
Abstract
Objective:
To determine whether the assessment of umbilical cord diameter (UCD) is a viable indicator of fetal growth and perinatal outcome.
Material and Methods:
A total of 652 singleton pregnancies between 10 and 40 weeks of gestation were reviewed for this study. The UCD was measured vertically in the longitudinal section, adjacent to its insertion at the fetal abdomen. Other fetal biometrics were measured according to standard measurement protocols. The perinatal outcome of each patient case was also recorded.
Result:
The UCD ranged between 0.73 and 1.68 cm, and correlated positively with gestational age, estimated fetal weight (r = 0.779, r = 0.639, P < .05), and other fetal biometrics. The UCD of 50 subjects was 2 standard deviations below the mean and correlated significantly (r = 0.712, P < .05) with poor fetal outcome in the first and second trimester. Observational studies of 50 subjects, whose UCD was 2 standard deviations below the mean, resulted in 21 cases of intrauterine fetal death, 10 cases of preeclampsia, 8 cases of oligohydramnios, and 11 cases of intrauterine growth restriction.
Conclusion:
The UCD has the potential to serve as an important indicator of fetal growth, well-being, and perinatal outcome.
The umbilical cord is physiologically and genetically part of the fetus and contains two arteries and one vein buried within Wharton’s jelly. The vein supplies the fetus with oxygenated nutrient-rich blood from the placenta. Conversely, deoxygenated and nutrient-depleted blood is supplied through the umbilical arteries back to the placenta. 1 Fetal growth and birth weight depend on the efficient delivery of nutrients from the mother to the fetus through the umbilical cord. The developmental integrity and function of this cord are essential considerations for fetal growth and well-being. 2 The definitive umbilical cord is visible, with sonography, from approximately 8–10 weeks of gestation, and the cord diameter could be sonographic criterion for assessing maternal and fetal health.
The umbilical cord diameter (UCD) is measured in a plane adjacent to the junction of the umbilical cord and fetal abdomen and has been reported to demonstrate a linear relationship with fetal growth. 3 Notwithstanding, this measurement may be affected by conditions such as fetal and umbilical cord anomalies, polyhydramnios, and oligohydramios. In addition, maternal disease conditions such as hypertension, diabetes, and anemia are thought to potentially affect UCD.
Appropriate assessment of fetal growth rate and health is essential for maternal/fetal care and could assist obstetricians to properly counsel women who are at risks of a preterm delivery and a postdate pregnancy. 4 Accurate knowledge of these and other maternal serum markers is required in the assessment of fetal anomalies. They may also indicate insufficiency and possible fetal distress.
A study has shown a varying degree of accuracy in the estimation of gestational age (GA), using traditional sonographic metrics such as biparietal diameter (BPD), femur length (FL), abdominal circumference (AC), and head circumference (HC). 5 Information from institutional data and observations shows a significant number of intrauterine fetal demise (IUFD) and fetal intrauterine growth restriction (IUGR), but the value of UCD in fetal well-being and perinatal outcome is underresearched. The aim of this study was to assess UCD as an indicator of fetal growth and perinatal outcome.
Materials and Methods
A prospective, cross-sectional analytical design was executed. After excluding all patient cases that did not meet the inclusion criteria, a total of 652 patient cases were retained for analysis. Patients with an uncomplicated pregnancy, at a GA of 10–40 weeks, and attended a sonography clinic in a Nigerian health care were characteristics of this convenient study sample. The period for this investigation was between June 2018 and May 2019. The inclusion criteria were based on pregnant women with a known last menstrual period, no history of diabetes, without drug/substance abuse, and a singleton pregnancy without congenital anomalies. Maternal patients with abnormal conditions such as gestational diabetes, hypertension, and anemia were excluded from the study.
All examinations were performed by a well-experienced sonographer using either the Siemens SONOLINE Omnia ultrasound imaging system (model: Cc-H3 170) or an Aloka ProSound (model: 3500SX) ultrasound machine. Both ultrasound devices were fitted with a curvilinear 3.5-MHz transabdominal probe. The patient was asked to lie in a supine position, and scanning was conducted in a variety of imaging planes. The UCD was measured vertically in the longitudinal plane, adjacent to the insertion at the fetal abdomen (Figure 1). The measurement was completed by placing the equipment’s electronic calipers from the outer to outer borders of the cord, in the longitudinal plane. In this way, it was possible to measure the greatest diameter of the cord. The crown-rump length (CRL) of each fetus was also measured. The BPD, FL, HC, and AC were all measured according to standard protocols. All measurements were taken twice, with the average values documented for statistical purposes. The mean and the mean ± 2 standard deviation values for the UCD were computed at two-weekly intervals. The BPD measurement of each fetus was taken between 14 and 40 weeks of gestation. The estimated fetal weight (EFW) was automatically calculated by the ultrasound system (using the machine software), based on the BPD, FL, HC, and AC measurements. IUGR was considered to be present when the EFW was below the fifth percentile for GA.

