
Abstract
Objectives:
The study aims were to evaluate the contribution of sonoelastography to Breast Imaging Reporting, and Data System (BI-RADS) scoring of breast images.
Materials and Methods:
Two observers evaluated the BI-RADS category, Tsukuba score, and the strain index of 83 lesions of 73 consecutive patients. A new scoring system was established to evaluate the lesions by using the BI-RADS score, Tsukuba score, and strain index ratio.
Results:
There was a statistically significant difference between the strain index value of benign (3.08 ± 2.71) and malignant group (4.62 ± 2.70) (P < .05). The sensitivity and specificity were 59.1% and 65.1% for the 3.12 cut-off value for the strain index. In the receiver operating characteristic (ROC) analysis, the area under the curve (AUC) of the only BI-RADS score was 0.834, both BT (BI-RADS + revised Tsukuba score) score and the total score (BI-RADS + revised Tsukuba score + strain index score) was 0.843. The interclass correlation coefficient for the two observers’ measurements of the strain index was weak, with .266 (P < .05).
Conclusion:
The potential contribution of sonoelastography on lesion characterization is still controversial. In this study, the agreement among the observers was inadequate, and the contribution of sonoelastography on BI-RADS classification was limited. In addition, in the daily practice of sonoelastograpic evaluation, the Tsukuba score, was easier to apply and should be used rather than strain index measurements.
Breast lesions are described according to the American College of Radiology, Breast Imaging Reporting, and Data System (BI-RADS) to standardize breast imaging results. Besides sonographic and mammographic imaging features, sonoelastography findings are also added to the BI-RADS lexicon. 1 Lesions are described by their elasticity as soft, intermediate, or stiff. 2 In addition to the conventional ultrasonographic (US) features of the lesion, the malignancy risk of a lesion can be predicted with the evaluation of the sonographic lesion stiffness.3–5 Elasticity imaging provides complementary information to conventional imaging by providing an evaluation of the lesion stiffness, a measurable feature of a tissue. 6
Elasticity is described as the rate of tissue displacement resulting from a certain amount of pressure on the tissue.7,8 The principle of sonoelastography is based on creating a stress force on a tissue, which causes an internal displacement difference according to the tissues’ elastic properties. This modality uses the same principles as manual palpation that have been used for hundreds of years to detect stiffness in soft tissue.7,9 Therefore, the primary clinical usage of the sonoelastography is based on the difference of stiffness between benign and malignant lesions.7,10 Malignant tumors are stiffer than benign lesions due to the extensive desmoplastic reactions with increased connective tissue production. Also, intercellular junctions in malignant lesions cause increased fibrosis and cell density alterations resulting in stiffness of lesions.7,9,10
Sonoelastography can be performed during an US examination and helps to determine tissue elasticity features in vivo as it is first described in the 1990s.1,7,8 Today, two main kinds of sonoelastography techniques are available as strain elastography (SE) and shear wave elastography (SWE). 11 In the SE technique, external tissue pressure is used to measure tissue stiffness, while in the SWE technique, compressive acoustic waves are used.7,12 The measurement of the tissue displacement (strain) in SE is performed with a transducer by manually applying repetitive pressure to the tissue. SE provides information about the relative stiffness of a lesion to surrounding tissue. It is defined as strain ratio which is qualitative data. During the pressure application, a stiffer malignant lesion than the surrounding tissue shows less strain than the surrounding soft tissue. So, measuring the strain of the lesion and surrounding healthy tissue using region of interest (ROI) gives us strain ratio and information about the stiffness of the lesion.9,12 In SWE, compressive acoustic waves are used to induce shear waves, and the waves are tracked. Measurement of the shear wave reveals both qualitative and quantitative (absolute elasticity value of soft tissues) data of the tissue elasticity.13,14 Currently, three technical approaches are used as 1-dimensional transient elastography (1D-TE), point shear wave elastography (pSWE), and 2-dimensional shear wave elastography (2D-SWE). 12
In the SE technique, after having a stable sonoelastogram, three primary methods are used to classify the lesions. One of them is the Tsukuba score classification, which depends on the lesions’ color pattern analysis. The other one is strain ratio, which gives us a semiquantitative assessment by measuring the strain value of both the lesion and the reference tissue within ROI. To measure strain value of the lesion, ROI should be placed at the same depth for both the reference tissue and the target lesion. The strain ratio is calculated by dividing the strain of the reference tissue into the strain of the lesion by the US software. The other method is the width ratio (EI/B ratio), which is based on the logic that malignant lesions are seen as larger in sonoelastography images than in B-mode US. The ratio of sonoelastography image size (EI) and B-mode size (B) is used in this method.9,12
B-mode sonography has a high sensitivity but lower specificity in the evaluation of solid breast masses, which causes high rates of false positivities. The breast lesions with a malignancy suspicion more than 2% undergo a biopsy. This fact causes unnecessary biopsies that result in benign histopathology. 1 Doppler sonography and sonoelastography can be added to the examination to improve the specificity of the B-mode sonography.15,16 Some studies have shown that sonoelastography increases the B-mode sonography’s specificity in the differentiation of benign-malignant lesions without extra cost or time.3,16–19 The aim of this study was to evaluate the contribution of sonoelastography to BI-RADS scoring by using Tsukuba scores, strain index ratio. It was envisioned as an easily applicable new scoring method for sonoelastography.
Materials and Methods
Women, more than 18 years of age, who had a breast biopsy between January 2017 and January 2018 at the host hospital, were invited to this study. The imaging was performed by the same radiologist, throughout this study. Patients having BI-RADS 3, 4, and 5 lesions were evaluated before the biopsy procedure by two observers, using a real-time B-mode US and sonoelastography. Both observers evaluated the patients blinded to each other. There were a total of 85 lesions in consecutive 73 patients. Breast US and sonoelastography were performed on a Toshiba Aplio 500 (Toshiba Medical System Corporation, Tokyo, Japan) with a 7 to 12 MHz probe before the biopsy. Each observer evaluated the patients using sonography initially and sonoelastography afterward. Sonography and sonoelastography images were obtained by both observers independently (Figure 1). The observers were radiologists with 15- and 10-year experience, respectively, and one observer specialized in breast imaging.
