
Abstract
Objective:
The Radiology department played a crucial role in detecting and following up with the COVID-19 disease during the pandemic. The purpose of this review was to highlight and discuss the role of each imaging modality, in the radiology department, that can help in the current pandemic and to determine the challenges faced by staff and how to overcome them.
Materials and Methods:
A literature search was performed using different databases, including PubMed, Google scholar, and the college electronic library to access 2020 published related articles.
Results:
A chest computed tomogram (CT) was found to be superior to a chest radiograph, with regards to the early detection of COVID-19. Utilizing lung point of care ultrasound (POCUS) with pediatric patients, demonstrated excellent sensitivity and specificity, compared to a chest radiography. In addition, lung ultrasound (LUS) showed a high correlation with the disease severity assessed with CT. However, magnetic resonance imaging (MRI) has some limiting factors with regard to its clinical utilization, due to signal loss. The reported challenges that the radiology department faced were mainly related to infection control, staff workload, and the training of students.
Conclusion:
The choice of an imaging modality to provide a COVID-19 diagnosis is debatable. It depends on several factors that should be carefully considered, such as disease stage, mobility of the patient, and ease of applying infection control procedures. The pros and cons of each imaging modality were highlighted, as part of this review. To control the spread of the infection, precautionary measures such as the use of portable radiographic equipment and the use of personal protective equipment (PPE) must be implemented.
In December 2019, a massive outbreak of a novel severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) infection occurred, in Wuhan, Hubei province China. The World Health Organization (WHO) was widely alerted about a severe pneumonia, of unknown origin, by the Public Health Commission, of Hubei Province, China. 1 By January 2020, Chinese scientists had isolated a novel coronavirus from patients infected with the viral pneumonia. The pathogen was identified to be a novel enveloped RNA beta-coronavirus. 2 The new coronavirus was identified as SARS-CoV-2, by the International Committee on the Taxonomy of Viruses. 3 The reason for this name is the similarity of its phylogenetic compared to the formerly isolated SARS-CoV. 2 The WHO designated it as coronavirus disease 2019 (CoVID-19), later in February 2020. 3 Following this, there has been a marked rise in the exponential growth of COVID-19 infections spreading rapidly from China’s neighboring countries such as Japan and South Korea. Eventually, it spread to other countries such as the United States, Europe, and Africa. Toward the end of January 2020, the WHO declared COVID-19 an epidemic and a global emergency. On March 10, 2020, the WHO declared COVID-19 as a pandemic disease following its deadly explosion in Italy. 1
The novel SARS-CoV-2 virus was ranked as the seventh human-related pathogenic coronavirus. After SARS-CoV and Middle East Respiratory Syndrome coronavirus (MERS), SARS-CoV-2 was the third pathogen with a predilection for causing deadly pneumonia. In addition, infections resulting from coronavirus disease are highly communicable. However, COVID-19 associated death rates are relatively low; about 1.0% to 3.5%, with geriatrics as an exception and specifically those over 70 years of age with comorbities. 4 According to a report published by the Chinese Center for Disease Control and Prevention, it has been estimated that: (a) About 5% to 10% of the people infected with COVID-19 need critical care because of severe respiratory dysfunction or extra-pulmonary organ failure, (b) around 15% to 20% can develop severe pneumonia, and (c) 80% of patients can develop mild symptoms. Among intensive care unit (ICU) patients, COVID-19 has been linked to death rates between 30% and 70%. 5
In addition, the SARS-CoV-2 virus is highly transmissible. The virus transmission mainly occurs through aerosol droplets. 1 According to a study carried out by D’Andrea et al, 1 infected human beings are the primary source of infection. Notably, infections can spread through asymptomatic human carriers as well.
The SARS-CoV-2 infection occurs with a broad base of clinical presentation ranging from asymptomatic to displaying severe symptoms that may require endotracheal intubation. 5 Likewise, infected symptomatic adults mainly present with high fever and dry cough. 6 For severe COVID-19 cases and deaths, some of the commonly reported risk factors were identified to include older people (>70 years), males, and preexisting medical conditions such as hypertension, atherosclerosis, diabetes, cancer, respiratory or chronic kidney disease. 5 Additionally, mild cases of COVID-19 can usually imitate upper respiratory viral infections. However, as the disease progresses, dysfunction of the respiratory system becomes the primary source of mortality and morbidity. 7
Clinical Imaging and COVID-19
Due to the relatively low testing sensitivity of real-time reverse transcription-polymerase chain reaction (rRT-PCR) tests (60%-70%) and the global shortage of resources, as has been described by reports from China, an increase in medical imaging strategies were needed to detect and diagnose patients, with COVID-19. 8 Accordingly, imaging of the chest played an essential role in detecting COVID-19, mainly at the early stage with a negative rRT-PCR test. Therefore, strengthening the recognition of image alterations was an essential step in helping clinicians to accurately and quickly diagnose the disease. 9
Even though differentiating other viral pneumonia from COVID -19 pneumonia with computed tomography (CT) is challenging and complex, 9 CT imaging had a sensitivity of 97% and was considered an essential early detection modality. This was particularly true for patients suffering from persistent clinical suspicions of COVID -19, despite a negative RT-PCR test. 8
Lately, the Chinese Critical Care Ultrasound study group and the Italian Academy of Thoracic Ultrasound proposed that the lung ultrasound (LUS) be considered a precise and adequate tool to identify lung involvement, in patients with COVID -19 and in pregnant women. The advantages of LUS as a non-ionizing and safe diagnostic choice allows for multiple images to be taken during pregnancy and has low risk compared to other imaging modalities. 10
Furthermore, a study has suggested that the use the ultrashort echo time (UTE) technique in magnetic resonance imaging (MRI) can be an alternative to CT, especially as a non-invasive evaluation of COVID-19 patients. 11
Encountered Radiology Department Challenges
Although medical imaging played an essential role during COVID-19, the radiology department was expected to face challenges and difficulties during the outbreak. The disease is highly contagious, and the need to prevent cross-infection between patients and hospital staff was difficult. It is not surprising that deaths among physicians, nurses, and even radiographers were widely reported. 12
The purpose of this review was to investigate and understand the radiology department’s role during the outbreak by discussing different imaging modalities benefits in detecting and diagnosing COVID-19 patients. It was also important to determine the challenges and difficulties encountered by the radiology department during the pandemic. This was achieved by carefully reviewing the latest published articles, related this topic from various databases.
Materials and Methods
In this review, published articles from 2020 and different databases included: PubMed, Google scholar, and the college electronic library were identified and collected. Search terms such as, COVID-19, coronavirus, radiology, radiography, role, challenges, importance, difficulties, CT, MRI, chest X-ray, and ultrasound were used to find related articles. Furthermore, the keywords included abbreviations for each modality: CT, MRI, and the US. Only articles that discussed the diagnostic role of different imaging modalities to detect COVID-19, challenges faced by the radiology department, and issues related to the infection control, were included in this review.
