
Abstract
Objective:
Children with critical congenital heart disease (CHD) often present in remote areas with life-threatening illness. Although performing complete pediatric echocardiograms requires significant training, remote locations necessitate sonographers with limited pediatric experience screen for CHD. The Sonographer University (SU) was designed to improve comfort in adult sonographers scanning children and recognizing CHD.
Methods:
The SU consisted of lectures, multimedia case studies, roundtable discussions, pathology stations, and hands-on scanning of 20 volunteer pediatric patients with either normal or diseased hearts. Topics included an overview of critical congenital heart lesions, crucial views for each defect, and pitfalls in imaging children.
Results:
Forty-four participants completed the SU seminar. In pretest assessment, approximately two-thirds said they were currently required to scan children. Participants’ comfort level sonographically scanning children and recognizing CHD improved substantially. A posttest showed that the course improved participants’ skill, knowledge, and confidence with pediatric studies.
Conclusion:
The SU seminar helped sonographers from remote areas to develop improved recognition of CHD, confidence in pediatric scanning, and methods for obtaining assistance with imaging a critically ill child.
Keywords
Congenital heart disease (CHD) affects approximately 1% of the 1.2 million people (under 21 years of age) living in Oregon and southwest Washington state. Many neonates, children, and adolescents are at risk of presenting with undiagnosed cardiac lesions and in dire circumstances to their local hospitals. Sonographers with limited pediatric experience are expected to perform echocardiograms in an effort to identify these problems. In this situation, sonographers commonly feel that they need more training to rapidly recognize findings specific to children with CHD who are deteriorating. In a high-stress environment, they may perform incomplete echocardiographic views, may not optimize equipment settings for children, may have difficulty calming the patient and family, or may lack recognition of a life-threatening disease. 1 Consequently, delays in initiating treatment or transfer of care can contribute to poor pediatric outcomes, such as acidosis, shock, and death. The Sonographer University (SU) seminar was envisioned and designed to instruct rural sonographers with adult patient diagnostic experience. The intent was to assist them to recognize specific CHD conditions in children that they may encounter in their local hospital.
Methods
Course Design
The SU seminar was held in May 2018 at an Oregon regional center for congenital heart care. The program was supported by a hospital-funded educational grant. Advertising through print and digital media was distributed to hospitals and local echocardiographic societies across the Pacific Northwest and the territory of American Samoa. These rural areas had direct ties to the hospital’s cardiac outreach program. Sonographers were not charged a registration fee, and scholarships were offered to cover housing and/or travel. The SU seminar occurred over the span of two consecutive days.
The first day consisted of a series of lectures given by physicians, surgeons, and pediatric-trained sonographers. Learners reviewed the anatomy and physiology of nine critical congenital heart lesions, including the signs and symptoms children with those lesions exhibit when they present for care. Crucial echocardiographic views for each defect were defined and demonstrated. The lesions consisted of coarctation of the aorta, D-transposition of the great arteries, total anomalous pulmonary venous return, hypoplastic left heart syndrome and other single ventricles, coronary artery anomalies, critical aortic and pulmonary valve stenosis, pericardial effusion, and overall depressed ventricular systolic dysfunction. The SU seminar also reviewed appropriate transducer selection and imaging optimization. A video demonstrating establishment of rapport, techniques to engage caretakers, methods of creating a comfortable atmosphere for children, ideal patient positioning, and probe placement were reviewed. An accompanying lecture addressed the common pitfalls associated with imaging children of varied ages. Other lectures included a current review of congenital heart disease (incidence and detection), relationship between detection and outcomes, accuracy of pediatric studies performed in adult cardiac laboratories, sources of error, and perspectives on imaging from a surgeon and a pediatric cardiac interventionalist. Furthermore, options on how to acutely obtain assistance with the care of pediatric patients was emphasized. In addition to lectures, the first day also included multimedia simulated cases and a roundtable discussion with sonographers sharing personal pediatric experiences acquired over 30 years of sonographically scanning children. Guided by cardiologists, the SU learners were immersed in an interactive learning station on the topic of cardiac pathology. This provided participants the chance to inspect both normal hearts and examples of the critical lesions that correlated with prior lectures. Learners were given universal serial bus (USB) drives loaded with lecture slides and simulated cases for further review.