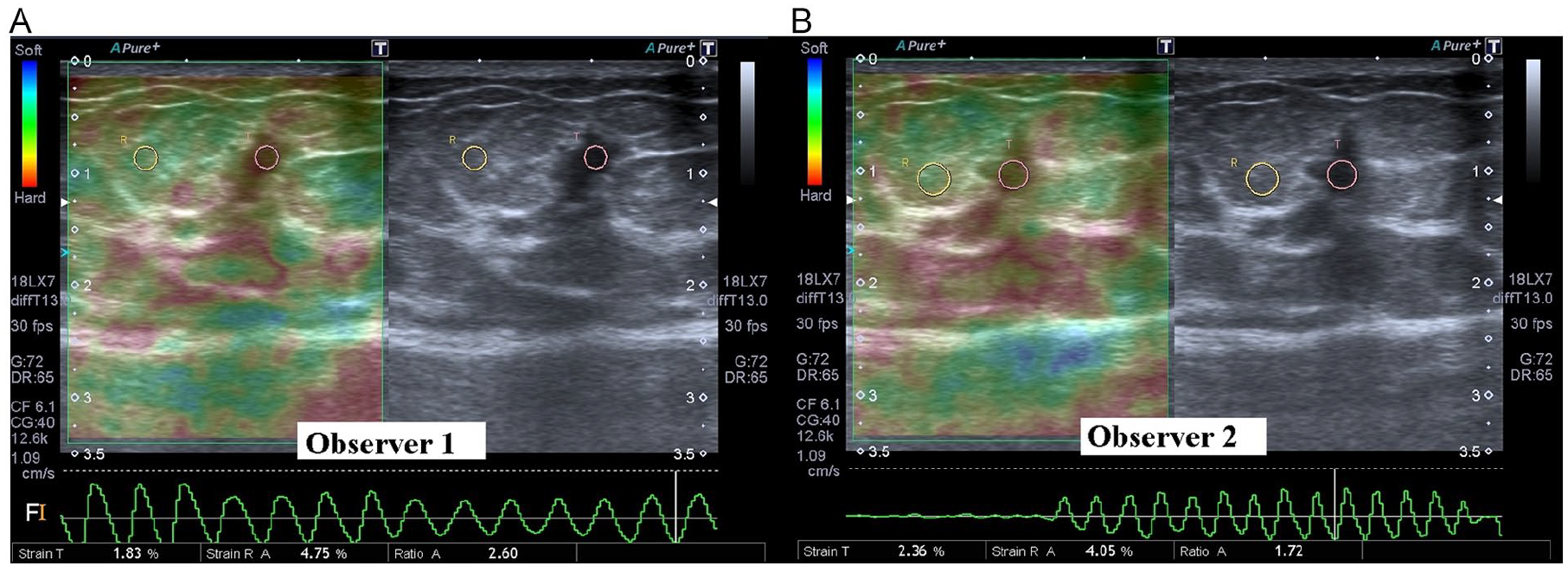
The two observers evaluate all lesions blind to each other: (A) The first observer’s sonoelastography image and strain ratio measurement of the lesion and (B) The sonoelastography evaluation of the same lesion by the second observer.
The exclusion criteria included patients who were male, below 18 years of age, and patients who had non-mass-like lesions on US or had the only microcalcification without occupying mass in sonography. The lesions greater than 5-cm diameter or located deeper than 2 cm from the skin were also excluded from the study. The widest, narrowest diameter, the average size, depth, and location of the lesion were recorded.
Both observers performed the real-time US and BI-RADS scoring concerning the sonographic features of the lesion. 1 Per shape, margin, echo pattern, posterior acoustic features, and accompanying microcalcification features of the lesion, each lesion was classified with a final BI-RADS score using B-mode sonography. Malignancy probability of the lesions was considered as BI-RADS 3 with probably benign nature, BI-RADS 4 with low suspicion for malignancy, and BI-RADS 5 with high suspicion for malignancy. Oval-shaped lesions with well-defined margins, parallel orientation, and echogenicity less than fat tissue, with or without minimal posterior acoustic enhancement, were categorized as BI-RADS 3. Lesions that were spiculated, with a height greater than the diameter, markedly hypoechoic, having posterior shadowing, with or without accompanying microcalcifications, were categorized as BI-RADS 5. The lesions having other sonographic features than BI-RADS 3 and 5 were categorized as BI-RADS 4 (such as heterogeneous masses without circumscribed margin). 20
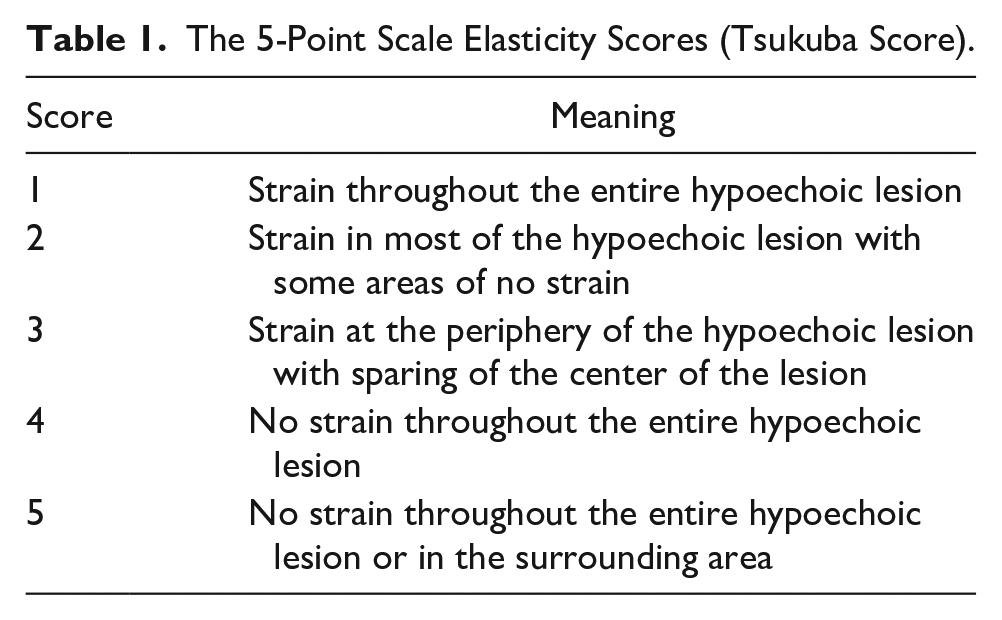
SE evaluation and measurement of strain ratio was performed twice by both of the observers to all of the patients after B-mode sonography. After placing the target lesion in the center of the image, the lesion was compressed vertically using the transducer. Compression was applied with an up and down motion of the probe, as the pressure was adjusted to remain between the two reference lines determined by the manufacturer. So, the observers could provide similar compression amounts and pressure curves in each compression cycle. Compression cycles continued until obtaining at least five similar curves to have a stable elastogram map. On these maps, observers evaluated lesions using the Tsukuba score (Table 1).18,21 After the scoring, strain index ratios were measured using a circular ROI with a 5-mm diameter.9,12 The ROIs were replaced on both the target lesion and the reference tissue. Subcutaneous soft tissue, which was at the same depth as the target lesion, was set as the reference tissue (Figure 2).