Results
CT and COVID-19
Most of the articles found in the literature focused on the use of CT in diagnosing COVID-19 patients. The results of these articles were categorized into 3 main findings; the CT lung appearance of COVID-19 patients, specificity and sensitivity of CT, and the comparison between CT and rRT-PCR test.
CT Lung Appearance of COVID-19 Patients
Ground-glass opacities (GGO) and lung consolidation were reported in several articles as imaging features within COVID-19 patients.3,9,13–22 Furthermore, in COVID -19 patients, a “crazy-paving” pattern, vascular enlargement, and air bronchogram were observed.9,13–16 The CT images revealed additional signs of COVID-19 such as thickened interlobular septa and intralobular lines superimposed on diffuse ground-glass attenuation, known as “crazy paving pattern. 3 Besides the “crazy-paving pattern,” added diagnostic signs were air trapping, reverese halosign, 3 batwing sign, white lung sign, and the Rosa roxburghii sign. 17 Figures 1–3 show the difference between COVID-19 chest CT imaging features.
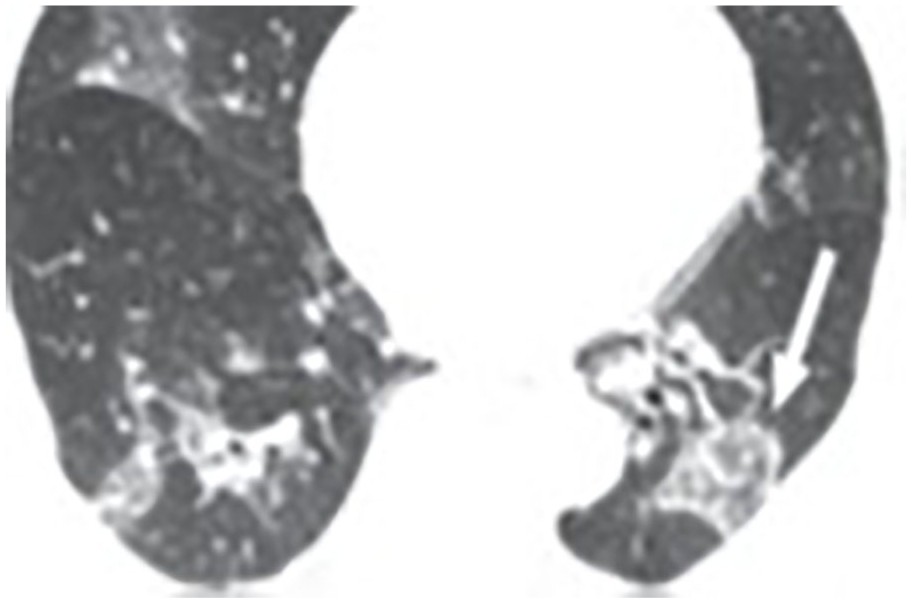
An axial section of chest computed tomogram of a 68-year-old male. The chest scan displays reverse halo sign in the lower lobe of left lung (arrow in white). 3
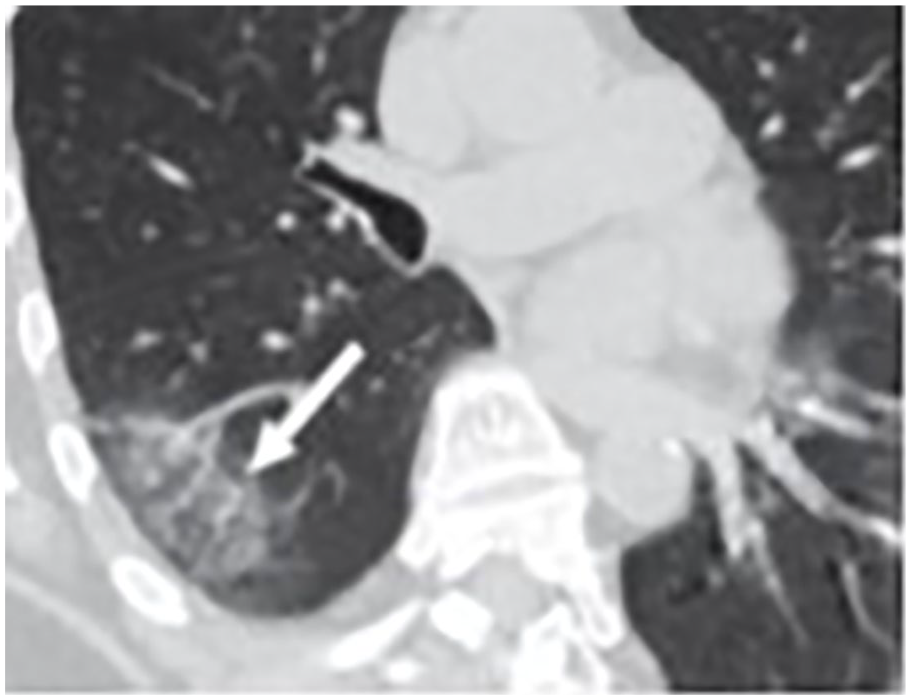
An oblique axial section of chest computed tomogram of a 61-year-old female. The image shows ground-glass opacities with vascular enlargement (arrow in white). 3

An axial section of chest computed tomogram of a 77-year-old female demonstrating multiple ground-glass opacities and consolidation in addition to thickening of interlobular septum (arrow in white). Air trapping and air bronchogram signs are shown (arrow in black). 3
Correlation Between CT Findings and COVID-19 Progression
ICU patients had more documented “crazy–paving patterns,” bronchus distortion, bronchiectasis, air trapping, and mediastinal and hilar lymph node enlargement than those patients not admitted to the ICU and discharged. 16 Furthermore, in severe COVID-19 cases, the chest CT revealed flaky or widespread lesions. 18 As a result, a chest CT can differentiate the stages of a lung lesion based on consolidation and disease extent. According to a clinical study, 30 patients were found to be in the early stage, 49.1% of 110 cases were in the progressive stage and 26 patients were in a severe category. For chest CT follow-up patients, 12 out of 16 (75%) showed disease progression, 25% of 16 patients had mild disease progression, and 5 had moderate disease progression. 17 CT findings in these patients revealed that disease extent was minimal in 2 patients, moderate in 4 patients, and severe in 2 patients. In addition, the clinical severity of the patients was determined. On CT, approximately 68% of patients in critical condition had 25% lung parenchyma involvement, while 26% of patients were not classified as severe cases. 19
CT Detection of COVID-19 Lung Lesion Involvement
A CT on 51 patients revealed that most of the patients (74.5 %) had an infection in all 5 lobes of the lung, while the remaining patients had an infection in other lobes individually or bilaterally. 3 Furthermore, in 43.6% of 110 patients, CT detected peripheral lung lesions, and in 56.4% of cases it detected lesions in both the central and peripheral zones. Approximately 5.5% of the 110 patients had multiple lung lesions, while 9.1% had individual lobe lung lesions. The majority of the patients (72.7%) had lesions in multiple lobes of the right and left lung. 17 The distribution of pulmonary lesions on CT in COVID-19 patients at various disease symptoms was mainly at the periphery, with only a few patients having central lesions. 13
