
Abstract
Objective
The rs10229583 polymorphism near paired box gene 4 (PAX4) is associated with insulin resistance and type 2 diabetes. Mutations in the PAX4 gene may be associated with impaired differentiation/development of pancreatic islet beta cells during fetal development and, consequently, a compromised insulin response to high blood glucose. To ascertain whether this polymorphism plays a role in gestational diabetes mellitus (GDM), we investigated the genotypic and allele frequency differences between GDM and normal pregnancies.
Methods
A total of 310 GDM and 440 normal pregnancies were evaluated. Allele and genotype frequencies of rs10229583 were determined for all participants with Sanger sequencing and SNaPshot. Association of the allele and genotypes of the single nucleotide polymorphism with the disease was analyzed using Pearson’s χ2 test and OR (odds ratio).
Results
The G allele was more frequent in patients with GDM compared with controls (OR = 1.47, 95% confidence interval (CI): 1.12–1.939). The GG genotype frequency of rs10229583 was significantly different between subjects with GDM and normal controls (OR = 1.411, 95% CI: 1.032–1.928). The OR of the GA + GG genotype was 3.182 (95% CI: 1.294–7.826) for patients with GDM compared with controls.
Conclusion
The present study suggests that rs10229583 is associated with GDM.
Introduction
Gestational diabetes mellitus (GDM) is defined as glucose intolerance first diagnosed during pregnancy and is associated with increased risk of preeclampsia, perinatal mortality of the fetus and type 2 diabetes (T2D) development. 1 During pregnancy, women experience increased peripheral insulin resistance, which is explained, in part, by increased production of estrogen, human placental lactogen and prolactin.2–4 To maintain glucose homeostasis, insulin secretion is increased. GDM occurs in cases where insulin secretion fails to compensate for insulin resistance. Women with a history of GDM are at a higher risk of developing T2D later in life. 5 GDM and T2D are multifactorial disorders with a common pathogenesis. The diseases share several features, including pancreatic beta-cell dysfunction, insulin resistance and association with similar risk factors. A variety of risk factors, including obesity, family history, lifestyle, ethnicity, genetics and physical inactivity, contribute to the development of both GDM and T2D. 6 Earlier studies strongly supported the possibility that GDM and T2D share the same genetic background. Over the past few decades, numerous studies have focused on the identification of accumulating genetic variants that are strongly associated with T2D. 7
The rs10229583 polymorphism is located downstream of the paired box gene 4 (PAX4) gene, which is located on chromosome 7q32 and belongs to a family of transcription factors. The gene plays an important role in the differentiation and development of pancreatic islet beta cells during fetal development.8,9 A number of investigations to date have identified rs10229583 near PAX4 as a locus for T2D. 10 However, little is known about its potential association with GDM. Based on these findings, we hypothesized that the rs10229583 single nucleotide polymorphism (SNP) is associated with predisposition to GDM. Therefore, PAX4 may be a novel target candidate gene for GDM therapy.
In the current study, we examined the genetic, clinical and biochemical differences between GDM and normal pregnancies according to the Strengthening the Reporting of Genetic Association Studies initiative. 11 We aimed to clarify the relationship between rs10229583 and GDM as well as its association with clinical and biochemical parameters. Our results may provide better insights into the mechanisms underlying PAX4 gene variations in the development of GDM.
