
Abstract
Objective:
The purpose of this study was to look for the earliest, cost -effective method that can be added to the routine antenatal screening for identifying patients who might develop gestational diabetes mellitus (GDM) in a proactive manner, as opposed to the current reactive approach of screening and treating GDM, during the second trimester of pregnancy.
Materials and Methods:
190 singleton pregnant women in the age group 18-35 years were selected for the study. On these women two step assessment was done. The current project was carried out to utilize sonography as an early, cost-effective method which could be added to routine antenatal screening for identifying patients, at risk for developing GDM.
Results:
Body mass index was found to have a significant association in those patients with GDM with a P < .001. There was a significant association between subcutaneous adipose tissue (SAT) depth and occurrence of GDM, with a P-value of <.001. Also, in the present study, the occurrence of GDM significantly increased with a rise in visceral adipose tissue (VAT), and there was a significant association between the two, with P < .001. It was noted that there were greater incidences of GDM as VAT depth increased. The existence of GDM greatly increased with a rise in total abdominal tissue (TAT), and there was a significant association between the two, with P < .001
Conclusion:
The sonographic measurement of SAT, VAT, and TAT, could be potential marker to identify probable events for the development of GDM, among Asian Indian women who tend to have T2DM, due to differential distribution of fat.
Gestational diabetes mellitus (GDM) is a prevalent women’s health concern in India and nationally they possess the maximum number of diabetic patients, only second to China. Indian women are estimated to present with approximately 3.8% to 17.9% pregnancies, affected by GDM.1-3 The term, GDM, is defined as any degree of glucose intolerance with the onset or first recognition during pregnancy, whether or not insulin is used for treatment.4-6 GDM has been associated with a variety of adverse maternal and perinatal outcomes. 7 Several risk factors are associated with GDM, including advanced age, ethnicity, increased body mass index (BMI), previous history of GDM, a family history of diabetes mellitus (DM), smoking, and a history of pregnancy disorders (such as miscarriage, stillbirth, macrosomia, preterm delivery, eclampsia, preeclampsia, etc.). Early treatment of women, diagnosed with GDM, can help in reducing GDM induced complications to the mothers and fetus such as polyhydramnios, congenital malformations, infections, and hypertensive disorders of pregnancy. Other related birth difficulties such as macrosomia, shoulder dystocia, birth injuries, as well as neonatal hypoglycemia and hyperbilirubinemia may also be diminished. 8
With a sedentary lifestyle, along with unhealthy food habits, both type-2 diabetes mellitus (T2DM) and obesity are increasing globally. Obesity itself leads to several metabolic disorders and cardiovascular diseases (CVDs). The severity of these diseases is directly linked to the distribution of body fat rather than its accumulation. 9 Research conducted by Cnattingius et al, noted that females who experienced considerable weight gain, had increased complications during their pregnancy. 10 Maternal obesity is found to be directly linked to having a higher risk of GDM. 11 Enhanced deposition of fat around intra-abdominal area is found to be correlated with increased insulin resistance, glucose intolerance, and development of T2DM.12,13
Often, many women with GDM, eventually convert to overt diabetes and approximately 10% GDM patients developed T2DM postpartum, as well as 40% of patients, a decade after delivery.14,15 Several guidelines have been posed to identify patients at risk for GDM; however, some factors were derived from studies involving non-pregnant females and this restricts the criteria to identifying pregnant women with an increased risk for adverse perinatal outcome. 16 In the last decade, a study on hyperglycemia and adverse pregnancy outcomes (HAPO) was conducted to possibly correlate and identify those patients at risk with pregnancy glucose intolerance and the development of overt diabetes. These patient’s primary risks included higher infant birth weight, primary cesarean section delivery, and neonatal hypoglycemia. Secondary outcomes were preclampsia, preterm delivery, shoulder dystocia/birth injury, and hyperbilirubinemia. The study concluded that there was a significant correlation between higher levels of maternal glucose with an increased frequency of negative primary and secondary postpartum outcomes. 17 Additionally, there was an increased risk of fetal congenital anomalies as well as maternal nephropathy and retinopathy complications, due to diabetes, which required treatment during pregnancy.