Accuracy, Sensitivity and Specificity of COVID-19 Chest CT
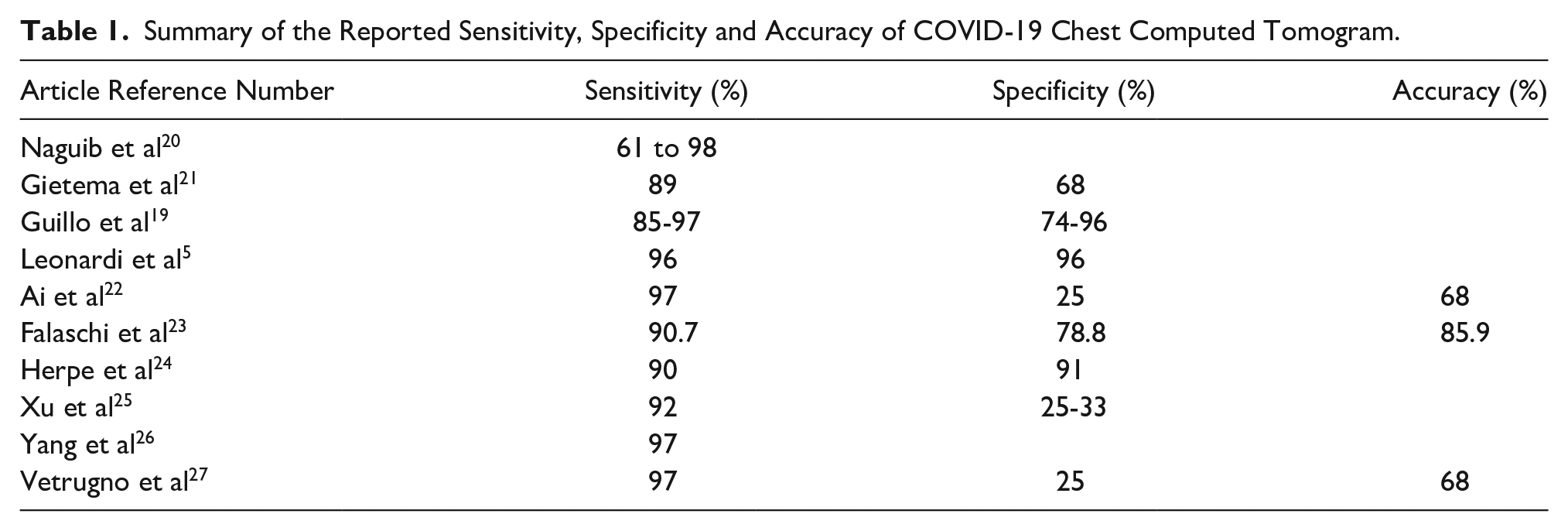
Several articles have reported the accuracy, sensitivity, and specificity of CT in detecting COVID-19 disease. Most of the studies demonstrated acceptable levels for the detection of COVID-19 (See Table 1).
Summary of the Reported Sensitivity, Specificity and Accuracy of COVID-19 Chest Computed Tomogram.
CT vs. rRT-PCR Test
Several studies have reported symptomatic patients with false-negative rRT-PCR test results. However, chest CT images
Furthermore, in comparison to rRT-PCR, CT can be used as a reference test to classify patients as positive or negative COVID-19 cases, since CT is a quick and reliable triage tool. It also produces a report in less time than the rRT-PCR. 31 Additionally, a CT severity score can be used as a diagnostic predictor for those patients who are not elderly patients. Similar imaging may be useful in diagnosing patients who are highly suspected of having COVID-19. 32 Moreover, correlating dynamic changes seen on a CT of the lung with laboratory test results could provide more information and help in the diagnosis and treatment of COVID-19 patient. 33 Furthermore, the utility of CT was further noted in distinguishing COVID-19 from other viral types of pneumonia. It also provided rapid diagnostic results as to whether patients were COVID-19 positive or negative, based on CT image features.34,35
Comparison Between COVID-19 CT and Radiography
Performing CT throughout the pandemic is challenging and a complex task, due to the disinfection procedure and the high radiation patient dose, specifically, for young patients. 36 The ACR also stated that the decontamination process required after imaging COVID-19 patients might disrupt the availability of radiologic services. Furthermore, the ACR does not recommend using a CT for COVID-19 patients unless they are symptomatic and have clinical indications. 37 Hence, the medical community relied on the portable chest radiograph (PCXR) as another diagnostic option for identifying and following up with lung abnormalities. However, this dependent on equipment availability and reduced infection control procedures, compared to CT. 38 However, the use of PCXR in early stages of COVID-19, was not recommended due to the low specificity and sensitivity for patients with a mild disease. 39 In these cases, a CT is the most valuable imaging modality for the early stages of COVID-19. 39 Therefore, CT is considered the standard imaging modality for assessing lung involvement. 10
Although a chest radiograph (CXR) is a faster and more widely available instrument for evaluating lung parenchyma, but a chest CT is considered a better option, due to its higher sensitivity. 37 A recent study showed that the CXR of 4 patients resulted in a negative report, without any sign of abnormality. Unfortunately, the chest CT showed some COVID-19 imaging features, such as GGO, crazy paving pattern and consolidation. 37 Figure 4 shows a 37-year-old male patient with a normal CXR and an abnormal chest CT and was 1 of the 4 cases reviewed.