Materials and methods
Subjects
The 310 patients with GDM and 440 normal pregnancy subjects selected for study were of Han Chinese ethnic origin. Between 2010 and 2014, subjects were recruited from the International Peace Maternity and Child Health Hospital affiliated with the Medical School of Shanghai Jiao Tong University and Bao’an Maternal and Child Health Hospital, Shenzhen, China. No previous diagnosis of chronic hypertension, type 1 or type 2 diabetes, infection, renal dysfunction, rheumatoid arthritis or systemic lupus erythematosus was reported in any case. GDM diagnosis was performed according to the International Association of the Diabetes and Pregnancy Study Groups criteria, 12 which later was also implemented by the World Health Organization (http://apps.who.int/iris/bitstream/10665/85975/1/WHO_NMH_MND_13.2_eng.pdf). Our study protocol was in accordance with institutional ethic guidelines and national laws. Informed written consent was obtained from all subjects. This study was approved by the Ethics Committees of the International Peace Maternity and Child Health Hospital affiliated with the Medical School of Shanghai Jiao Tong University and Bao’an Maternal and Child Health Hospital and conducted in accordance with the principles of the Declaration of Helsinki.
Study protocol
All subjects underwent a 75-g oral glucose tolerance test between 24 and 28 weeks of gestation to screen for GDM. Subjects were examined in the morning after a 12-h overnight fast between 08:30 and 09:30. Plasma glucose levels were measured at 0, 1 and 2 h during the glucose challenge. GDM was diagnosed in cases where one of the glucose values met or exceeded the threshold. Body mass index (BMI) for all pregnancies before delivery was calculated as the ratio of weight (kg) to the square of height (m2). 13 Large, appropriate and small for gestational age rates were recorded. Biochemical data, including plasma glucose, glycosylated hemoglobin A1c (HbA1c) and triglyceride levels, were additionally measured in all cases.
Genotyping
Genomic DNA samples were extracted from peripheral whole blood using the TIANamp Blood DNA kit (TIANGEN Biotech, Beijing, China). Genotyping was performed using SNaPshot (ABI Prism SNaPShot multiplex kit; Applied Biosystems) on an ABI PRISM 3730 genetic analyzer according to the manufacturer’s instructions and evaluated using ABI GeneScan software. Approximately 15% of the samples in our study were sequenced using an ABI PRISM 3730 genetic analyzer to reconfirm genotype. Reproducibility of data was 100%. The proportion of technically successful genotyping out of all samples assessed for genotype was 98%.
Primers for amplification were designed using Primer3 (http://frodo.wi.mit.edu/). All primers were synthesized by Sangon Biotech Co., Ltd. (Shanghai, China). Fragments of the variant were amplified from 100 ng DNA in a 20-µl reaction mixture containing 50 mmol MgCl2, 50 mmol dNTP, 1 µM forward primer, 1 µM reverse primer and 0.5 U Taq polymerase (TaKaRa). A touchdown PCR program was used according to the manufacturer’s instructions. The primer sequences for PCR amplification were as follows: forward 5′-CAACAGTGCTGCCTATTCCC-3′ and reverse 5′-TAGGAAAGGAGATGCCCTCA-3′.
Statistical analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences Windows version 17.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation and compared using the Student’s t-test. Association of the allele and genotype of the SNP with the disease was analyzed using Pearson’s χ2 test and OR (odds ratio). Deviation from Hardy–Weinberg equilibrium was assessed using the Chi-square test. All tests were two-sided, and a value of p < 0.05 was accepted as statistically significant.