This cross-sectional sonographic image of the fetus and umbilical cord demonstrates the method of measuring the umbilical cord diameter.
Data Analysis
Data generated were transferred onto a Microsoft Excel for data analysis. The statistical mean and range of UCD, based on GA categories, were estimated. The Shapiro-Wilk test for normality and parametric analyses were conducted to determine whether the data were normally distributed. A Pearson correlation analysis was performed to investigate the relationship between UCD and GA, EFW, BPD, HC, FL, and AC. All statistical analyses were performed using Statistical Package for Social Sciences (SPSS) version 20.0, and statistical significance was set a priori at P ≤ .05.
Results
The UCD ranged from 0.73 to 1.68 cm for GAs between 10 and 40 weeks. It correlated positively with GA and EFW (r = 0.687 and r = 0.539, respectively; P < .05). The UCD strongly correlated with abdominal circumference (r = 0.648, P = .000) and estimated FW (r = 0.539, P =.000). The UCD increases with commonly used fetal parameters for sonographic estimation of GA (such as BPD, HC, and FL). The UCD related to GA and FW by these equations: UCD = 0.029 [GA] + 0.523; UCD = 0.135 [FW] + 1.101. The UCD of 50 patients was not included in the computation of the nomogram. This exclusion was due to 21 cases of IUFD, 10 cases of preeclampsia, 8 cases of oligohydramnios, and 11 cases of IUGR. Among these 50 cases of poor fetal outcome, the UCD was 2 standard deviations below the mean and correlated significantly (r = 0.712, P < .05) with adverse fetal outcomes (see Tables 1–3).
The Distribution of Patients’ UCD and GA.
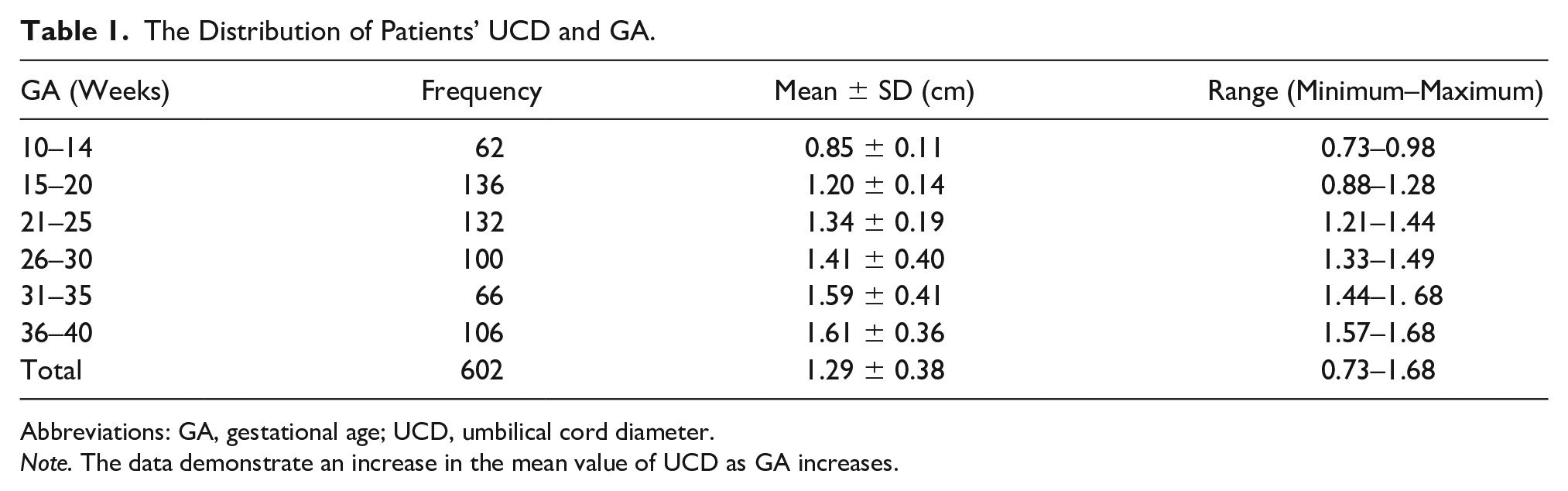
Abbreviations: GA, gestational age; UCD, umbilical cord diameter.
Note. The data demonstrate an increase in the mean value of UCD as GA increases.