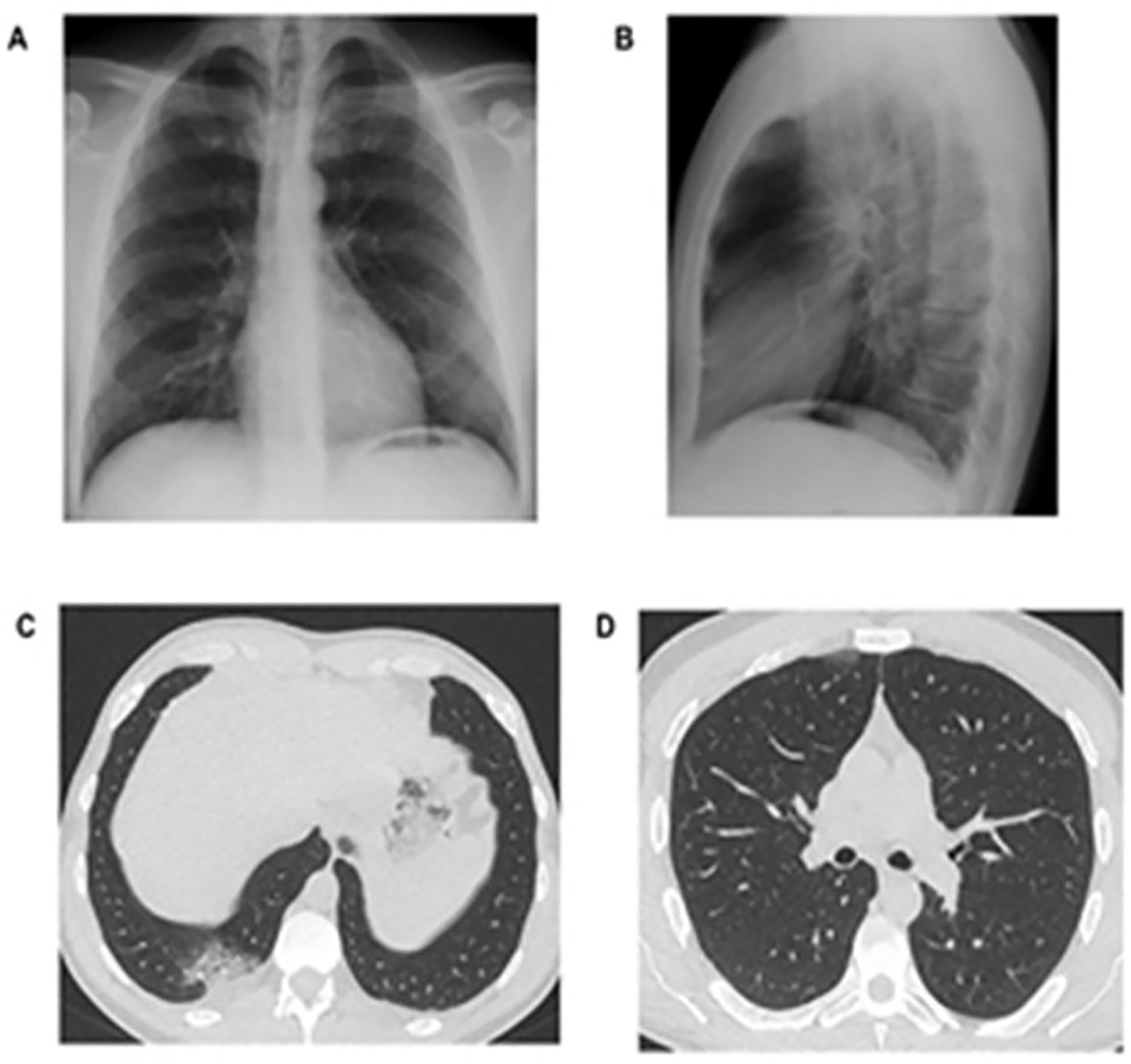
Posterior-anterior. (A) and lateral (B) images of chest radiograph of a 37-year-old male patient. The chest radiograph did not show any signs of abnormalities. (C & D) are axial chest CT. Image (C) demonstrates the “crazy paving pattern,” in the right posterior costophrenic recess with mild pleural effusion. Image (D) shows that anteriorly in the right upper lobe there is small subpleural area of ground-glass opacity. 37
Sonography and COVID-19
Although CT is considered the primary imaging modality in diagnosing COVID-19, not all patients qualify, such as pregnant and pediatric patients. For this reason, several articles have demonstrated the potential of lung sonography in diagnosing COVID-19 patients, as an alternative diagnostic tool.
Sonographic Lung Appearance of COVID-19 Patients
In a case study, the sonographic findings of 3 COVID-19 pediatric patients revealed signs of coalescing and scattered B-lines, pleural effusion, irregularities in the pleural line, and consolidations. 40 Another study addressed the findings of a lung sonogram (LUS), performed on confirmed COVID-19 pediatric patients. LUS displayed typical B-lines indicating abnormalities, consolidation, and GGO in the right lung, and contralateral A-lines in the lower region of the left lung. Improvement in symptoms was documented on the LUS as B2-lines transitioned to B1-lines and then to A-lines. 41
Furthermore, the most common signs observed in LUS for COVID-19 adult patients were B-lines, irregular pleural lines, thickened pleural lines, and consolidation.41–50
Another study stated that the most common LUS findings in 10 pediatric patients were vertical B-lines, white lung sign, pleural irregularities, and subpleural consolidation. As a result, LUS was an essential imaging tool in determining moderate and severe COVID-19 pneumonia. 44 Figures 5–7 illustrate how LUS can demonstrate different COVID-19 imaging features.
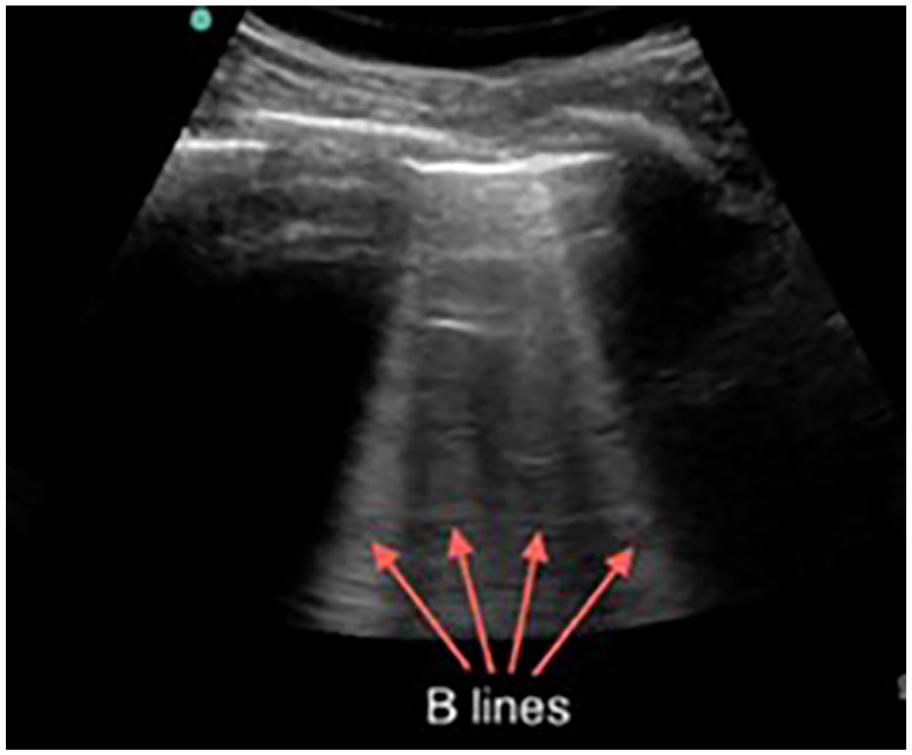
An example lung ultrasound that shows B-lines (vertical artifact). 44
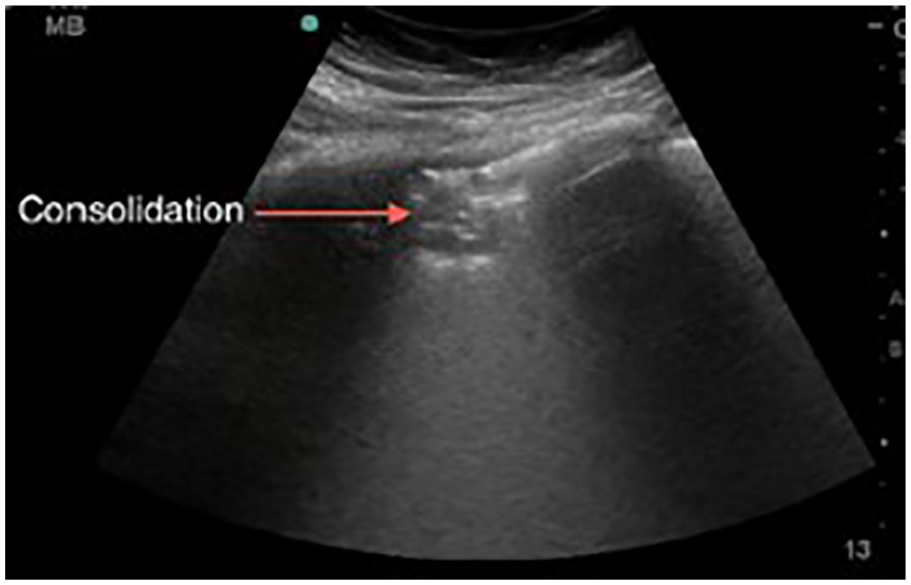
This lung ultrasound image shows a small consolidation in the anterior area with indistinct margins. 44
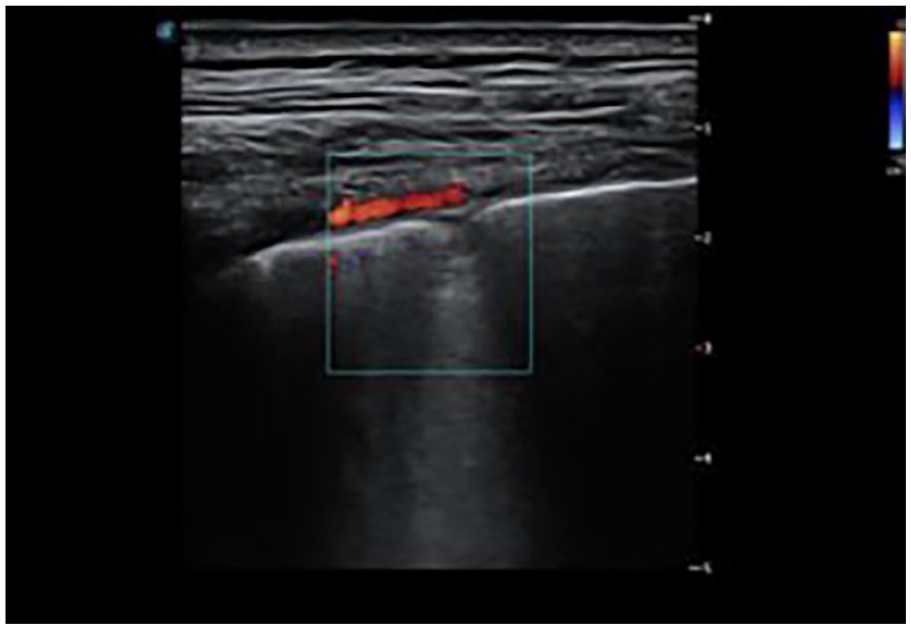
This lung ultrasound shows fixed B-lines, with interrupted pleural line and patchy consolidation. 44
LUS and Pregnant COVID-19 Patients
LUS, as a radiation free modality, can be used to safely image a pregnant COVID-19 patient. A published study of a pregnant COVID-19 patient revealed diffuse and thick B-lines on either side of the lungs and had basal posterior involvement. 44 Another study of 4 pregnant women with COVID-19 reported lung involvement with sonography. On LUS, all 4 patients had COVID-19 pneumonia which included irregular pleural line, white lung, large subpleural consolidations and multiple vertical artifacts. 10
Correlation Between COVID-19 LUS and CT
A study has compared COVID-19 chest CT findings with LUS. Five of the 29 patients (17%) showed a “white lung” with LUS, which is correlated with the “crazy paving pattern” of GGO, on a CT. 42 Furthermore, it was reported that a higher aeration score on LUS was associated with advanced and extreme stages of the disease on chest CT. 43 Accordingly, the LUS score can differentiate the impaired regions of the lung that contribute to hypoxemia by different impairments of aeration, vasoconstriction, and shunt. 50
Comparison Between COVID-19 LUS and Radiography
