an alpha of .05 and a confidence interval of 95%.
Results
Over the year of data collection, a total of 57 medical records were included in the study. This included 27 patients in the IVC group and 30 patients in the Clinical group. 61.4% of the study population were males. Median age of the study population was 50 years (31, 65). The patient characteristics and the baseline clinical characteristics were comparable between the two groups as depicted in Table 1. The mean heart rate, however, was significantly higher in the IVC group when compared with the Clinical group (t = 2.55; P = .01).
Baseline Characteristics in the IVC Group and Clinical Group and Differences Between the Groups.
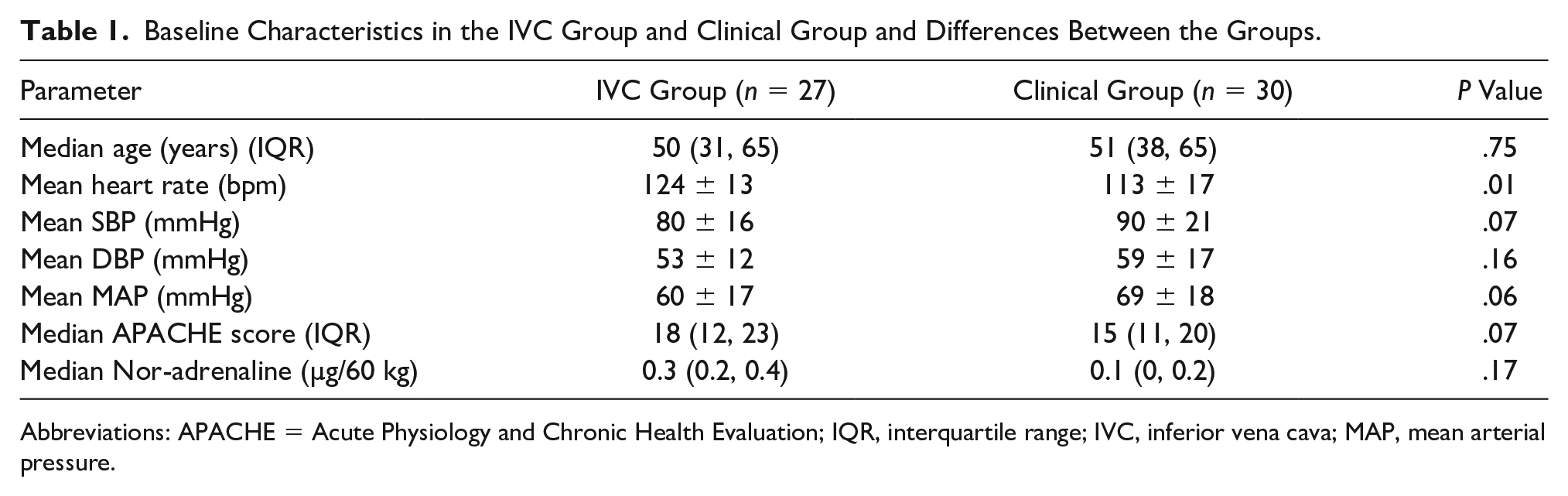
Abbreviations: APACHE = Acute Physiology and Chronic Health Evaluation; IQR, interquartile range; IVC, inferior vena cava; MAP, mean arterial pressure.
The intervention and post-intervention parameters are depicted in Table 2. There was no significant difference between the median amount of fluid given between the two groups which was 1000 milliliters (500, 1500) in the IVC group compared with 1000 milliliters (500, 1000) in the clinical group (z = 0.65; P = .51). The median quantity of fluid received in the first hour in the IVC group (500 milliliters; 75, 750) was significantly higher than in the clinical group (100 milliliters; 100, 125) (z = 2.98; P = .003). Both groups received similar median dosages of vasopressors (noradrenaline); 0.3 µg/60 kg (0.2, 0.4) in the IVC group compared with 0.1 µg/60 kg (0, 0.2) in the clinical group (z = 1.86; P = .06).
Amount of Fluid Given and Change in Clinical Parameters Post-Intervention in the IVC Group and the Clinical Group.