Indian women registered the highest incidences of GDM, compared to their Caucasian and South Asian women counterparts. 18 Therefore, the diabetes in pregnancy study group India (DIPSI) formulated a single step, cost-effective, simple screening test which requires that 75 g of glucose be administered orally to patients during the 26 to 28 week of pregnancy and blood glucose levels are recorded 2 hours, postadministration. If the blood glucose concentration is found to be ≥140 mg/dL, those patients were identified as suffering from GDM. The logic behind performing the test was that a normal female would maintain euglycemia after 2 hours, but patients at risk of GDM would be dysglycemic, due to impaired secretion of insulin. Unfortunately, the test has a low diagnostic sensitivity, and this was a serious limitation. In short, this limitation makes this diagnostic approach ineffective for screening patients at risk for GDM. Moreover, there are multiple proposed recommendations worldwide. 19
Visceral adipose tissue (VAT) plays an important role in a number of metabolic or associated diseases such as dyslipidemia, hypertension, and impaired fibrinolysis as well as increases the risk of CVDs.18,19 VAT produces fewer adipokines and more tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), and insulin resistance is induced by an interplay of these cytokines. 20
Visceral fat can be monitored by computed tomography (CT) which is not feasible in pregnancy due to the adverse effects of radiation exposure to the fetus in utero. Therefore, sonography should be considered an alternative diagnostic screening technique. 21 The lack of uniformity in guidelines leads to difficulties in establishing the diagnosis of GDM. Thus, it is essential to look for easy and early screening strategies to identify women, at risk for developing GDM. The purpose of this study was to look for the earliest, cost-effective method that can be added to the routine antenatal screening for identifying patients who might develop GDM in a proactive manner, as opposed to the current reactive approach of screening and treating GDM, during the second trimester of pregnancy. In other words, ideally it is advantageous to identify the problem before the development of its sequalae and the potential impact on the pregnancy outcome.
Materials and Methods
For this study, a group of women, age 18 to 35 years old, with singleton pregnancies were recruited. Each individual in the potential patient population completed a questionnaire which included their age, socio-economic status, education, history of polycystic ovaries syndrome (PCOS), or GDM in previous pregnancies and family history of DM. Patients with multiple pregnancies and/or suffering from prepregnancy DM, prior pregnancy affected by GDM, prior history of polycystic ovarian syndrome, and already on medication of metformin/corticosteroid were excluded. The selected women participated in step 2 of the assessment. The objective of the study and questionnaire were duly approved by Ethics Committee, SMS Medical College, Jaipur, India (14/MC/EC/2018).
The consented females were evaluated using a 2-step process. The first step of the study occurred during the 11 to 14 weeks of gestation; the abdominal adipose tissue depth was measured utilizing sonography. 22 Subcutaneous adipose tissue (SAT) depth was measured from the outer border of the rectus abdominus muscle to the skin surface, at the intersection of the linea alba and the umbilicus. Visceral abdominal tissue depth was measured from the inner border of the rectus abdominus muscle to the anterior wall of the abdominal aorta. Total abdominal tissue (TAT) depth was measured from the SAT layer surface to the anterior wall of the abdominal aorta, as shown in Figure 1.
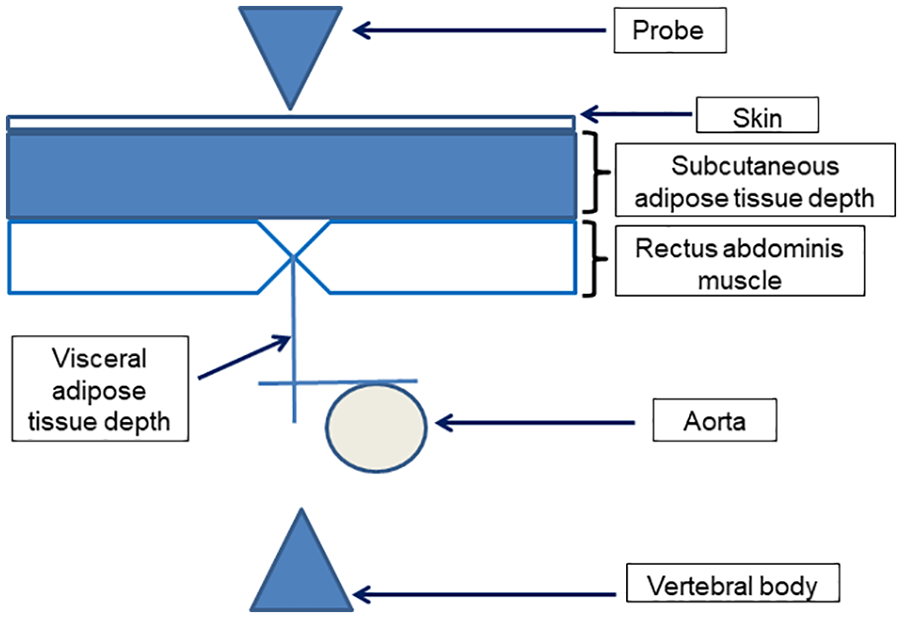
This is a schematic representation of adipose tissue depth measurements, in a pregnant woman.
The sonographic image depth and zoom settings were standardized, such that the aorta was at the bottom of the screen and the vertebral bodies were just visible. This technique had inter-observer reliability of 0.79 (95% confidence interval [CI]: 0.69-0.88) for SAT and 0.87 (95% CI: 0.82-0.93) for VAT. Measurements were taken using a HITACHI Aloka Pro Sound ultrasound machine with a 3- to 5-MHz transducer. An actual image of sonograph depicting the method of measuring adipose tissue depth has been shown as Figure 2.