The 5-Point Scale Elasticity Scores (Tsukuba Score).
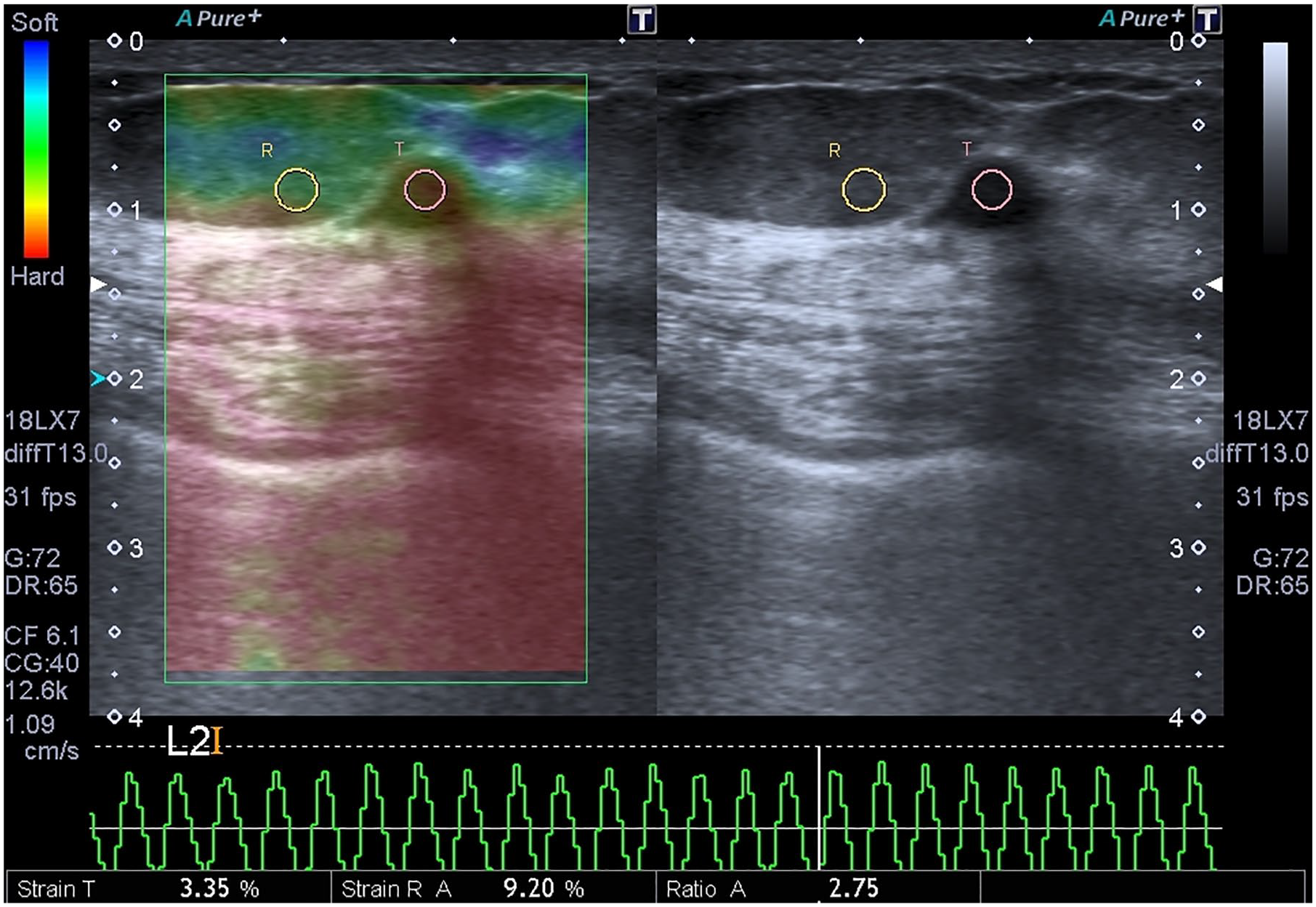
The ROIs are replaced on both the target lesion and the reference surrounding soft tissue at the same depth. ROI, region of interest.
After two observes evaluated BI-RADS scores and Tsukuba scores, these results were examined for consistency with each other. If the BI-RADS scores of the two observers were compatible, the result was accepted as the BI-RADS score of a lesion. However, if the BI-RADS scores of the two observers were different, the higher score was accepted as the final score. The same methodology was also used for obtaining the final Tsukuba scores.
BI-RADS results were scored in a similar way to previous studies, 22 and the scoring scheme was as BI-RADS 3 were converted to 0 points, BI-RADS 4 to 1 point, and, BI-RADS 5 to 2 points. Moreover, as one of the study contributions, a new scoring system was developed using the Tsukuba score (revised Tsukuba score). The revised Tsukuba system was designed to map original Tsukuba scores of 1, 2, or 3 to 0 points, 4 or 5 to 1 point. A strain index cut-off value was determined to differentiate malignant and benign lesions. The values below the cut-off value were scored as 0 points, and values above were scored as 1 point (Table 2). BI-RADS score, BT score (BI-RADS + revised Tsukuba score), BS score (BI-RADS + strain index score), TS score (revised Tsukuba score + strain score), and the total score (BI-RADS + revised Tsukuba score + strain score) were obtained for each lesion.
The New Image Scoring System and Associated Points.
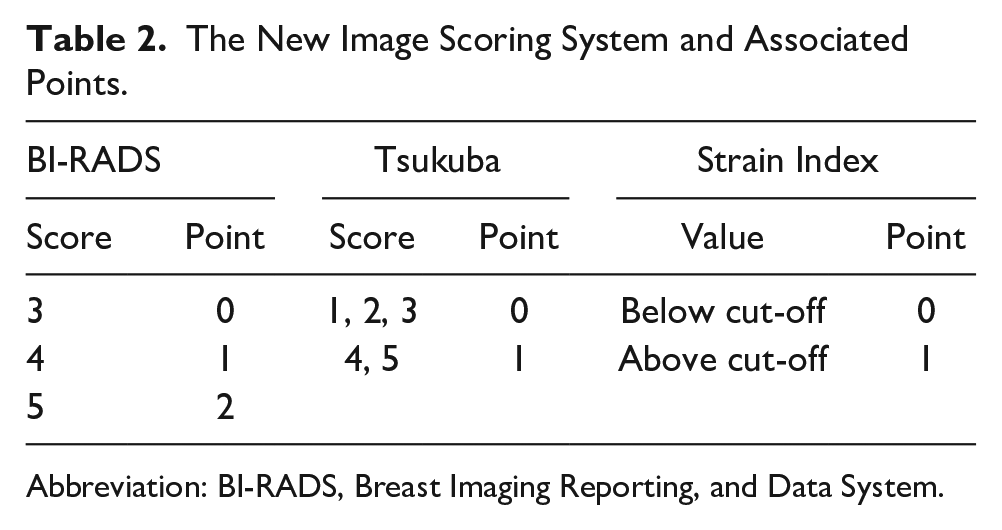
Abbreviation: BI-RADS, Breast Imaging Reporting, and Data System.