The second day consisted of guided echocardiographic scanning of 20 volunteer pediatric patients (7 months to 16 years) presenting with normal hearts or cardiac disease. Ten hands-on sonographic scanning stations were set up in multiple locations around the host hospital. Cardiac sonographers with pediatric experience supervised each station, and learners were allowed to progress at their own pace. Volunteers with normal hearts were scanned during the first half of the day. Specific topics explored during the scanning session, aside from normal cardiac anatomy, included: coronary optimization, atrial septal/ventricular septal sweeps, use of the right sternal border and subcostal windows, pulmonary vein enhancement, and “age challenges.” The age-challenge scanning stations were focused on how to obtain an echocardiogram in a disengaged teenager, a talkative kindergartener, and a wiggly toddler. The second half of the day was spent evaluating pediatric volunteers with CHD, including single ventricles at all stages of palliative surgery, bicuspid aortic valve, repaired transposition of the great arteries, and repaired Ebstein’s anomaly. Sonographers with pediatric experience guided learners through pertinent views for each lesion with advice on image enhancement. Additionally, two diagnostic interpretation sessions were set up with pediatric cardiologists reviewing deidentified echocardiograms. They demonstrated both optimized and challenging versions of the critical lesions presented on the first day. The physicians stressed the importance of specific views for different diseases, techniques for enhancing visualization of challenging structures, and how missing information negatively affects an echocardiographic interpretation.
Course Assessment
Prior to the course, learners were given an online survey to evaluate the frequency and comfort level with scanning children as well as comfort recognizing CHD. Additionally, a 15-question online test assessing knowledge of specific congenital lesions, using echocardiographic images and videos, was performed. Question content evaluated topics including accurate identification of anatomy, recognition of acuity of disease, determination of appropriate next steps, and comprehension of ultrasound physics (see Figure 1). Upon completing the seminar, learners took a posttest and survey to gauge course effectiveness. The surveys were anonymized and collected with an online survey tool. Pre- and postsurvey results were compared using Wilcoxon signed-rank analysis.
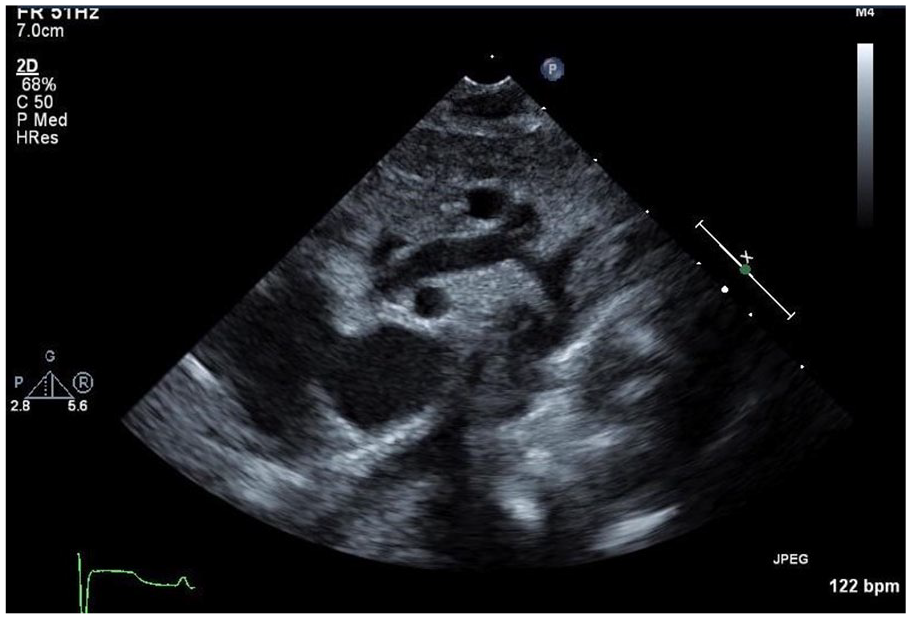
Sample image from pre- and postassessment test. Question: How concerned are you about the above abnormality? Answer choices included: (A) Not concerned at all—Complete the study and follow your regular procedures for notifying providers/readers; (B) Mildly concerned—Complete the study but make sure to notify the providers/readers that the study may be abnormal; (C) Concerned—Obtain focused additional imaging and notify providers/readers; and (D) Very concerned—Stop the study now and immediately notify providers.