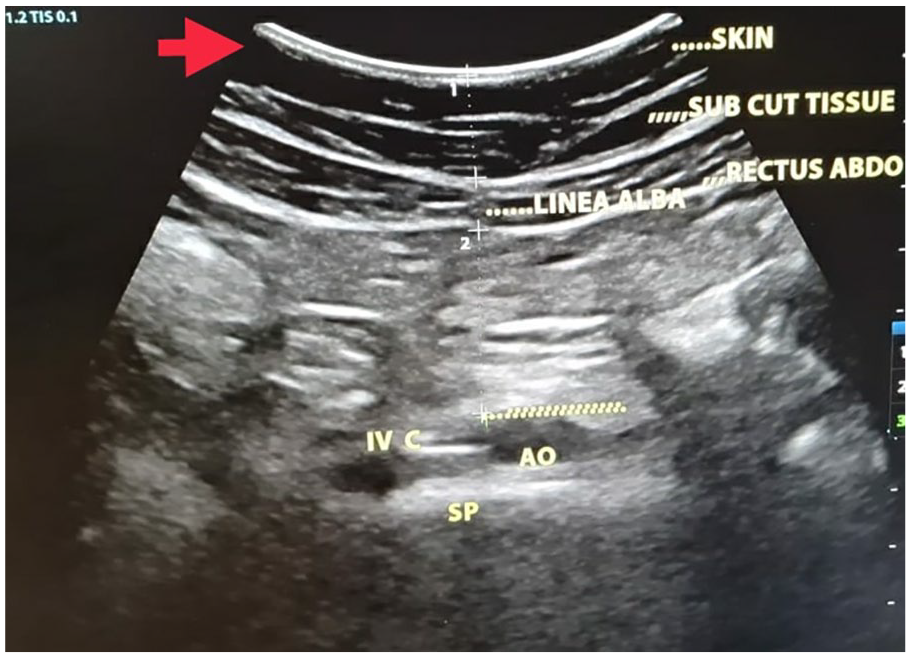
The sonogram demonstrates the procedure for measuring the adipose tissue depth in a pregnant patient (ie. IVC-Inferior Vena Cava, AO-Aorta, SP- Spine).
For the second step, participants completed an oral glucose tolerance test (OGTT) following the guidelines of IADPSG. The women were studied during the gestational period of 24 to -28 weeks. Following the procedure, they underwent a fasting blood sugar level test. The OGTT was performed at a specified location, where they were asked to consume 75 g of glucose. The results were evaluated using IADPSG criteria 1 and 2 hours after consumption. If any of the plasma glucose levels were found to be equal or more than 92 mg/dL for fasting; 180 mg/dL for 1 hour postconsumption of glucose or 153 mg/dL for 2 hours, then the woman was considered a GDM patient.
Results
The study on GDM in this cohort of pregnant women was conducted in a local university’s department of Obstetrics and Gynecology. The study results were based on 190 women attending antenatal care in the hospital’s out-patient department and met the inclusion criteria of being 18 to 35 years old with a singleton pregnancy, at 11 to 14 weeks gestational age. Excluded from the study were women with known prepregnancy DM, prior pregnancy affected by GDM, prior history of polycystic ovarian syndrome, already on medication for metformin/corticosteroid.
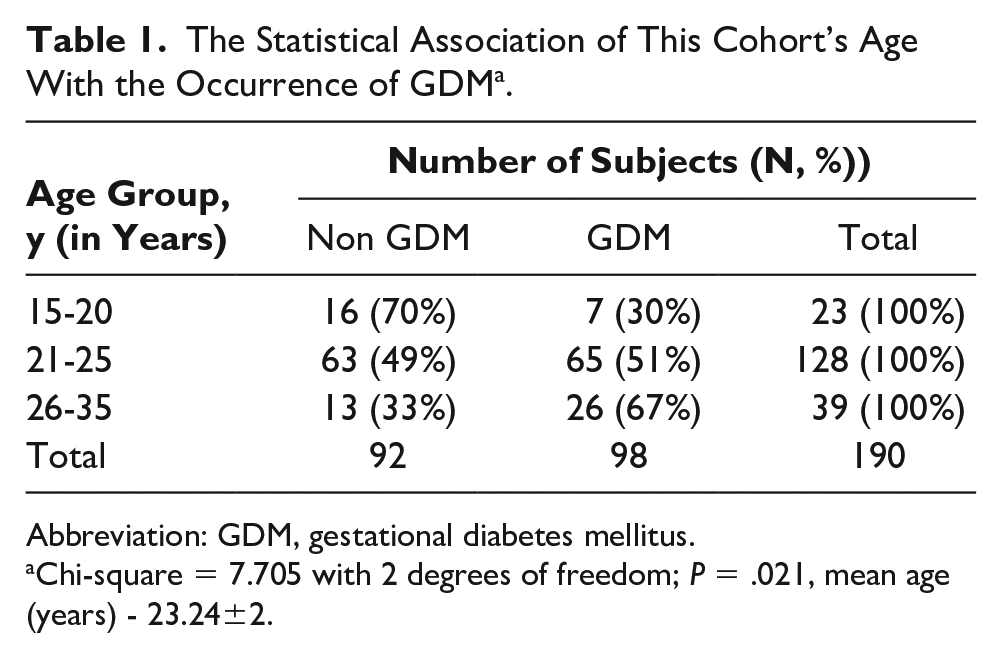
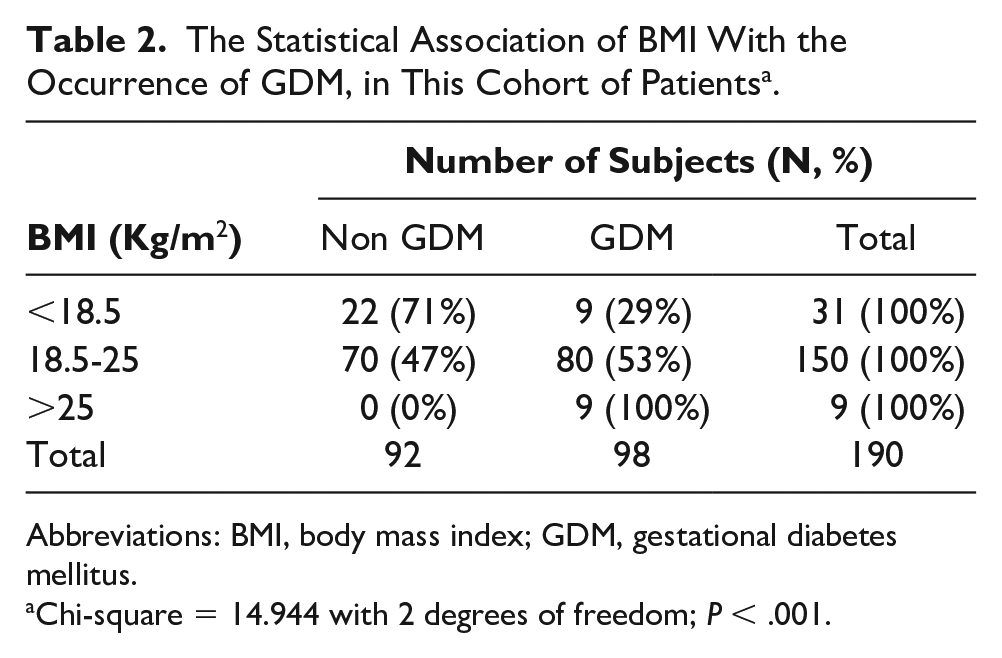
The women who were selected underwent sonographic imaging at 11 to 14 weeks of gestation to determine their abdominal adiposity. At 24 to 28 weeks of gestation, their fasting blood glucose values were taken, and if it was found to be less than 92 mg/dL, a 75 g OGTT was done. The subjects were divided into 2 groups-non-GDM and GDM. Patients who