The Distribution of Patients’ UCD and EFW.
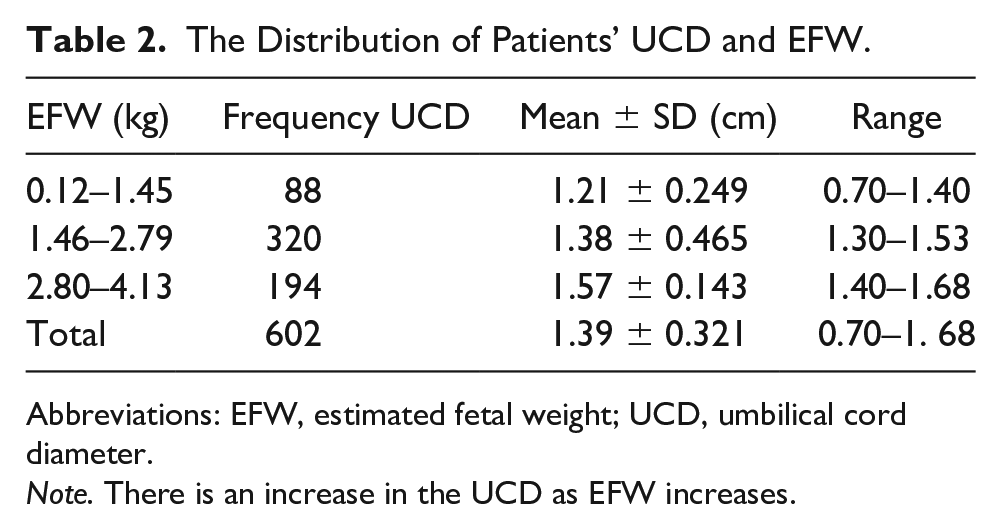
Abbreviations: EFW, estimated fetal weight; UCD, umbilical cord diameter.
Note. There is an increase in the UCD as EFW increases.
The Relationship of Patients’ Umbilical Cord Diameter Compared With Other Fetal Parameters.
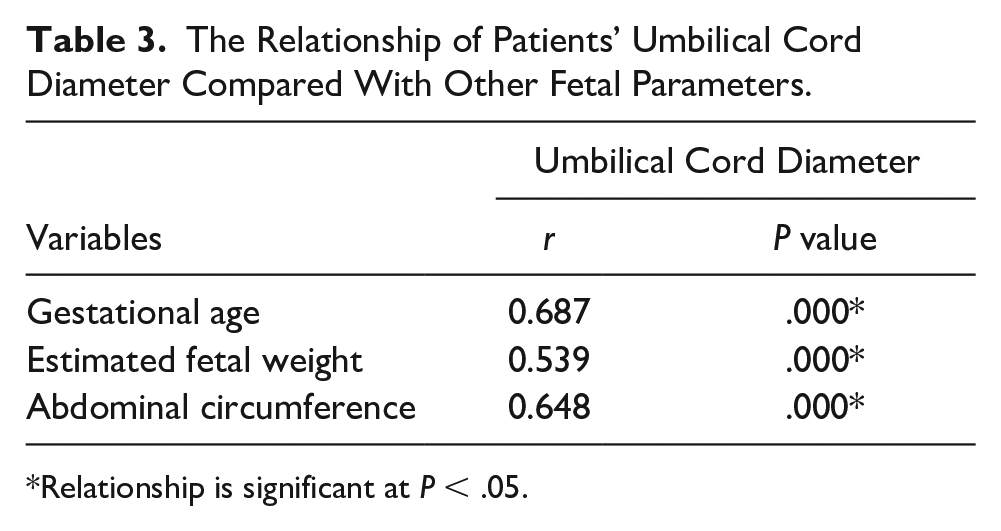
Relationship is significant at P < .05.
Discussion
Providing the best possible antenatal care and a successful maternal/fetal outcome depends largely on the accuracy of the determining GA. Sonography has remained an important imaging modality in estimating GA and in the assessment of fetal well-being. Estimates of UCD could help improve surveillance of the fetal growth trajectory and transform the care for a suspected complication in pregnancy.
In this study, the UCD ranged between 0.73 and 1.68 cm for GAs between 15 and 40 weeks and had a strong positive correlation with GA and EFW (r = 0.679 and r = 0.539, respectively; P < .05). Weissman et al 3 in their study on umbilical cord cross-sectional diameter, for varied GAs, observed that UCD increased progressively, with GA. Other studies6–8 also observed that the UCD increased steadily with GA.