Results
Forty-four learners attended the SU seminar from the Pacific Northwest region of the United States and the island of American Samoa. Of those, 42 were adult-trained sonographers with varied experience conducting sonography of pediatric patients. Additionally, there was one pediatrician and a vascular sonographer who attended this course. There were 39 learners who completed the precourse survey, and 65.7% responded that they sonographically scanned children occasionally or frequently. Prior to the SU seminar, 23.5% of learners were not at all comfortable providing sonography for children (see Figure 2), 35.3% were not at all comfortable recognizing CHD (see Figure 3), and 29.4% did not have a pediatric sonographic imaging protocol. Nineteen participants completed a postsurvey, which showed that 5.9% remained not at all comfortable scanning children, 17.6% were not at all comfortable recognizing CHD, and 5.9% still did not have a pediatric sonographic imaging protocol. Comparison of scores from pre- and posttests demonstrated no statistically significant difference in the learners’ average scores, 54.6% (95% CI, 14.3%-78.6%) to 58.8% (CI, 35.7%-85.7%).
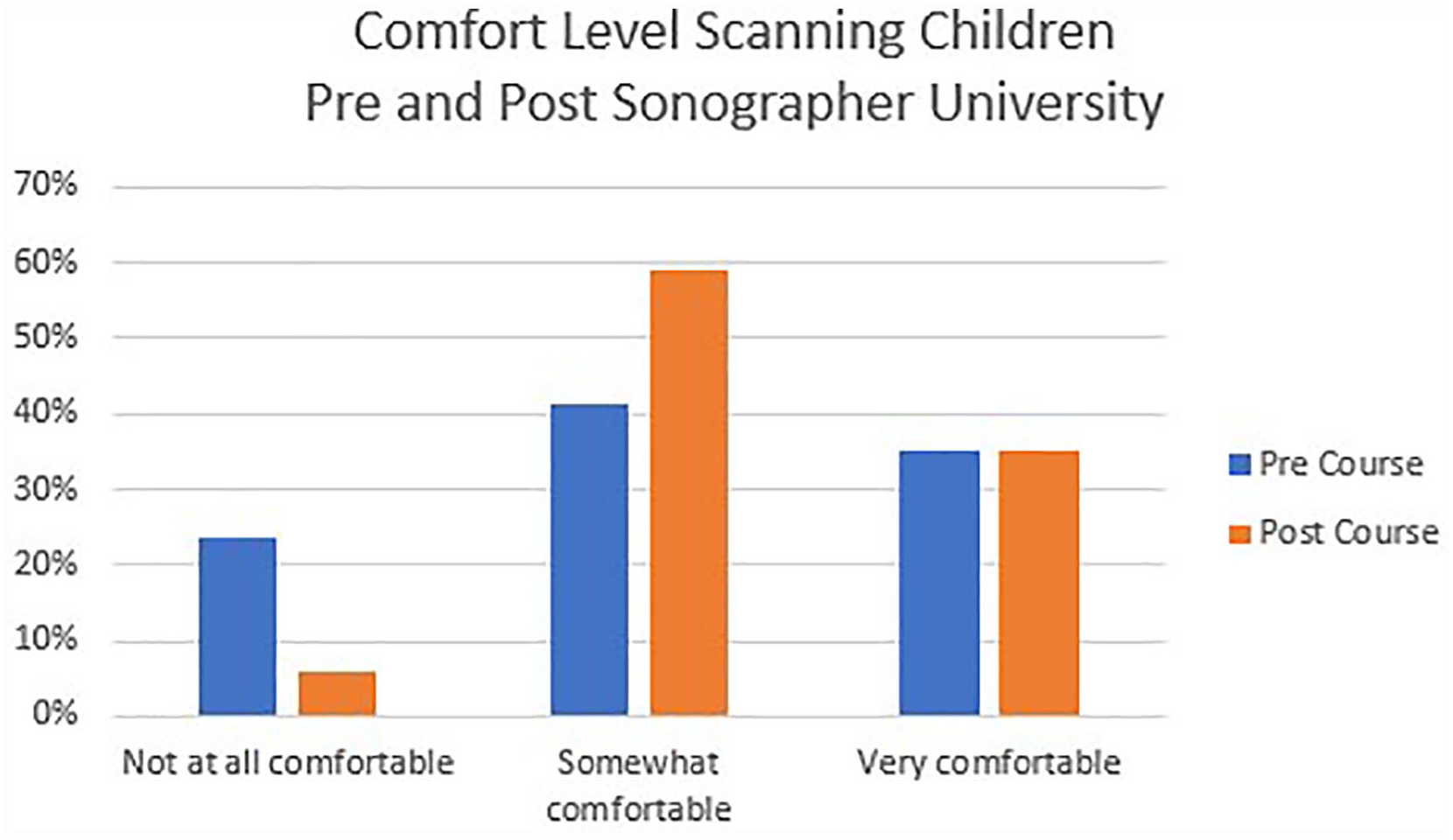
Adult-sonographer comfort level scanning children before and after the Sonographer University.