In a retrospective study of 43 patients, the sensitivity of sonography was compared to the sensitivity of a chest radiograph, in diagnosing COVID-19. LUS was shown to have a sensitivity of 88.9% and specificity of 56.3%. On the other hand, a CXR had a sensitivity of 51.9% and specificity of 75.0%. 51 Another study found that LUS had a sensitivity of 94% and specificity of 89%. 46 Also, a study on 24 patients compared the results of chest sonogram with a CXR. On the chest sonogram, 94% of patients with respiratory symptoms demonstrated lung abnormalities. 52
Additionally, it was reported that LUS could play a vital role in the pandemic because of its high sensitivity in detecting peripheral pulmonary changes. 53 Furthermore, LUS was found to be superior to CXR in detecting COVID-19 pneumonia.54,55 Besides, LUS has been shown to be superior to a chest CT in detecting smaller peri-pulmonary lung lesions as well as pleural and peri-pulmonary effusion.44,46,50
Lung Sonogram vs. Portable Chest Radiograph
A study was conducted on 11 patients who had a negative COVID-19 based on a nasal swab result. All participants had abnormal sonogram and CXR. Nine out of the 11 patients had typical findings of COVID-19 on a LUS. B-lines were noted on the sonogram, in 8 of the 11 patients. Following these results, all patients had a repeated PCXR and only 6 of the 11 patients had a negative result for the second time with a suspicious LUS. However, the patients were treated and isolated as positive COVID-19 cases. 56
COVID-19 Performance of a Portable Pocket-Sized Ultrasound System
In comparison to a traditional ultrasound equipment system, portable pocket-sized ultrasound systems are considered inexpensive, flexible, and easy to handle. Therefore, a study was conducted to evaluate the feasibility of using it for COVID-19 diagnosis. There were no significant differences in the scores obtained on a high-end ultrasound equipment system compared to a portable ultrasound unit. The average scores obtained from the 2 equipment systems were normally distributed. There was a good correlation between the 2 equipment systems, regarding the measured parameters. 57
X-Ray Equipment System and Detecting COVID-19
When a patient arrives with an acute respiratory disease, at the emergency department (ED), a chest radiograph is usually the first examination ordered. 58 As a result, the ACR suggested placing portable X-ray equipment systems in the ED to assess lung changes and avoid moving suspected COVID-19 patients. PCXR can be regarded as a first-line diagnostic imaging tool for the assessment of lung abnormalities in symptomatic patients. 37
Chest Radiographic Appearance of COVID-19
COVID-19 patients were found to have lung consolidation and ground glass opacities on their CXRs.9,36,59–62 In addition, abnormalities on CXRs were observed in 62% of the COVID-19 patients demonstrating the above-mentioned SARS-CoV-2 imaging features, as well as 1% had a pneumothorax. Furthermore, CXRs revealed single, multiple, and interstitial infiltrates (48%, 52%, and 7% respectively). 59 Additionally, a study was conducted on 44 COVID-19 pediatric patients and of those, 38 patients who had peribronchial cuffing, as well as 28 had involvement of the peripheral space, 22 had GGOs, and 18.2% had lung consolidation. 60 Another study found nodules and reticular–nodular opacities in a CXR of 234 patients. 36 See Figures 8 and 9, which demonstrated radiographic features of COVID-19.