The CRL had been shown to be accurate in dating a first trimester pregnancy. This measurement protocol is best made when the fetus is in a straight position. In cases where the fetus is not in a straight position, the UCD could provide an alternative means of dating the pregnancy in the first trimester. Results of this study also agree with those of Rostamzadeh et al 9 and Barbieri et al. 10 Both investigated UCD and its relationships with fetal biometric parameters and stated that UCD correlated positively with GA. Abdalla et al 11 conducted a similar study by estimating fetal age sonographically using UCD in the second and third trimester.
This study also established that UCD increases with commonly used sonographic metrics used to estimate GA and FW (such as BPD, HC, FL, and AC). Afroze et al, 12 in a separate study, reported a strong correlation between commonly used fetal measurements for GA and UCD. From these relationships, UCD continues to demonstrate a useful parameter for monitoring fetal growth.
The UCD of 50 subjects in this study was 2 standard deviations below in the first and second trimester. Observational studies of these 50 subjects resulted in 21 cases of IUFD, 10 cases of preeclampsia, 8 cases of oligohydramnios, and 11 cases of IUGR. Among these 50 cases, the UCD that was 2 standard deviations below the mean correlated significantly with adverse fetal outcomes. In fetuses with adverse outcome, UCD also correlated significantly with the severity of the outcome. Hill et al 13 reported a significantly shorter umbilical cord in the first trimester in cases of IUFD, in comparison with normal fetuses. Ghezzi et al, 14 in their study, noted that more than 40% of fetal demise cases which occurred within 15 weeks had, at the first trimester scan, an UCD that was 2 standard deviations below the mean. It is known that the amount of Wharton’s jelly in the first and early second trimester is low compared with the third trimester. It therefore signifies that the size of the umbilical cord early in gestation is primarily due to a progressive enlargement of umbilical cord vessels, which is required for sufficient blood supply to the growing fetus. Reduction in the UCD, at this early stage of pregnancy, might imply poor blood supply to the fetus. Earlier studies15,16 have reported that the resistance to blood flow decreases constantly from the 8th to 14th week of gestation. This phenomenon may in one part be explained by the progressive disintegration of the spiral arteries because of trophoblastic invasion and in another part by the increasing diameter of the umbilical vessels. 14 Another study 17 reported an increased umbilical artery resistance to blood flow in patients who developed a pregnancy-related hypertensive disorder compared with patients with a normal pregnancy course. From our observational studies, the mothers of ten of the fetuses whose UCD was at least 2 standard deviations below the mean had preeclampsia, while 25 cases of the fetuses whose UCD was at least 2 standard deviations below the mean for that GA resulted in IUFD. Resistance to blood flow within the umbilical cord, therefore, appears to stem from poorly developed umbilical vessels, which consequently results in small UCD. In addition to the aforementioned research, other studies have demonstrated the reciprocal relationship between umbilical vessels and the composition of Wharton’s jelly, in the second half of gestation, and its influence on maternal/fetal outcomes.18–21 Bruch et al, 22 using a computerized microscope, demonstrated that umbilical vessels and Wharton’s jelly ultrastructure in IUGR fetuses were significantly different compared with normal fetuses. Again, earlier studies had revealed that neonates, with Down syndrome, had shorter umbilical cords than their normal counterparts. 23 From these observations, umbilical cord morphometry could be useful in identifying a risk of IUFD.
One of the major functions of Wharton’s jelly is to facilitate fetal-amniotic fluid exchange of water and electrolytes, freely moving between compartments. 24 Scanning electron microscopy studies have revealed that precipitation of collagen type IV, laminin, and heparan sulfate was observed in the first trimester around canalicular-like structures in Wharton’s jelly. 25 These findings may document exchanges that occur between umbilical vessels and amniotic fluid. 25 The interaction between these canalicular-like structures, the surrounding mesh of collagen fibrils and myofibroblasts, normally present in Wharton’s jelly, appears responsible for regulating the turgor and elasticity of the umbilical cord. 26 Since the risk of cord compression or torsion is irrelevant or unlikely early in pregnancy, other features, such as the capability to exchange substances from and to the amniotic fluid, are more important in a rapidly growing fetus. Disruption of this function adversely affects the growth of the fetus. The size of the umbilical cord is an important marker of the integrity and functionality of ultrastructure for the umbilical cord. It may also be a reflection of its capability to perform the essential support for a swiftly developing fetus.
Conclusion
The UCD could serve as an important indicator of fetal growth, well-being, and perinatal outcome. Abnormal umbilical cord size might be an important marker for the identification of patients at risk of IUFD and poor maternal/fetal outcomes. There is a need for a replication and larger study of umbilical cord morphometry. This type of study would be useful in confirming a method of identifying a group of patients at risk of IUFD or an adverse fetal outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.