All patients signed informed consent before the sonography, sonoelastography, and breast biopsy. Ethical approval was granted by the local Institutional Ethics Committee (number: 1900019).
Statistical Analysis
SPSS 16.0 (SPSS Inc., Chicago, IL, USA) for Windows package program was used in the analysis. Descriptive analyses were performed to evaluate demographic data. Independent-samples t test was used for the normally distributed parameters such as strain index values. The sensitivity and specificity of BI-RADS classification, revised Tsukuba score, strain index, and combination of three scoring systems were calculated. Mann-Whitney U test was used to compare the mean values of the groups. A receiver operating characteristic (ROC) curve was generated, and the area under the curve (AUC) was measured for each scoring system. After obtaining the ROC curve, the highest sensitivity and specificity were determined as the cut-off value. The intraclass correlation coefficient (ICC) was calculated to evaluate the reliability between the two observers’ measurements. The Cohens-Kappa analysis evaluated the compatibility of the two observers for all scores previously mentioned. A P value of <.05 was considered statistically significant.
Results
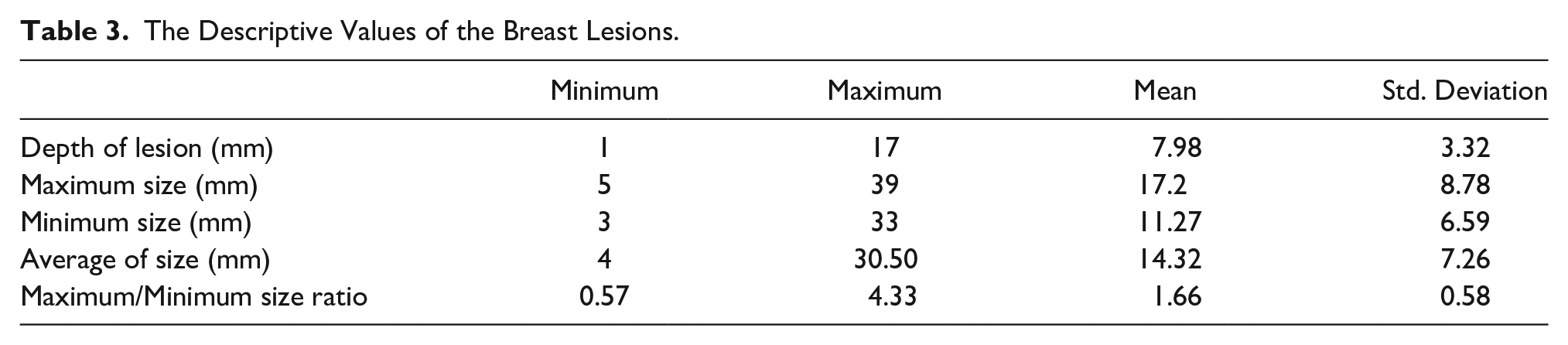
The mean age of the 73 participants was 45.55 ± 11.22 (between 16 and 76 years). The lesion size and depth are shown in Table 3. Thirty-nine of the lesions (45.9%) were on the right breast, and 46 (54.1%) were on the left breast. Distribution of breast lesions according to breast quadrants was as 46 lesions (54.1%) in Upper-Outer (UOQ), 11 (12.9%) in Lower-Outer (LOQ), 10 (11.8%) in Upper-Inner (UIQ), and 18 (21.2%) in Lower-Inner (LIQ) quadrants. While 63 (25.9%) of the lesions were benign, 22 (74.1%) were malignant. The distribution of the histopathology results and BI-RADS scores of the patients are shown in Table 4. BI-RADS scores were upgraded in 25 lesions due to the lack of interobserver compliance. According to the Tsukuba scoring system, the score was upgraded in six patients due to the lack of interobserver compliance. Both observers were concordant with the scores except for these upgraded scores.
The Descriptive Values of the Breast Lesions.
The Distribution of the Histopathology Results and BI-RADS Scores.
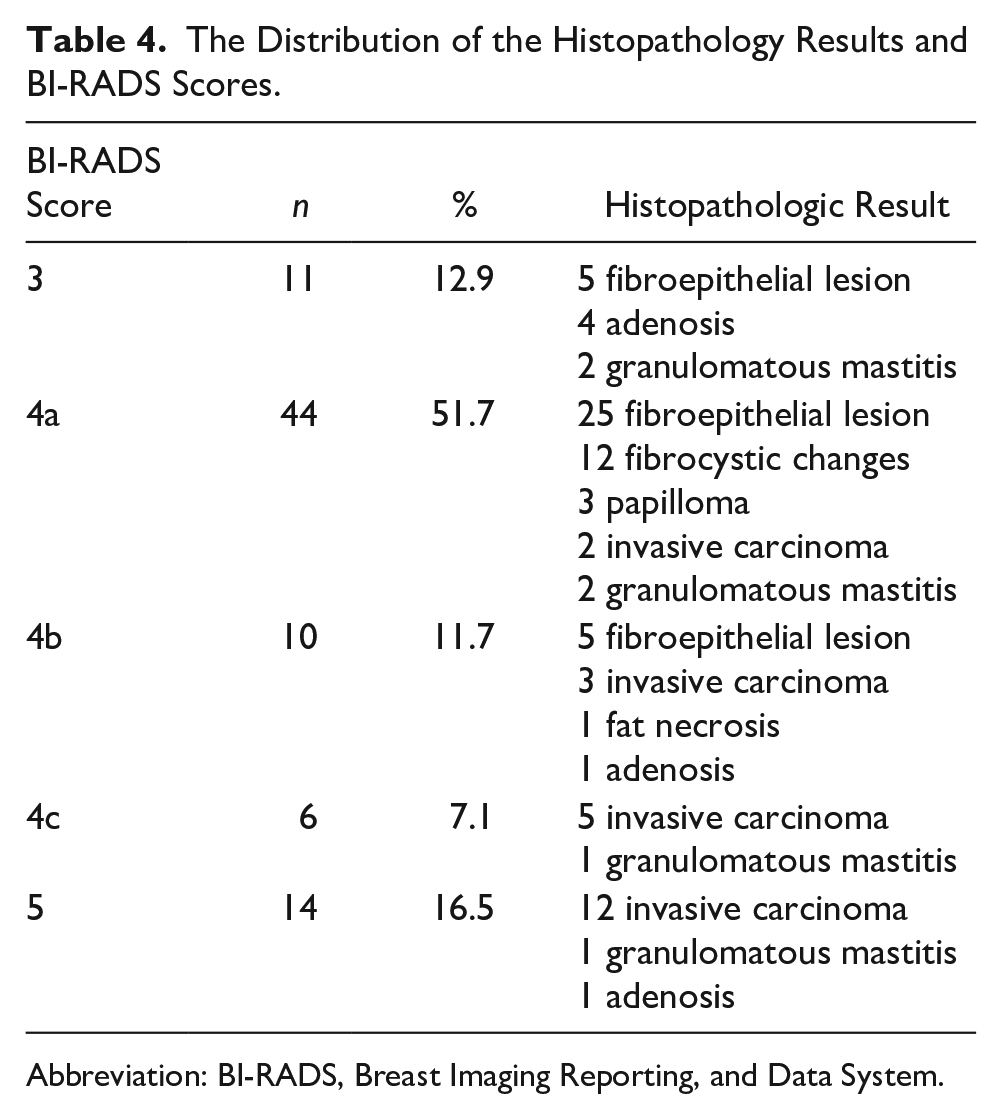
Abbreviation: BI-RADS, Breast Imaging Reporting, and Data System.