had one or more abnormal value of either the fasting blood sugar level (>92 mg/dL) or 1-hour level (>180 mg/dL) or 2 hours level (>153 mg/dL) were considered to have GDM. This resulted in 98 subjects in the GDM group and 92 in the non-GDM group. The maximum number of females studied was in the age group of 21 to 25 years, out of which 49% had GDM (See Table 1). From the preliminary investigation based on plasma glucose concentrations, it was observed that there was an increase in the incidences of GDM with an increase in age of the pregnant female. Body mass index for the subjects were measured at 11 to 14 weeks of gestation. The range was 18 to 28 (kg/m2) with a mean value of 20.67 (kg/m2). In the present study, BMI was found to have a significant association with GDM with a P < .001 (See Table 2). From this observation, it was deduced that there was a significant correlation of an increase in the incidences of GDM with an increase in BMI.
The Statistical Association of This Cohort’s Age With the Occurrence of GDM a .
Abbreviation: GDM, gestational diabetes mellitus.
Chi-square = 7.705 with 2 degrees of freedom; P = .021, mean age (years) - 23.24±2.
The Statistical Association of BMI With the Occurrence of GDM, in This Cohort of Patients a .
Abbreviations: BMI, body mass index; GDM, gestational diabetes mellitus.
Chi-square = 14.944 with 2 degrees of freedom; P < .001.
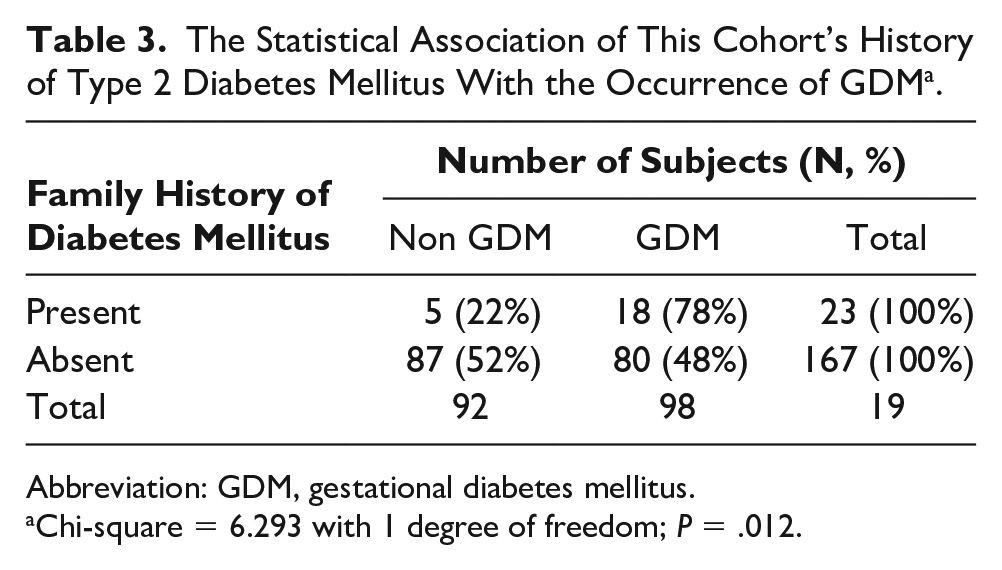
In the present study, there was a significant association between the occurrence of GDM and family history of Type 2 DM in the subjects, with the P = .012 (see Table 3). It was observed that there was an increase in the occurrence of GDM when seen in terms of positive family history. However, considering the significance with no family history of diabetes, there was not much difference between the groups.