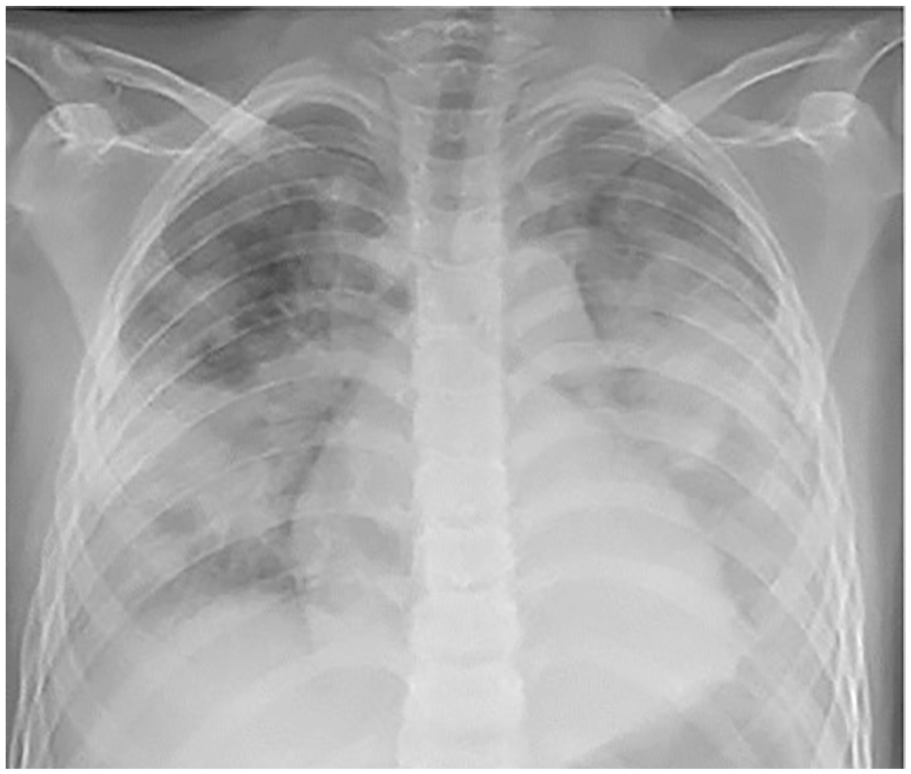
A chest radiograph of a 10- year-old boy. The image shows diffuse bilateral coalescent consolidation. 60
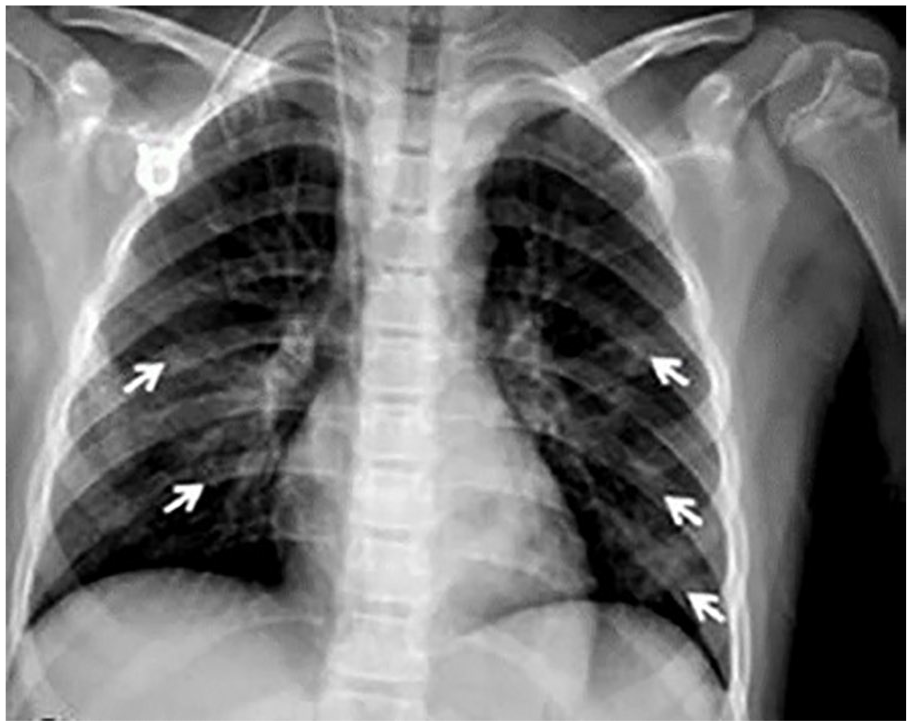
A chest radiograph a 10-year-old girl. The image shows patchy bilateral ground glass opacities (GGO) (white arrows). 60
Diagnostic Accuracy of a Chest Radiograph
It has been reported that patients who were presented for a CXR at the early onset of COVID-19, had a higher likelihood of having a normal or near-normal CXR. However, when the CXR was performed 6 days after the onset of the symptoms, it had significant diagnostic accuracy. 58 As a result, initial CXR can be a helpful tool in triaging suspected COVID-19 patients and those who may have poor outcome. 63 Furthermore, a CXR’s sensitivity was reported as 68.1% with variability ranging from 69% to 90% 36 and also between 25% ando 69%. 60
Additionally, to help radiologists in diagnosing patients and to avoid discrepancies, a CXR scoring system was established, for COVID-19 patients with pneumonia. The results revealed that the radiologists had a high level of agreement in the radiographic scoring. 64 However, for a pediatric CXR, a study indicated that there is no need for the radiographic diagnosis of COVID-19 and should only be performed for symptomatic patients, to evaluate the airway condition. 65
MRI and COVID-19
According to the literature, MRI is rarely used to diagnose COVID-19, and only few articles have discussed its role in this pandemic. 65 The reported image findings of COVID-19 in MRI included GGO, GGO with consolidation, air bronchogram, and pseudo cavity.11,66 Both previous studies recommended MRI as a potential alternative tool for chest CT, in detecting COVID-19, due to similar diagnostic imaging findings (See Figure 10).