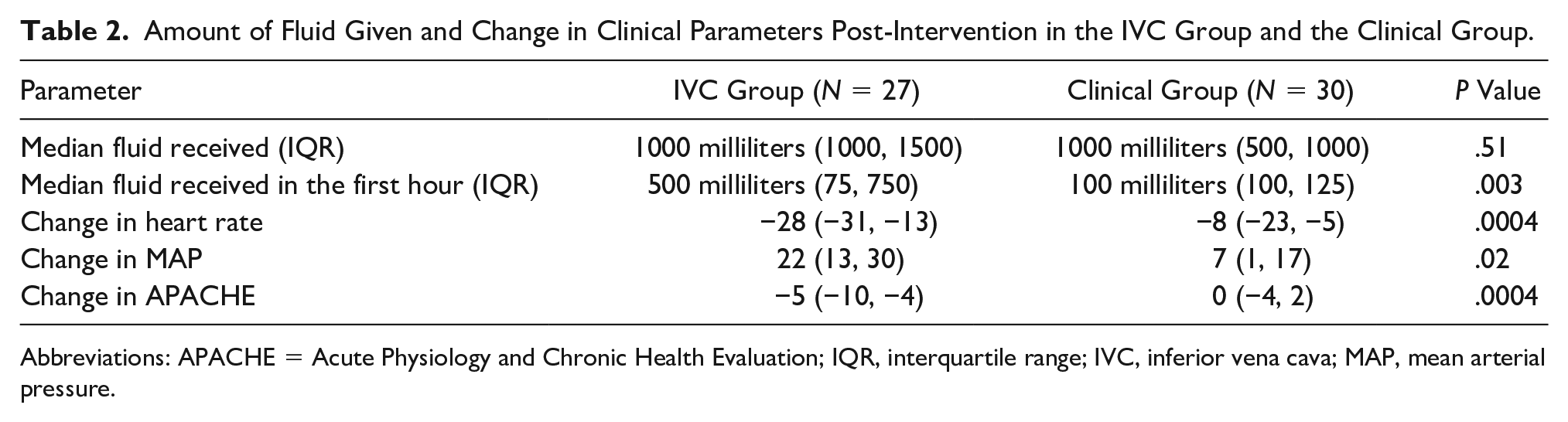
Abbreviations: APACHE = Acute Physiology and Chronic Health Evaluation; IQR, interquartile range; IVC, inferior vena cava; MAP, mean arterial pressure.
Figure 2 illustrates the change in clinical parameters post-intervention. The fall in heart rate after fluid administration was 28 bpm (13, 31) in the IVC group in comparison with 8 bpm (5, 23) in the clinical group (z = 3.5; P = .0004) which was statistically significant. The rise in MAP was 22 mmHg (13, 30) in the IVC group in comparison with 7 mmHg (1, 17) in the clinical group which was statistically significant (z = 2.36; P = .02). The observed decrease in APACHE II score in the IVC group was 5 points lower (4, 10) after fluid administration when compared with the clinical group which was 0 points (−2, 4) which was statistically significant (z = 3.52; P = .0004).
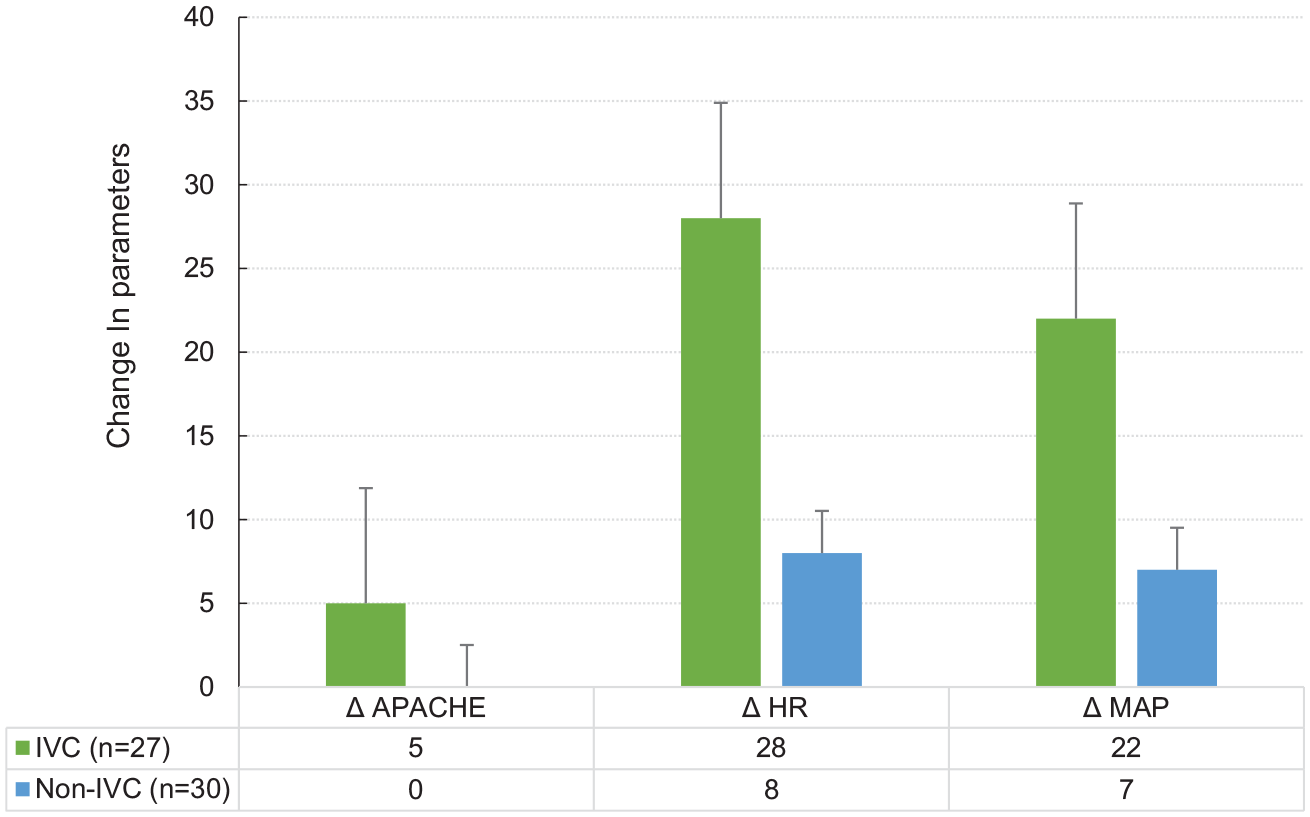
Bar graph depicting the change in heart rate, MAP, and APACHE score post-intervention in the IVC group (green bar) and the Non-IVC group (clinical group) (blue bar) with the error bar depicting standard error. APACHE = Acute Physiology and Chronic Health Evaluation; IVC, inferior vena cava; MAP = mean arterial pressure.