The Statistical Association of This Cohort’s History of Type 2 Diabetes Mellitus With the Occurrence of GDM a .
Abbreviation: GDM, gestational diabetes mellitus.
Chi-square = 6.293 with 1 degree of freedom; P = .012.
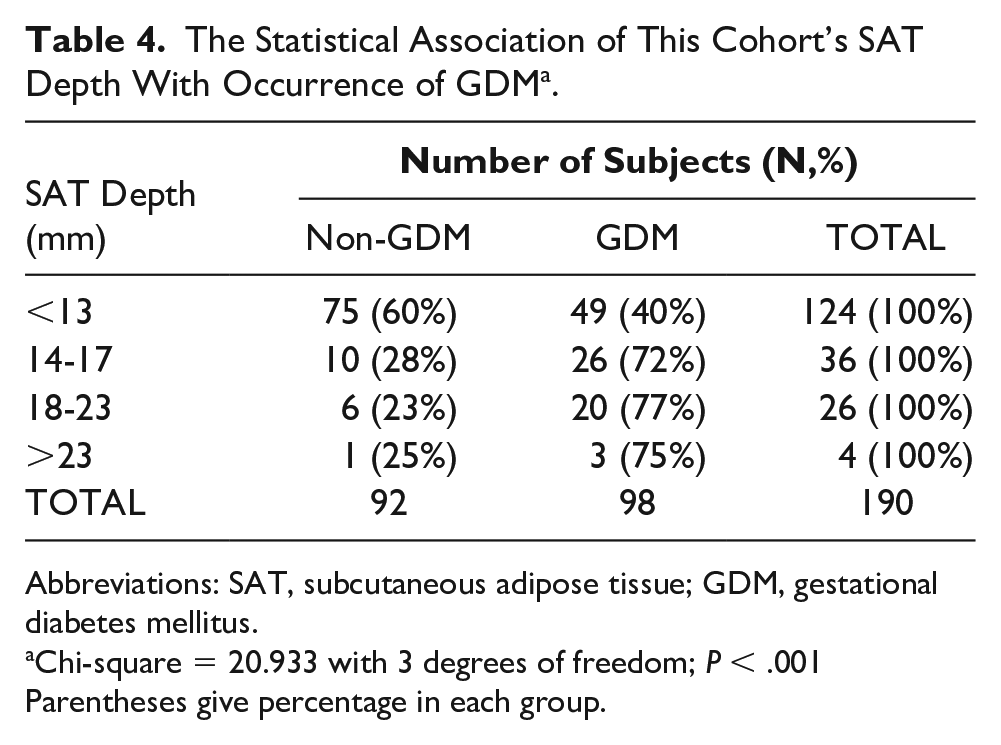
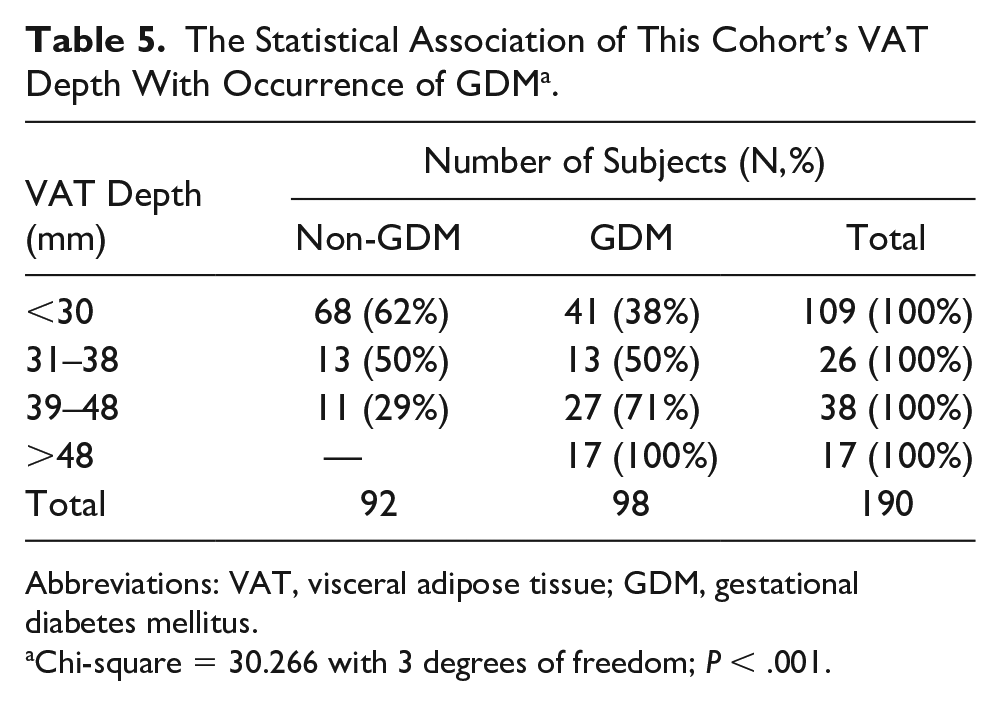
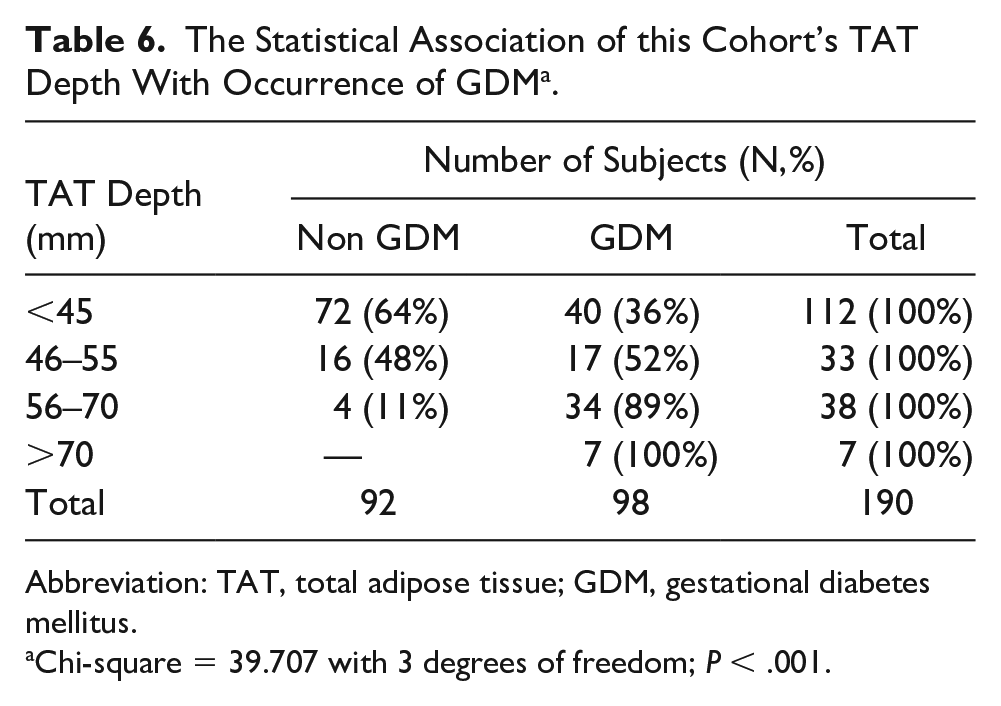
Presence of GDM significantly rose from 39 to 72% once SAT depth increased from <13 mm to >14 mm or more as shown in Table 4. There was a significant association between SAT depth and occurrence of GDM, with a P-value of <.001. Also, in the present study, the occurrence of GDM significantly increased with a rise in VAT, and there was a significant association between the two, with P < .001 (Table 5). It was noted that there were greater incidences of GDM as VAT depth increased. The existence of GDM greatly increased with a rise in TAT, and there was a significant association between the two, with P<.001 (See Table 6). Figure 3 graphically represents the distribution of the TAT depth in non-GDM and GDM category using percentage in each group.
The Statistical Association of This Cohort’s SAT Depth With Occurrence of GDM a .
Abbreviations: SAT, subcutaneous adipose tissue; GDM, gestational diabetes mellitus.
Chi-square = 20.933 with 3 degrees of freedom; P < .001 Parentheses give percentage in each group.
The Statistical Association of This Cohort’s VAT Depth With Occurrence of GDM a .
Abbreviations: VAT, visceral adipose tissue; GDM, gestational diabetes mellitus.
Chi-square = 30.266 with 3 degrees of freedom; P < .001.
The Statistical Association of this Cohort’s TAT Depth With Occurrence of GDM a .
Abbreviation: TAT, total adipose tissue; GDM, gestational diabetes mellitus.
Chi-square = 39.707 with 3 degrees of freedom; P < .001.