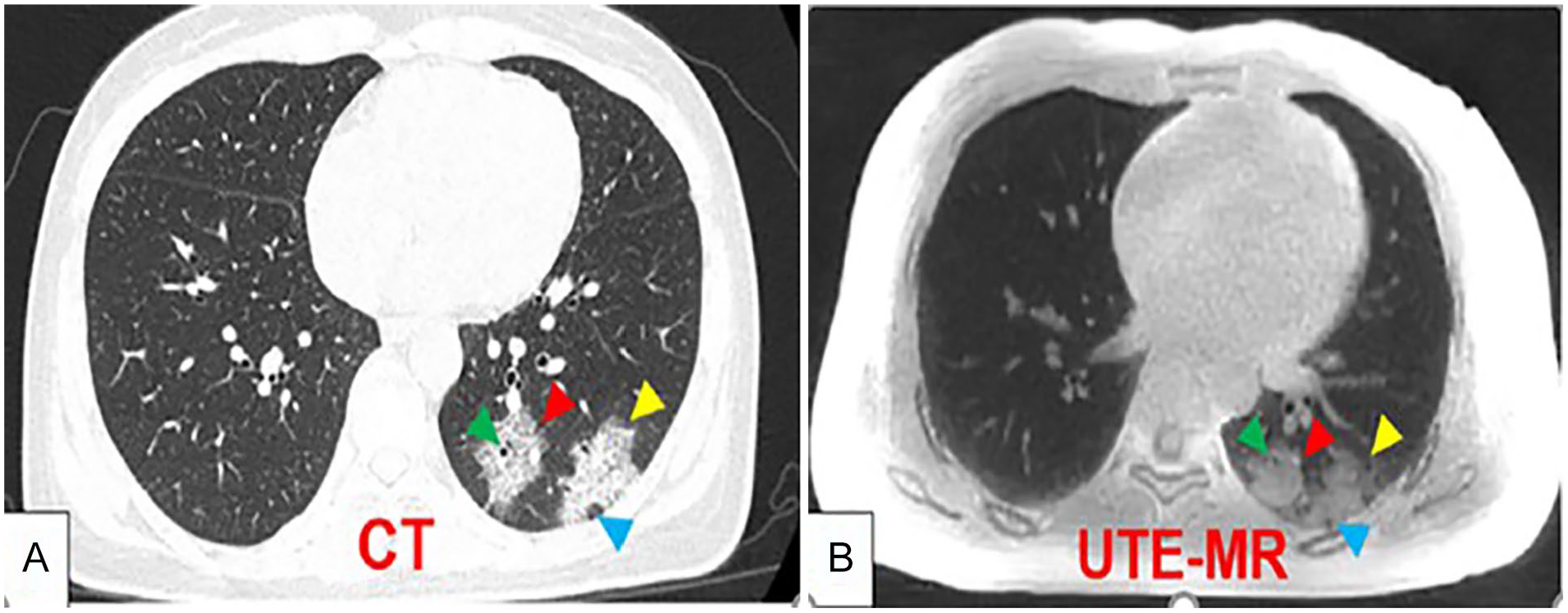
Image A is an axial chest CT and Image B is a Ultrashort echo time-Magnetic resonance imaging (UTE-MRI) axial chest image. Both images are for a 33-year-old COVID-19 patient. The red arrow shows a pure consolidation, the yellow arrow points on GGO with consolidation, green arrow shows an air bronchogram, and lastly the blue arrow points on a pseudo-cavity. 11 CT, computed tomogram; GGO, Ground-glass opacities.
Challenges Within the Radiology Department During the COVID-19 Outbreak
Several encountered challenges in the radiology department were reported. There are multiple factors have influenced the difficulty of developing a team-based schedule and implementing the work plan, including the ratio of the available staff to the number of cases presented to the department. The staff number was reduced due to positive or contact COVID-19 cases among the staff and school closure which has forced some staff to stay at home with their children. Additionally, the staff’s concern about personal protective equipment (PPE) effectiveness during the imaging of the infected patients was another challenge. 67
Furthermore, although LUS is one of the imaging modalities used to scan positive COVID-19 patients, the sonographers faced a unique challenge as their work requires a close contact for an extended period leading to an increased risk of infection. As a result, the LUS scan protocol was adjusted to include shorter examination time. In addition, due to the increased infection risk for sonographers, a LUS was suggested as the last option for COVID-19 patients. 67
Furthermore, at the peak of the pandemic, a shortage of PPE posed a significant challenge to imaging departments.67,68 The PPE distribution process was determined based on the risk within that specific work area. Besides, the highest level of allowed PPE was only allotted to radiographers, who had frequent patient contact with those exhibiting fever. 68 The other highlighted challenge is the infection control procedures. During the early stages of the epidemic, an infection control unit was established to ensure that the radiology department could function normally and effectively. The infection control team typically involved the head of the imaging department, the radiographer-in-charge, the nurse-in-charge, and the chief resident. 68
Therefore, to reduce the risk of cross-contamination, in the non-portable modalities such as CT and MRI, the non-urgent imaging requests were delayed until a COVID-19 diagnosis was confirmed. However, If the examination was considered urgent, dedicated imaging equipment was reserved for the last case of the morning or the afternoon shift. 69 Conversely, due to a potential staff shortage, during the pandemic, some scheduled appointments and non- essential services had to be canceled. Accordingly, the referring physician and the radiologist had to decide the priority of each examination. This procedure offered the medical imaging staff enough time to implement infection control measures while also reducing the workload. 69 The last reported challenge concerned radiology was the training for students in the radiology department and the possibility COVID-19 infection. 67
Discussion
This review investigated the role of different imaging modalities during the COVID-19 pandemic and the challenges it posed for the radiology department. CT was the most significant modality in detecting and diagnosing SARS-CoV-2. The majority of the reviewed articles underscored that CT had a higher sensitivity than a rRT-PCR test.18–22,25,30,70,71 Even though a rRT-PCR test was routine for diagnosing COVID-19, published studies reported many false-negative cases while the chest CT revealed a positive diagnosis. This could be due to various rRT-PCR technique limitations, such as incorrect swabbing, extraction, and PCR transport media. 8
Moreover, a chest CT demonstrates the lower respiratory tract, while rRT-PCR test was limited to the upper respiratory tract. 28 In addition, CT results can be obtained and reviewed immediately after the examination compared to rRT-PCR test results, which may take 24 hours or more. 21 To improve CT detection of COVID-19, the recognition of subtle imaging changes should be improved. This is important such that it would help physicians in diagnosing the disease accurately and quickly, especially in the early stages when the rRT-PCR test was negative. 9
Additionally, CT findings in COVID-19 patients can help to predict the course of the disease and the length of the hospital stay, ICU admission rate, and the disease outcome. Hence, this can help to manage the patients, and plan the resources more effectively, especially for the use of ICU beds. 16
To decide which imaging modality of choice to be used effectively for COVID-19 imaging diagnosis, many factors should be considered such as mobility of patient, availability, and ease of deep cleaning. 72 A CXR is a critical tool for diagnosing and detecting a COVID-19 pneumonia. 73 In contrast, chest CT was debated as the most accurate and sensitive in detecting COVID-19, at an early stage.55,74 Therefore, chest CT has a significant advantage over a CXR regarding the initial stage of COVID-19, as peripheral regions of GGOs are the diagnostic hallmark of early SARS-CoV-2, which is easily missed on a CXR. 21 Although the CXR findings for COVID-19 are not specific, any positive diagnostic indication can be used to justify a hospitalization or repeat the rRT-PCR test, if the first test was negative. 60 However, the role of performing a CXR to monitor the patients clinically is controversial. It is not recommended by the Fleischner Society to perform a daily CXR on intubated stable patients, but it is recommended to correlate the imaging findings to laboratory and clinical parameters. 36