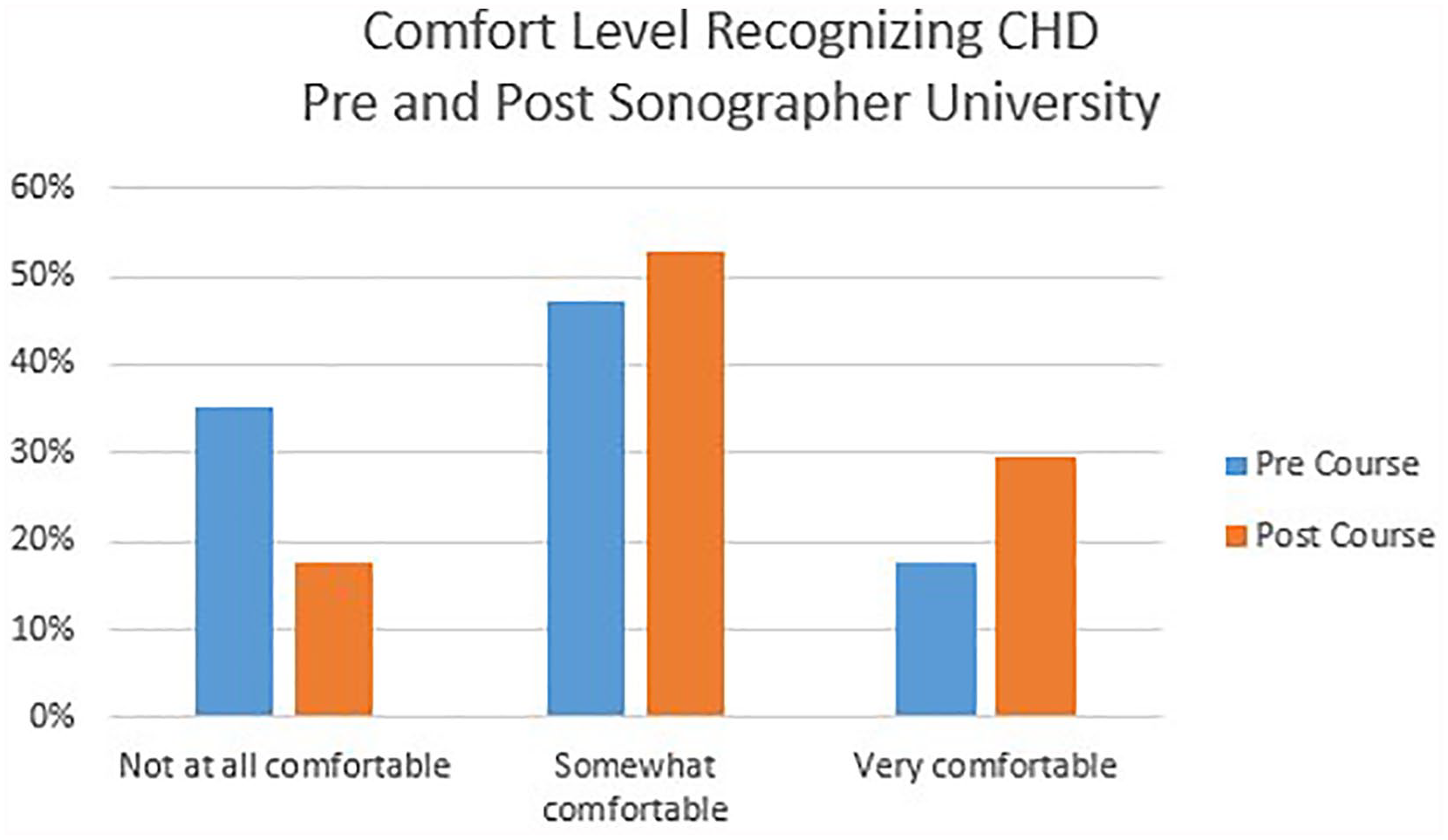
Adult-sonographer comfort level recognizing congenital heart disease before and after the Sonographer University.