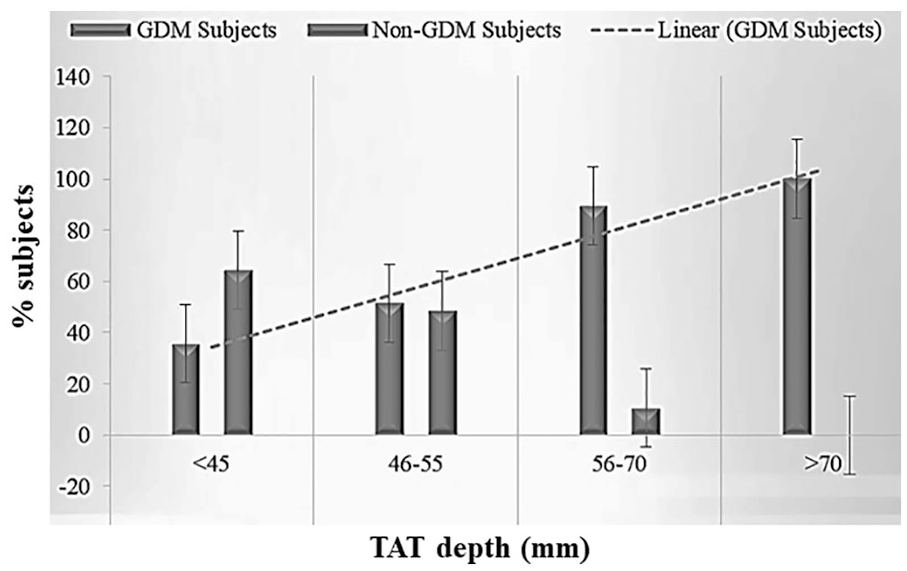
The statistical association of total adipose tissue (TAT) depth with occurrence of GDM, in this cohort of patients. GDM, gestational diabetes mellitus.
Logistic Regression for Prediction of GDM
A logistic regression analysis was conducted to predict GDM in the 190 pregnant participants which utilized age, gestational age, thyroid stimulating hormone (TSH), subcutaneous adiposity, visceral adiposity, and total adiposity, as predictors. A test of the full model was statistically significant, indicating that the predictors reliably distinguish between positive and negative outcomes of gestational diabetes (chi square = 56.311, df = 8, P = .000) (See Table 7). The prediction success overall was 69.5%, based on 66.3% positive outcomes and 72.8% negative outcomes.
The Full Statistical Model Test for Prediction, Based on the Variable Measurements Collected From This Cohort of Patients a .
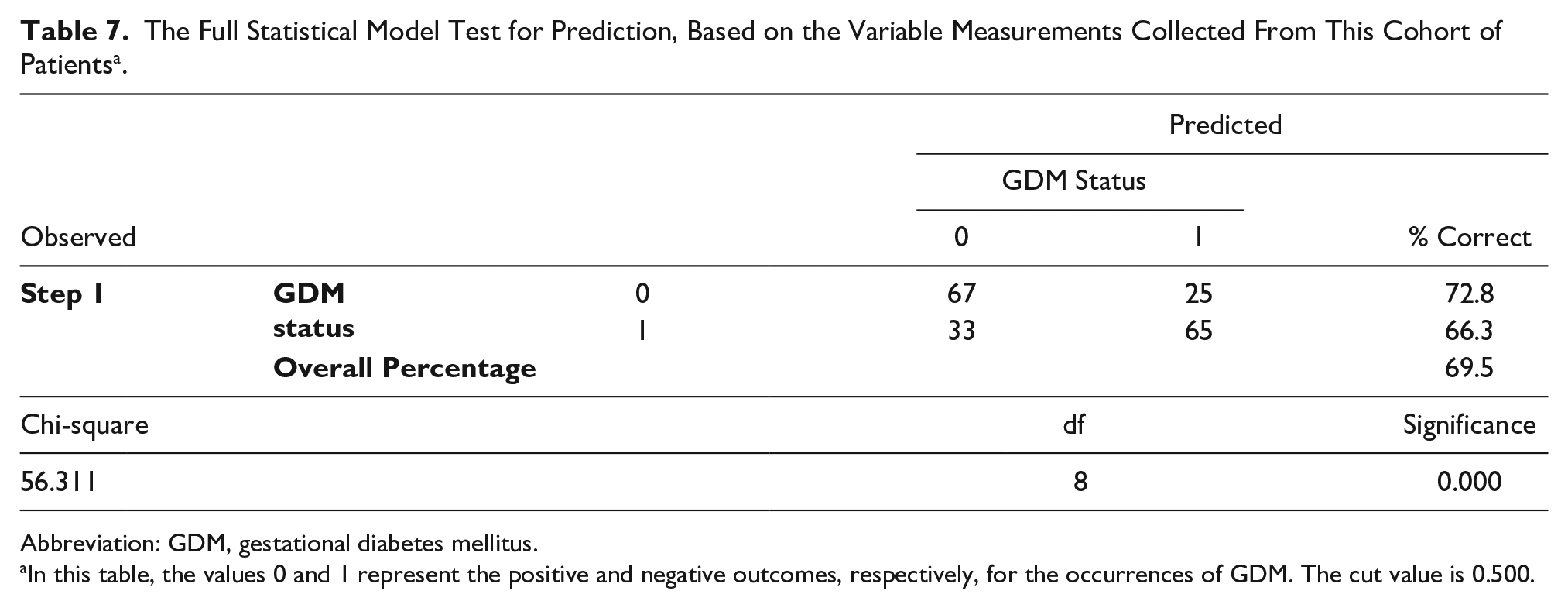
Abbreviation: GDM, gestational diabetes mellitus.