Discussion
Point of care sonography has gained impetus as an aid for assessment and management of patients in various specialties such as critical care, emergency medicine, and medicine. Internal medicine residents desire sonography training, but self-reported competence is low. 8 Several studies have shown that after brief training, residents can become competent in performing and interpreting basic sonographic examinations. However, most studies focus on a limited number of findings or very specific settings such as the ICU and have involved small numbers of residents.9–11 Others have shown that even after extensive practice, residents’ competence in performing and interpreting sonograms is poor. A study conducted by Henneberry et al has emphasized on the pivotal role played by point of care sonography done by emergency physicians in emergency department for management of variety of medical and traumatic conditions. 6 A randomized controlled trial conducted by Jones et al has shown the importance of an early goal directed sonogram, for patients with non-traumatic hypotension, in decreasing time to a final diagnosis, in the emergency department. 12 Caronia et al trained medical residents with a 2-hour module, in focused vascular sonography, for assessing the compressibility of common femoral and popliteal veins. 13 They concluded that demonstration by medical residents had substantial agreement with radiologists, for the diagnosis of a deep venous thrombosis (DVT), after a 2-hour course. 13 However, it is well acknowledged that point of care sonography is different from the sonography performed by radiologists, hence it is not meant to replace the use of comprehensive diagnostic imaging studies. The above-mentioned study was carried out for evaluation of the skills of medical residents in performing bedside sonography. It also reported on the effect of fluid management for critically ill patients and the assessment of IVC diameter.
In the current study cohort, there was no significant differences in the baseline characteristics between the IVC and the clinical group, barring a higher heart rate in the IVC group. There were no significant differences in the fluid administered or the vasopressor doses between the two groups. The amount of fluid given to the patients in the IVC group in the first hour was significantly higher than in the clinical group. There were six patients in the IVC group who were correctly identified as having a predominant cardiogenic shock. In this group, fluids were administered at a lower rate for those patients. Post-intervention, there was a significant increase in the MAP, along with a significant fall in the heart rate and APACHE II score in the IVC group when compared with the clinical group. Shock and its management is a dynamic process with the improvement in shock occurring because of factors other than the amount of fluid administered. This includes the rate of fluid administration, regular monitoring, and concomitant vasopressor administration. Thus, although the total fluid administered between the groups were similar, the fluid administered in the initial 1 hour yields the significant difference in the clinical parameters seen in this cohort. This is possibly based on the accurate assessment of fluid status by the IVC measurements.
The study emphasizes the use of bedside sonography by trained medicine residents in improving the fluid management of patients, by IVC assessment. IVC measurement is a simple tool that can guide the fluid management of the patient. IVC measurements may be performed using minimal training. In the setting of shock, the IVC can guide physicians regarding fluid management. A collapsibility index of >50% would indicate either hypovolemic or septic shock which would require aggressive fluid management. An IVC collapsibility of <50% in the presence of shock would indicate the presence of cardiogenic or obstructive shock in which case overzealous fluid administration would be detrimental to the patient’s condition. No prior study has been performed addressing this topic which holds importance in the sphere of management of critically ill patients, by medical residents.
Limitations
The limitations of this study are based on the design of a retrospective study and interobserver variation for conducting sonography. The sample size of this study was based on the documentation available during the study period. It is understood that the sample size is small and the results should be interpreted in the context of potentially skewed results, given the small number of patients.
It will be important to confirm these findings with prospective studies that have larger sample sizes. Furthermore, it would be important to design studies that not only train new residents but also describe the amount of training required to perform these measurements, with reasonable certainty.
Conclusion
There was a significant increase in MAP, and reduction in the APACHE II score and heart rate in the IVC group when compared with the clinical group, in this cohort. This comes irrespective of the amount of total fluid administered representing the importance of rate of fluid administration and the frequent and accurate monitoring using sonography.
Footnotes
Ethics Approval
Ethical approval was taken from the institutional ethics committee prior to the start of the study.
Informed Consent
Informed consent of the participants was not applicable as this was a retrospective study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
Trial registration for this study is not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.