The quality of the entire SU seminar and each individual lecture was assessed with a 5-point Likert scale, with rating choices from poor to excellent. Qualitative evaluations of the seminar were overall excellent, and 89% of learners stated they would repeat it. The group qualitatively felt the seminar had improved their skills, knowledge, and confidence with providing sonographic scanning of children. The hands-on scanning component of the seminar was the highest rated portion of the training. Additional qualitative assessment included the following comments: The presentations were clear and helpful. Each topic was addressed towards adult sonographers approaching pediatric echoes. It was great having hands on scanning. The roundtable discussion was awesome. I would love to do this again. Unfortunately, my employer is resistant to support staff with educational opportunities such as this. Without free tuition there is no way I could have attended. Sonographers helped a ton while scanning. I appreciate the wide variety of topics and pathology discussed.
In response to the question, What would you suggest for a future course?, learners responded: Make hands on scanning time longer. More case studies. A booklet to take home to the adult echo lab with echo pictures and illustrations.
To provide added context, a few selected profiles are provided of some of the SU learners:
Learner 1: A recent graduate from an echocardiography program, with one year of work experience. Learner 1 reported never providing pediatric sonography, not feeling comfortable scanning children, or recognizing critical CHD.
Learner 2: A sonographer that worked at a large urban hospital in an echocardiography laboratory and mostly scanned adult patients as well as some inpatient neonates and outpatient children. Learner 2 reported frequently providing pediatric sonography and felt very comfortable both scanning and recognizing CHD.
Learner 3: A vascular sonographer with nearly 20 years of experience in general and vascular sonography labs. Learner 3 reported never scanning children and did not at all feel comfortable recognizing CHD.
Discussion
Pediatric-trained sonographers are rare and often not available for hire in local hospitals, situated in remote regions. For adult-trained sonographers, additional training on how to adequately and completely perform neonatal and pediatric echocardiograms on patients with CHD requires mentorship, time, and practice. Even if a sonographer were trained in pediatric imaging, the frequency with which these skills are utilized in a remote setting may be minimal and over time these skills could be lost. However, in most settings, a pediatric patient may need a sonographic evaluation. In that moment, it is paramount that the sonographer is equipped with a straightforward, fast, and focused approach to evaluate potential CHD. This need was supported by the fact that nearly two-thirds of the sonographers were required to scan children either occasionally or frequently.
Although improving pediatric skills in adult-trained sonographers is imperative, this does not replace a complete pediatric echocardiogram performed for CHD in an Intersocietal Accreditation Commission (IAC) accredited echocardiographic laboratory. Instead, a large amount of the SU’s didactics were focused on the limitations of an incomplete pediatric study. It also pointed out the limited conclusions that can be made for children under different physiologic conditions. Furthermore, this seminar stressed the absolute need for a complete pediatric echocardiogram and pediatric cardiology evaluation to accompany any limited study performed. Participants were introduced to several direct ways to communicate with on-call pediatric sonographers and pediatric cardiologists for future questions. They were also given contact business cards for these professionals to provide an immediate reference.
The continued advancement of imaging technology, including rapid assessment tools such as point-of-care ultrasound, has led to increased desire and expectations for these imaging studies. The technology to quickly evaluate CHD is rapidly outpacing the training available.2,3 Limited courses and seminars, similar to the SU, have been used for training novice practitioners. In one study, first-year pediatric cardiology fellows completed a 3-day pediatric echocardiography course with a mixture of lectures and hands-on scanning sessions. 4 Fellows that participated in the course performed more independent pediatric echocardiograms over the following 3 months than the control group. Additionally, those fellows reported significantly higher self-efficacy scores after completion of the course. It was concluded from that study that perception of self-confidence contributed to a cardiology fellow’s willingness to perform additional echocardiograms.