In this table, the values 0 and 1 represent the positive and negative outcomes, respectively, for the occurrences of GDM. The cut value is 0.500.
Discussion
A random selection of subjects visiting the outpatient ward showed that nearly 50% of the subjects had GDM with the greatest number of subjects in non-GDM category overall. In the GDM groups, the most frequent occurrence was in the range of 21 to 25 years. The prevalence of GDM was seen to be increasing with age. A study conducted by Lao et al, also found that there was a significant difference and positive correlation in the prevalence of GDM with age. 23 Kuo et al, also found a strong association between maternal age and incidences of GDM. 24
In this study, most of the pregnant females had BMI between 18.5 and 25 kg/m2 and it was found that an increase in BMI led to a significant increase in the prevalence of GDM. The results of the present cohort are comparable to several research studies which were being conducted worldwide, including a study done by Kim et al, where they found an increased risk of GDM was associated with increasing BMI. 25 A significant association between the occurrence of GDM and the subjects, who had a family history of T2DM, was observed in the present cohort. This was similar to observations made by Moosazadeh et al, in a meta-analysis which revealed that having a family history of T2DM was a risk factor in developing GDM. 26
Obesity is one of the major risk factors for diabetes. Indeed, a recent meta-analysis of 32 studies concluded that BMI, waist circumference, and waist-to-hip ratio had similar associations with incident diabetes. Body surface measurements, such as waist circumference, do not distinguish between the various adipose tissue depots, which have differences in biologic function. Specifically, there can be sizable differences in the amounts of VAT and SAT between individuals with the same waist circumference. In this study, the presence of GDM significantly increased from 39% to 72%, with an increase in SAT depth, from < 13 mm to > 14 mm. De Souza et al, conducted a study in a Caucasian population where SAT was not deemed important in evaluation, based on the histology that is more heterogeneous. 27 In contrast, the present study indicated a strong association of SAT depth with incidences of GDM. Whereas, in another study done by Yang et al, in their Korean (Asian) population demonstrated a range of SAT depth which was 9 to 41 mm, with a mean of 19 ± 5 mm and had results similar to the present cohort. Yang et al, also observed a significant association existed between elevated SAT and development of GDM. 28
The disparity in the significance of SAT among various study populations could be explained by the fact that SAT is thicker in adult Asian Indians and South Asians, compared to their western counterparts.29,30 The presence of dysfunctional adipocytes in SAT of Asian Indians could be the culprit for being more susceptible to metabolic disorders. It has been further observed that SAT is the main depot of free fatty acids (FFA), which are eventually delivered to the liver, indicating that SAT may be the causal factor associated with hepatic insulin resistance in abdominal adiposity. 31 Since SAT is higher in Asian Indians, it might exert more metabolic effects and hence, have greater significance.
Subjects with an increased VAT depth also had an increased incidence of GDM. Maximum number of GDM patients had VAT depth less than 31 mm. This was corroborated by De Souza et al, while evaluating the role of first-trimester maternal abdominal adiposity in the prediction of dysglycemia and GDM, found that the VAT depth had a range from 1.1 to 11.4 cm, with a mean of 4.1 cm. They demonstrated that VAT is a pathogenic marker of dysglycemia. 32
Epidemiological studies have shown the consequence of excess fat that leads to adverse outcomes is primarily due to the location of the fat. Centrally located visceral fat appears more pathogenic than subcutaneous fat. 33 In this study, the range of TAT depth was from 9 mm to 89 mm, with a mean of 42.9 mm. TAT depth had a statistically significant association with the blood sugar levels and presence of GDM. In the study by Souza et al, it was observed in their subjects, the range of TAT was 20 mm to 142 mm, with a mean of 59 mm. In another study done by the same group, the role of hepatic fat and abdominal adiposity in early pregnancy was evaluated together to predict impaired glucose homeostasis in mid-pregnancy. The results concluded that first trimester TAT and VAT depth along with maternal hepatic fat, helped in predicting the onset of GDM, independent of maternal age, ethnicity, family history of type 2 DM, or maternal BMI. 34
Limitations
This was a cohort study and participants were a convenient sample therefore the results are specific to them and not generalizable. The study design would be classified as preexperimental and has the inherent threats to internal and external validity.
Conclusion
In this cohort study, 190 pregnant females, with a singleton pregnancy at 11 to 14 weeks, were studied to determine the factors responsible for the development of GDM. It can be concluded, based on the multivariate analysis with logistic regression, that none of the study variables factors were significant predictors for GDM. However, the sonographic measurement of SAT, VAT, and TAT had the potential to identify the development of GDM. This has clinical significance based on the fact that Asian Indian women have a higher tendency to have T2DM, due to differential distribution of fat.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.