In comparison, LUS can be a useful imaging tool for detecting and monitoring COVID-19 pneumonia lung lesions. In addition to LUS being an affordable, flexible and radiation free imaging modality, it also provides supplementary imaging information. 47 Compared to CXR, lung point of care ultrasound (LPOCUS), in children, has shown an excellent sensitivity and specificity. Taking these benefits into consideration, the use of LPOCUS may reduce the need for CXRs in COVID-19 patients. Additionally, LUS can be used for pregnant patients enabling safe and multiple serial imaging, without exposing the patient and fetus to radiation. 10 As a result, this would reduce the overall number of times that the radiographers get exposed to SARS-CoV-2, 40 reduce in-hospital transfer, and the contamination risk of medical equipment.47,75 Moreover, LUS was identified to replace chest radiography and CT in detecting pathology related to lung pleura and parenchyma. Similarly, LUS can help to identify and monitor infection in COVID-19 patients even before the onset of disease progression. 47 Moreover, a study suggests that for the initial assessment of lung involvement, in COVID-19 patients, a chest CT can be replaced by LUS. This was due to the disease severity observed by LUS had a high correlation with the severity assessed on CT. 75 Furthermore, it was reported that detection of B lines on LUS is more frequently associated with COVID-19 than the abnormal CXR. 51
Regarding MRI, only few studies have clearly explained the role of MRI in COVID-19 pandemic.11,66 It has been demonstrated that MRI and CT can detect COVID-19 infection in the same way. Indeed, using a unique technique like such as UTE-MRI has shown that image quality is equivalent to a low dose CT image, with the same imaging features. Furthermore, depending on those findings, UTE-MRI can substitute CT to reduce the patient’s radiation dose as the patient may require multiple CT scans during the illness. 11 Also, the other study did not recommend using MRI as a first choice to evaluate the pulmonary opacities even though it has the same capability of CT. This can be related to some MRI limitations such as loss of signal due to physiological respiration and heart movement conditions. 66
The reported challenges that the radiology department faced were mainly related to health infection control, staff workload, and the radiology training of students. Therefore, strict policies and procedures must be followed and implemented to control the virus spread. Precautionary measures, such as the use of portable X-ray equipment systems to limit the transport of infected patients to radiology departments, the use of PPE and disposable gowns, and the disinfection of CT, MRI gantry, and ultrasound transducers, should be strictly enforced by radiology department personnel. 76 Due to close contact with the patient and extended examination time, the sonographer or sonologist may be at risk of infection during sonography, particularly with point-of-care and portable sonograms. 77 In terms of radiology staff, temporal and physical team segregation can effectively manage the radiology department workload. 69 As a result, maintaining staff mental and physical health is critical in providing proper healthcare to COVID-19 patients. 78 The studies were further summarized in A and B appendices, accessible in the online supplemental material.
Limitations
This review has several limitations in terms of searching criteria and types of the included studies. First, only 3 databases were used to identify the relevant articles. If more databases could have been included, it would have increased the number of the reviewed articles as well as strengthen the outcomes. However, various articles from different countries discussing different imaging modalities were identified and reviewed. This was intentional done to discuss and provide an overview of the role of imaging department, in the current pandemic. Second, only a few MRI related articles were identified, therefore making it difficult to provide sufficient evidence compared to other imaging modalities. Therefore, future imaging reviews should emphasize the role of MRI during COVID-19. The implications of this review include updating the clinical community about the diagnostic role of different imaging modalities, comparing imaging techniques in terms of detection accuracy and safety, reviewing the imaging findings of COVID-19 features and imaging department obstacles during the pandemic. This review can provide an additional educational resource on COVID-19 imaging as well as support future radiology research initiatives.
Conclusion
Although the rRT-PCR test is considered the initial step for diagnosing COVID-19, published studies reported many false negative cases, due to technique related limitation factors. Furthermore, shortage of these test kits in some countries has prompted researchers to look into alternative diagnostic methods, such as clinical imaging. A chest CT can image the lower respiratory tract whereas the rRT-PCR test is limited to the upper respiratory tract. It is also considered the most accurate and sensitive technique for detecting COVID-19, in its early stages. Conversely, LUS can also be used for pregnant patients, enabling safe and multiple serial imaging, without the risk of radiation to patient and fetus. Moreover, UTE-MRI can be used in place of CT to reduce the patient’s radiation dose, if serial CTs are required. Precautionary measures included the use of portable X-ray equipment and utilization of PPE, so as to control the spread of all infections.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793211056903 – Supplemental material for The Role and Challenges of Clinical Imaging During COVID-19 Outbreak
Supplemental material, sj-docx-1-jdm-10.1177_87564793211056903 for The Role and Challenges of Clinical Imaging During COVID-19 Outbreak by Mustafa Alhasan and Mohamed Hasaneen in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-2-jdm-10.1177_87564793211056903 – Supplemental material for The Role and Challenges of Clinical Imaging During COVID-19 Outbreak
Supplemental material, sj-docx-2-jdm-10.1177_87564793211056903 for The Role and Challenges of Clinical Imaging During COVID-19 Outbreak by Mustafa Alhasan and Mohamed Hasaneen in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The authors would like to thank the Radiography and Medical Imaging senior students and staff (Malak Al Hariri, Sara Awwad, Noura Attieh, Leyan Hussein, Yasmin Aktar, Lubna Jasim, Sahana Kotian, Jerald Paul) for providing help during the research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.