Although courses can be geared toward beginners, the SU seminar was focused on learners that possessed the physical skills to perform an echocardiogram but lacked experience in pediatrics. Programs like the SU devoted to obstetrics have been effective in training sonographers to perform specific views and increase the detection of fetal cardiac anomalies. The most notable studies have shown that multiple-year training programs are most effective at increasing detection rates of prenatal CHD.5,6 However, not all institutions are able to offer such extensive programs, and the geographical distance of sonographers to training facilities may be a hindrance. A study from Northern Ireland tested a limited 2.5-day course for prenatal detection of CHD. 7 Training included lectures and hands-on sonographic scanning of the four-chamber view and outflow tracts of the heart. With even that limited course, the detection rate of major CHD was increased from 28% to 43%.
Quantitatively, learners at the SU seminar did not demonstrate a significant improvement in their standardized test scores due to several reasons. One cause may have been that the SU seminar was structured for quality improvement in regional sonographers and was statistically underpowered to demonstrate a significant difference. Next, test questions were written before the lectures were composed and did not connect, in parallel, with content stressed by the speakers. Additionally, the percentage of learners that completed the posttest assessment was less than half of those who took the presurvey. Finally, scores may have been affected by the significant variation in basic training of the learners. Although this course assumed some basic prior experience, a vascular sonographer would not have been expected to score higher on the posttest compared to a learner with some pediatric sonographic experience.
Immediate qualitative assessments showed improvement in self-reported sonographer skills, knowledge of CHD, and comfort with children. The overall perception of the course was that it was successful in improving individual skills. Self-efficacy has been linked to performance outcomes and willingness to perform a difficult task. 8 To perform well, a base of knowledge and skills is necessary; however, the perception of one’s ability to perform is an important factor in achieving success. 9 In this case, the SU seminar learners anecdotally reported that they were more willing to perform pediatric echocardiograms and with greater confidence. One limitation of the seminar was that there was not a posttest given 6 to 12 months afterward to evaluate longitudinal learning.
Larger academic institutions are well suited to training learners and have an obligation to adequately prepare them in recognizing life-threatening pediatric cardiac disease. The SU seminar demonstrated that creating and implementing a limited pediatric course for those who could already perform an echocardiogram is feasible and relatively easy. The fact that the hands-on portion of the seminar was highly ranked speaks to the need for physical engagement in the learning process, particularly in this skills-based profession. More quantitative assessment of learners both immediately after the sessions as well as at 6-month and 1-year intervals would provide the true impact of this type of educational seminar.
Implications for practice
In a clinical landscape situated in a diffusely populated area like Oregon and Washington, not all studies can be performed in a pediatric IAC-accredited laboratory. This makes it imperative that sonographers performing adult studies become comfortable with performing urgent pediatric sonographic studies. This extends to becoming knowledgeable about congenital cardiac lesions and the proper approach for pediatric patients. Tertiary care pediatric echocardiography laboratories are equipped to provide supplemental pediatric training, and this seminar demonstrated the feasibility and desirability within this regional area. Utilizing a format like this SU seminar, sonographers were able to improve their comfort in recognizing critical congenital heart disease. They also improved their overall confidence in performing a pediatric echocardiogram as well as their knowledge about seeking help when evaluating a child with CHD. Additionally, this educational approach led to deeper connections with adult sonographers and the academic center, facilitating future communication in caring for these patients.
Future recommendations
Further studies quantifying long-term results of seminars, like SU, are needed and should assess the interval for repeated education. Additionally, this type of educational seminar needs further development and adjustment to meet specific learner’s needs (i.e., providers in emergency rooms, neonatal, and pediatric intensive care units). Finally, this case series demonstrated the importance of providing significant sonographic scanning time, numerous case studies, and portable echocardiographic example images of CHD for learners. These activities will provide future learners the potential to improve their clinical education and ultimate performance of their pediatric echocardiography skills.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Friends of Doernbecher Foundation Grant.