While the mean strain value of benign cases was 3.08 ± 2.71, it was 4.62 ± 2.70 in the malignant lesion group (Figure 3). The difference between the two groups was statistically significant (P < .05). The sensitivity and specificity were 59.1% and 65.1% for the 3.12 cut-off value, respectively. Therefore, patients with an elasticity value of less than 3.12 cut-off point were scored as 0 points, and the values above 3.12 were scored as 1 point (Figure 4). The sensitivity and specificity were 82.5% and 72.7%, respectively, for the revised Tsukuba scores.
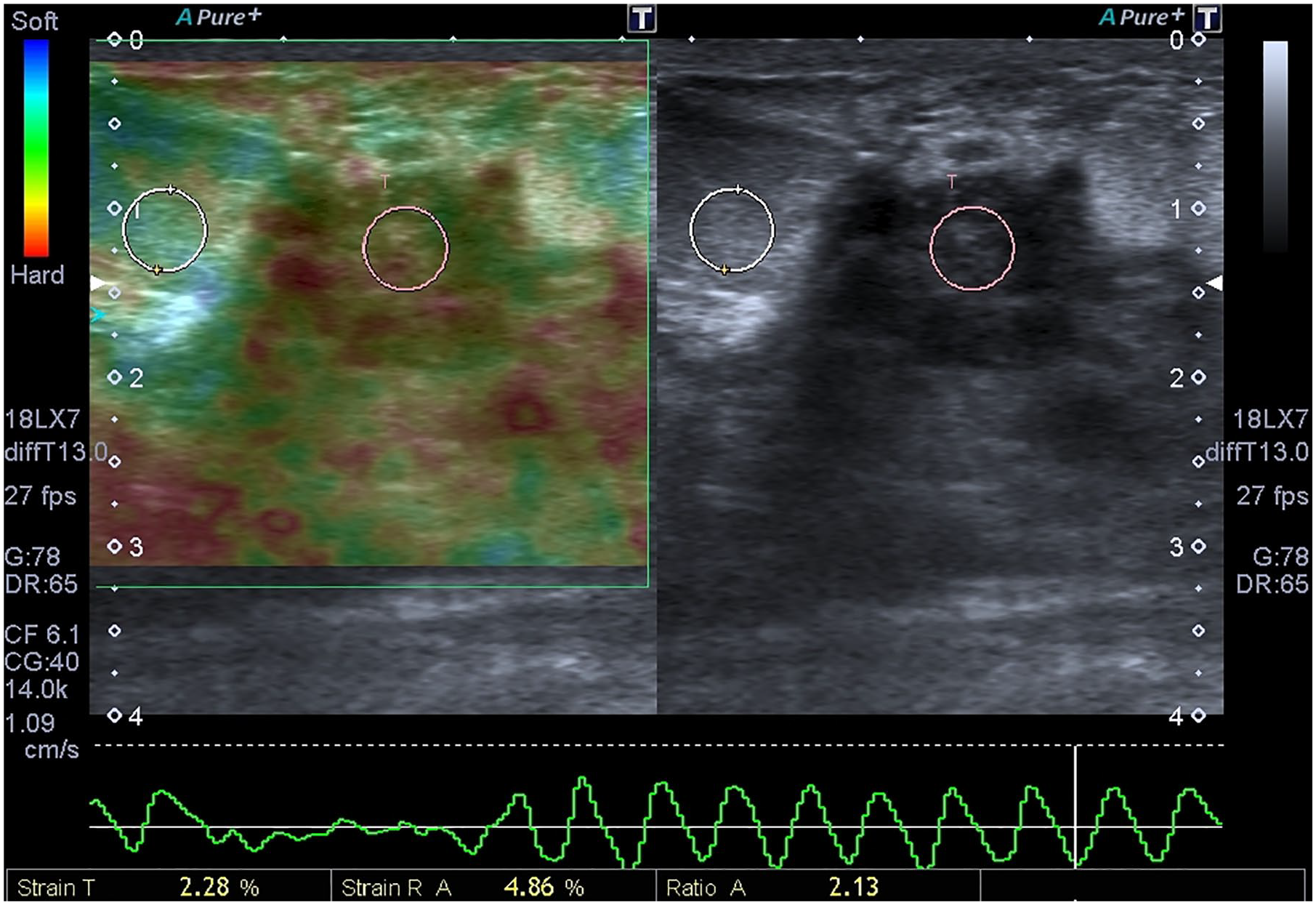
Both observers evaluate this hypoechogenic heterogeneous lesion as BI-RADS 4a and the strain ratio measured once by one of the observers is 2.13. The mean strain ratio measurements of two observers of this mass is 2.62 which is below the cut-off value. The histopathologic report reveals granulomatous mastitis after percutaneous core biopsy. BI-RADS, Breast Imaging Reporting, and Data System.