Results
Clinical and biochemical characteristics of subjects
Demographic characteristics of the subjects
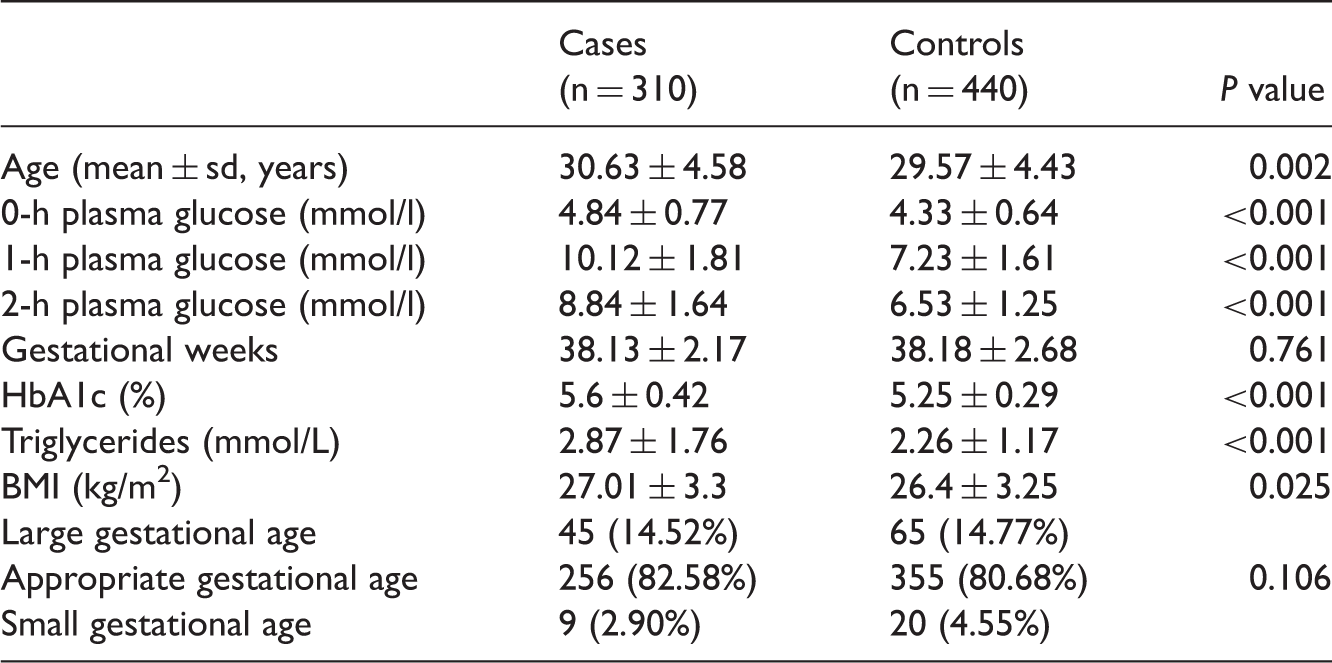
HbA1c: hemoglobin A1c; BMI: body mass index
Genotyping and allelic frequencies
The rs10229583 polymorphism genotypes and the risk of developing GDM
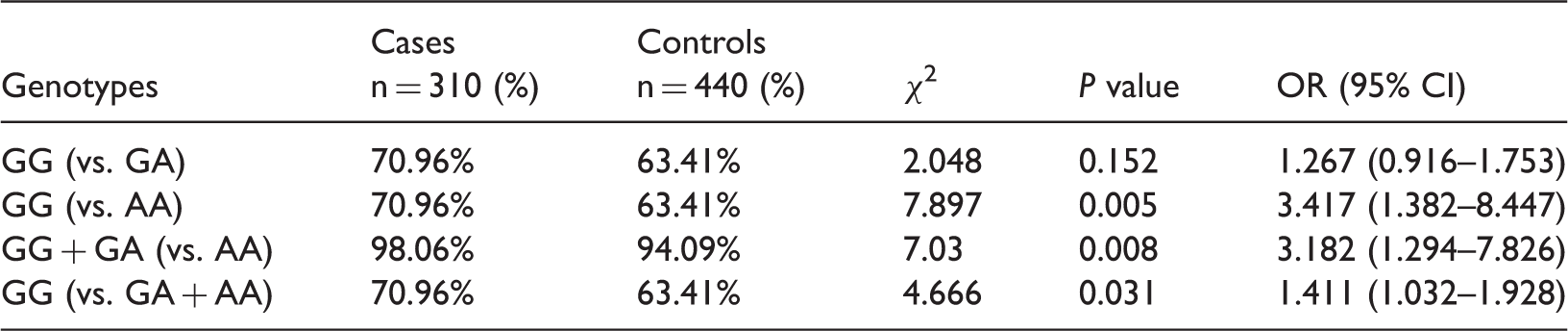
CI: confidence interval
The G allele was associated with GDM risk (OR = 1.47, 95% CI: 1.12–1.939, p < 0.005) (Table 2). The OR of the GA + GG genotype was 3.182 (95% CI: 1.294–7.826, p = 0.008), and that of the GG genotype was 1.411 (95% CI: 1.032–1.928, p = 0.031) for patients with GDM compared with controls. These data indicate that the G allele is a risk factor for GDM development.