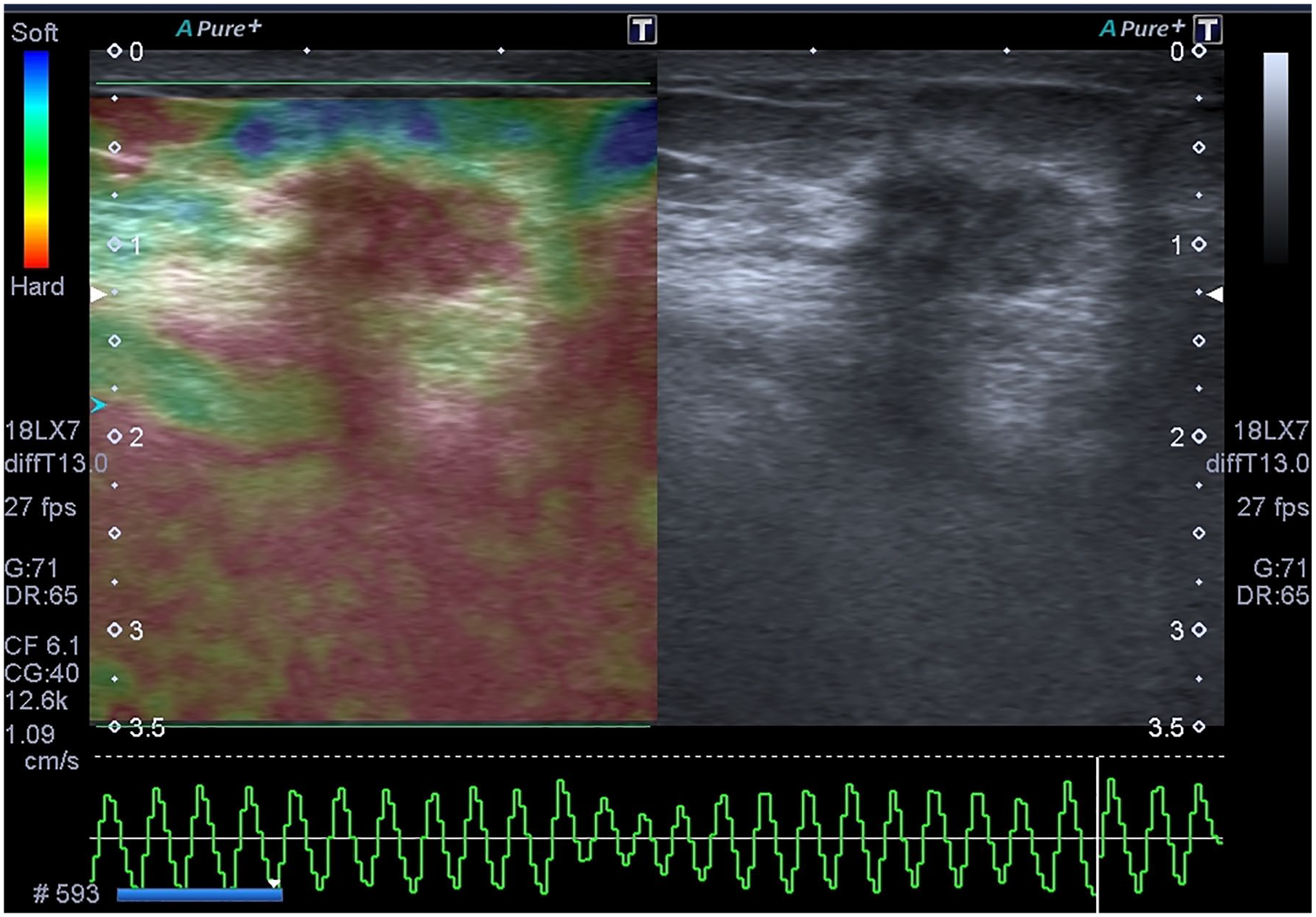
Sonoelastography image of a 47-year-old woman with a palpable mass on her left breast was seen. Both observers evaluated lesion as BI-RADS 5 and Tsukuba score 5. The strain index ratio of this measurement was 3.51, and the mean ratio of both observer’s measurements was 3.91 of this lesion. BI-RADS, Breast Imaging Reporting, and Data System.
The difference between the mean scores of the benign and malignant lesion groups was statistically significant in all scoring systems except strain ratio scorings (P < .05) (Table 5). In the ROC analysis, the AUC of the BI-RADS score was 0.834. The AUC of BT score and the total score was above the BI-RADS score and 0.843 (Figure 5).
The Mean Scores of the Benign and Malignant Lesion of All Scoring Systems.
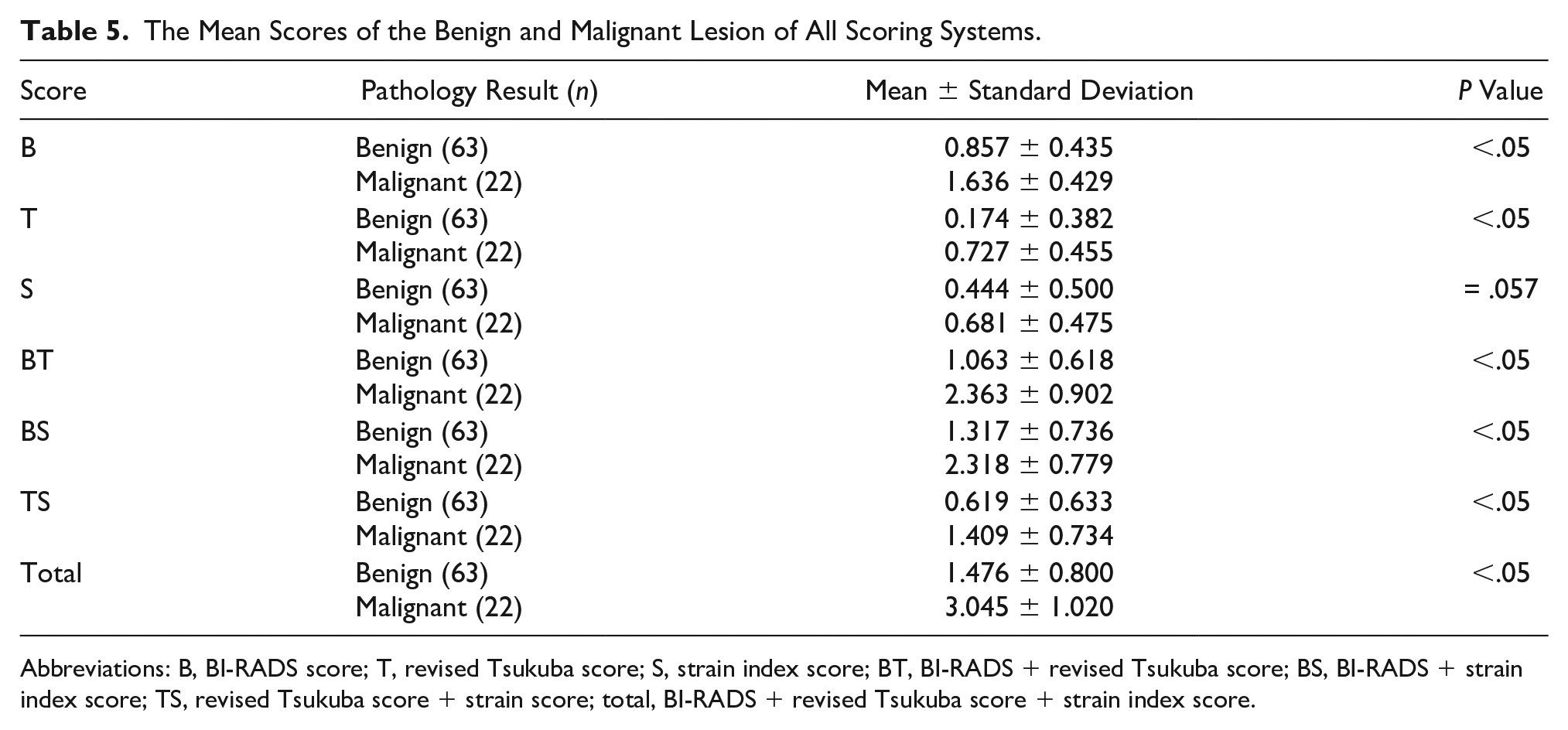
Abbreviations: B, BI-RADS score; T, revised Tsukuba score; S, strain index score; BT, BI-RADS + revised Tsukuba score; BS, BI-RADS + strain index score; TS, revised Tsukuba score + strain score; total, BI-RADS + revised Tsukuba score + strain index score.
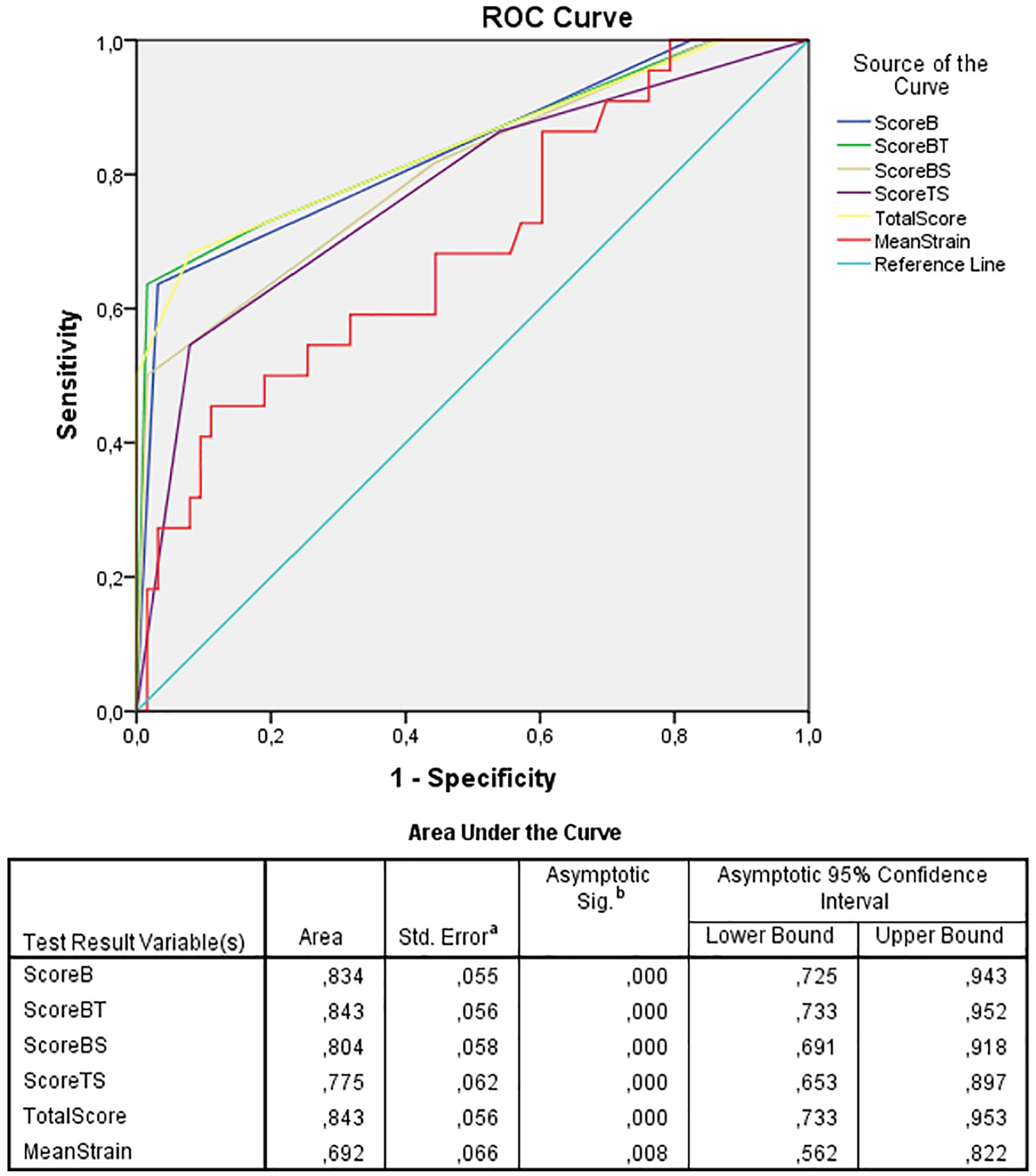
ROC analysis, the AUC of the BI-RADS score, BT score, BS score, TS score, and total score including all three variables. ROC, receiver operating characteristic; AUC, area under the curve; BI-RADS, Breast Imaging Reporting, and Data System; BT score, BI-RADS + revised Tsukuba score + strain index score; BS score, BI-RADS + strain index score; TS score, Tsukuba score + strain index score.
The ICC calculated for both of the two observers’ SE index measurements was poor with .266 (P < .05). For Tsukuba scoring, the agreement between observers was moderate, ĸ = .51 (P < .000), while the analysis for grouped Tsukuba scores was substantial, ĸ = .71 (P < .000). In BI-RADS scoring, in which two groups were formed as one group for 3 and 4a with the benign probability, and one group for 4b, 4c, and 5 with high malignancy probability, the agreement between the observers was adequate in grouped BI-RADS scoring, ĸ = .88 (P < .000).