Association of rs10229583 with clinical and biochemical characteristics in subjects with GDM
Association of SNP rs10229583 with clinical and biochemical characteristics in subjects with GDM

HbA1c: hemoglobin A1c; BMI: body mass index
Discussion
GDM is a multifactorial disease caused by the complex interplay of multiple genetic, environmental and immunologic factors.14–17 As GDM appears to share the same genetic background as T2D, candidate genes for GDM have been identified based on those associated with T2D. A number of genetic variants related to T2D are also reported to be associated with GDM. 18 Several genome-wide association studies have suggested that mutations or polymorphisms in PAX4 are associated with both type 1 and 2 diabetes.19–20 To clarify whether PAX4 is linked to GDM, we evaluated the possible association between the rs10229583 locus and GDM for the first time in this study.
Consistent with earlier findings, BMI and plasma glucose, HbA1c and triglyceride concentrations were significantly higher in subjects with GDM compared with those of normal controls. However, neonatal birth weight did not differ between subjects with GDM and normal controls. All pregnant women diagnosed with GDM in the clinic underwent diet and exercise therapy to ensure that weight before delivery and newborn birth weight were effectively controlled. Pharmacological therapy was also indicated in some cases to provide appropriate blood glucose control.
Our data revealed a significant association of the rs10229583 SNP with GDM. In particular, the G allele may be a risk factor for development of the disease. The relative risk for GA + GG was 3.182 (95% CI: 1.294–7.826, p = 0.008), while that for GG was 1.411 (95% CI: 1.032–1.928, p = 0.031) for patients with GDM. The rs10229583 polymorphism is located downstream of PAX4. While several studies to date have focused on the effects of PAX4 in the pathogenesis of T2D, to the best of our knowledge, none have addressed its potential association with GDM. PAX4 is a transcription factor belonging to the PAX family of proteins that contains a paired box domain, a paired-type homeodomain and an octapeptide involved in fetal development and tumor growth. PAX4 is expressed in early pancreatic endocrine cells, which is necessary for differentiation, development, proliferation and insulin secretion of pancreatic islet beta cells. The protein stimulates the expression of PDX1, a key transcription factor for islet development.21,22 Targeted disruption of PAX4 in mice has been shown to reduce beta-cell mass at birth. Shimajiri et al. reported that the R121W mutation in PAX4 is significantly associated with T2D. 11 Ma and colleagues identified an association of rs10229583 near PAX4 with elevated fasting plasma glucose and impaired beta-cell function in controls and earlier age at diagnosis in Chinese populations. 23 Moreover, the rs10229583 locus was associated with T2DM in a Mongolian population in China. 24
To determine the functional implications of the rs10229583 SNP in GDM, we performed an association analysis between these variants and biochemical characteristics. Notably, the GG genotype of rs10229583, the risk variant for GDM, was not associated with BMI, neonatal birth weight or plasma glucose, HbA1c or triglyceride levels. Further research is required to elucidate the precise mechanisms by which these loci contribute to GDM susceptibility.
In conclusion, rs10229583 near PAX4 has been identified as a novel locus associated with GDM in Chinese populations, providing further insights into the pathogenesis of this disease.
Footnotes
Acknowledgements
We are grateful to all the subjects for their ongoing participation.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by a grant from the Shenzhen Municipal Science and Technology Innovation Council (grant no. JCYJ20150403105513698).