Discussion
In this study, the contribution of SE to BI-RADS classification was evaluated. Although it was easy to apply after the B-mode US, the results revealed that for both revised Tsukuba scoring and strain index values, they did not significantly contribute to BI-RADS classification, for distinguishing between benign and malignant lesions. The AUC of the BI-RADS classification according to the lesion’s US features was 0.834, the BT score and the total score AUC were both 0.843, and the contribution of sonoelastography to BI-RADS scoring in the diagnosis was minimal.
The mean strain value was 3.08 in benign lesions, and 4.62 in malignant lesions. In a study held with 181 lesions, the mean strain value was found as 2.61 in the benign lesions, and 3.73 in malignant lesions. 15 Although the elasticity scores measured with SE were significantly higher in malignant lesions, their sensitivity (59.1%) and specificity (65.1%) for the 3.12 cut-off value were not high. Moreover, there was no significant contribution of strain index ratios to BI-RADS classification in our study. In the study of Parajuly et al, the mean strain value measured was 1.87 in benign lesions and 7.9 in malignant lesions. In this study, sensitivity and specificity were measured as 94.6 and 94%, respectively, for the 3.54 cut-off value. 23 In the study held by Cho et al, sonoelastography strain index ratio was used to differentiate benign and malignant results in nonpalpable breast lesions, and the mean strain index for benign and malignant lesions was found as 2.63 ± 4.57 and 6.57 ± 6.62, respectively. In this study, sensitivity and specificity were calculated as 95% and 75% for the 2.24 cut-off value. 17 The sensitivity and specificity values of both studies were higher than our study. Also, the cut-off values of malignant lesions in both studies were high compared with our study, and the mean strain values and cut-off values of benign and malignant lesions were different in both studies. The standard deviations of the study conducted by Cho et al were very high. 17 This fact was related to the user and experience-dependent nature of sonoelastography. In the literature, a meta-analysis showed that the cut-off values for strain ratio in breast lesions varied between 2.27 and 4.5. 24 The main reason for the different cut-off values is associated with differences in the placement of the ROI. Also, inter-manufacturer differences in both technologies of the SE and display scale variability limit the comparability of images and values of SE. 13 We believe that standardization in SE technology and software can ensure similar results in different centers.
SE is performed manually by compressing and releasing the tissue. In SE, rather than a certain numerical value of the lesion’s stiffness, a ratio is used by comparing the stiffness of the lesion with the normal soft tissue at the same level. This evaluation constitutes many relative steps in the measurement of strain index. This technique requires experience, and the learning curve slope is high. Therefore, its reproducibility has been reported as poor previously. 25 The differences in the users’ manual compression caused poor compliance between the two observers in our study. Besides, sensitivity and specificity were found to be low in the present study due to the nature of sonoelastography performed by manual compression. The presence of different cut-off values in different studies and different mean values for benign and malignant lesions show that strain index values are user- and device-dependent. So, if SE is desired to be used in daily practice, values for each device and user must be determined. Also, each operator’s learning curve should be determined before using this modality in differentiating benign-malignant breast lesions.
In a meta-analysis focusing on SE’s diagnostic differentiation performance for benign and malignant breast lesions, the overall mean sensitivity and specificity values were found as 0.834 and 0.842 for the Tsukuba score, respectively. For strain ratio sensitivity and specificity, values were found to be 0.883 and 0.814. 24 In another meta-analysis, using pSWE to differentiate benign and malignant lesions, the overall sensitivity was 0.84, and specificity was 0.94. 26 The sensitivity and specificity of the SE and SWE were similar to each other in literature. Our study’s sensitivity of the revised Tsukuba score was similar to the literature, but the sensitivity and specificity values of strain ratio were lower than the literature. This result may be caused by the lack of a user’s experience or the technical features of the device used. In a study, it was shown that using a computer-aided diagnosis (CAD) system provides higher diagnostic accuracy and interobserver agreement in breast sonoelastography. 27 Also, devices such as footplate extenders may improve the uniformity of the applied pressure. 28 The usage of devices and software to standardize external compression might help the reproducibility of the sonoelastography.
In this study, it was not possible to find a significant contribution of SE on BI-RADS scoring alone in differentiating malignant and benign breast lesions. However, a study using a 2D SWE had shown that combined SWE and BI-RADS scoring had a better diagnostic performance compared with BI-RADS scoring alone. 3 Therefore, the contribution to BI-RADS scoring in determining malignant tumors, SWE might be more beneficial due to its technology. Further studies are needed to examine and compare SE and SWE values on phantoms and real cases.
Although the ICC for the two observers for strain ratio was poor, it was substantial for the revised Tsukuba scores. This finding demonstrates that different practitioners may report similar results more frequently by using the revised Tsukuba scoring than the strain index ratio.
There were some limitations to the present study. The first was the difficulty of applying SE due to manual compression. Although the device’s software showed the amount of compression to standardize the compression amount in real-time, the same compression pressure may not be accomplished for every case. Further training in the usage of sonoelastography or performing multiple measurements for each patient may make the sensitivity and specificity values more optimal. Second, breast structure and the depth of the lesion may also affect the amount of compression and response to compression. However, we did not use these data in the analysis. Also, the study sample size was limited, and this only allowed for evaluating certain types of malignant lesions. Another important limitation was that the evaluation was held with SE, which was user-dependent and had less operator compliance. Further prospective study series should be designed with SE and SWE to determine the ideal sonoelastography method in evaluating breast lesions. Besides, learning curves and the compliance between the observers should be evaluated separately for the first half of the consecutive patients and the last.
This study showed that a combination of strain index values, revised Tsukuba scoring, and conventional US had a minimal contribution to BI-RADS scoring in differentiating benign and malignant breast lesions. If sonoelastography is to be used in daily practice, it would be appropriate to prioritize the revised Tsukuba scoring system. It would be due to it being easier and more practical than strain index measurements, and there is more consistency between the observers in revised Tsukuba scoring.
Conclusion
The potential role of sonoelastography in lesion characterization is still controversial. In this study, the reliability among the observers was poor, and its contribution to BI-RADS classification was limited. Since it is a user-dependent method, optimal measurement standards shall be investigated further. If sonoelastography is chosen for lesion evaluation, the Tsukuba method should be preferred, over the strain index measurement.
Key Takeaways
Despite low interobserver compliance and limited contribution to BI-RADS classification in determining malignant breast lesions, sonoelastography is a practical method to evaluate breast lesions and can be easily applied simultaneously with sonography.
In the SE technique, the revised Tsukuba scoring has good interobserver compatibility, which can be applied more easily, and is preferable to the strain ratio measurement in daily practice.
Footnotes
Ethics Approval
Ethical approval for the study was granted by the institutional review board.
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because of the study design.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial registration
Trial registration was not applied due to study type.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.