
Abstract
Human chorionic gonadotropin is generally used as a biomarker to identify invasive molar pregnancy. The extent of the disease (e.g., its staging) has not, however, relied on its sonographic description. A case is presented that can illustrate some diagnostically useful sonographic features of three-dimensional transvaginal sonography for this condition. The clinical imaging of this case initially suggested it to be a benign hydatidiform mole but ultimately was diagnosed as an invasive molar pregnancy, with human chorionic gonadotropin monitoring. Clinical imaging was used to help manage this patient, with the demonstration of trophoblastic invasion of the uterine wall. Although two-dimensional sonography is commonly used to diagnose molar pregnancy, three-dimensional sonography may offer a clinical advantage for the management of invasive molar pregnancy, which can occur in 15% of benign hydatidiform molar pregnancies.
Keywords
Gestational trophoblastic neoplasia (GTN) has been categorized into complete molar pregnancy (CMP), invasive molar pregnancy (IMP), and choriocarcinoma (CHC) for appropriate management.1,2 CMP, a benign anomalous product of gestation, represents a condition occurring in about 1 in 500 to 1000 pregnancies. IMP occurs in 15% of those cases, and CHC occurs in 5% of those case, which demonstrates the occurrence of these clinical entities. 3 Human chorionic gonadotropin (hCG) has been the primary biomarker used to make the diagnosis of IMP. Advances in high-resolution two-dimensional transvaginal sonography (2DTVS) and three-dimensional transvaginal sonography (3DTVS) enable visualization of the extent of actual trophoblastic invasion into the uterine wall. 4 The current standard of patient care dictates that hCG be drawn for diagnostic follow-up after a CMP diagnosis is histologically made in order to identify its natural decline. If the hCG levels plateau or rise, however, the presence of an IMP is indicated. A recent case is described that illustrates the management of this disease entity with the use of 3DTVS.
Case Report
A 32-year-old G3P1011 at approximately 6 weeks gestation presented to an outpatient clinic for confirmation of pregnancy. At the time, she declined a quantitative beta hCG or transvaginal sonogram. The patient was again seen at 8 weeks gestation and had a quantitative beta hCG of 116 309 mIU/ml, drawn at that time. A 2DTVS and 3DTVS revealed markedly thickened and heterogeneous endometrium with multiple irregular cystic spaces, compatible with CMP. She underwent suction dilation and curettage, with the final pathology examination resulting as immature hydropic chorionic villi with features most consistent with complete hydatidiform mole (CMP). She was seen for a follow-up visit when she complained of heavy vaginal bleeding, similar to her menstrual flow, so she then underwent 3DTVS. The sonography results were significant for suspected IMP. Analysis of the images revealed that there was penetration of the molar pregnancy on the posterior uterine wall with the distance between the IMP. The posterior uterine serosa was noted to be 1.8 mm (see Figure 1), and the histogram demonstrated a vascularity index of 13.3% (see Figure 2). The patient was then recommended to meet with a physician on the gynecologic oncology service. On postoperative day 23, the patient presented to the local emergency department with a complaint of heavy vaginal bleeding associated with passage of clots. The patient’s quantitative beta hCG was found to be 49 497 mIU/ml, which was increased since her uterine evacuation. She underwent a second uterine evacuation, and a computed tomogram (CT) of the chest and abdomen/pelvis was deemed negative for metastatic disease. These diagnostic results helped to establish the patient to be at stage I gestational trophoblastic disease (GTD), considered to be low risk. Surgical pathology from the second dilation and curettage revealed retained products of molar pregnancy with blood clot and decidua. Subsequently, the patient was started on sequential methotrexate therapy, which resulted in a continued decrease in quantitative beta hCG.
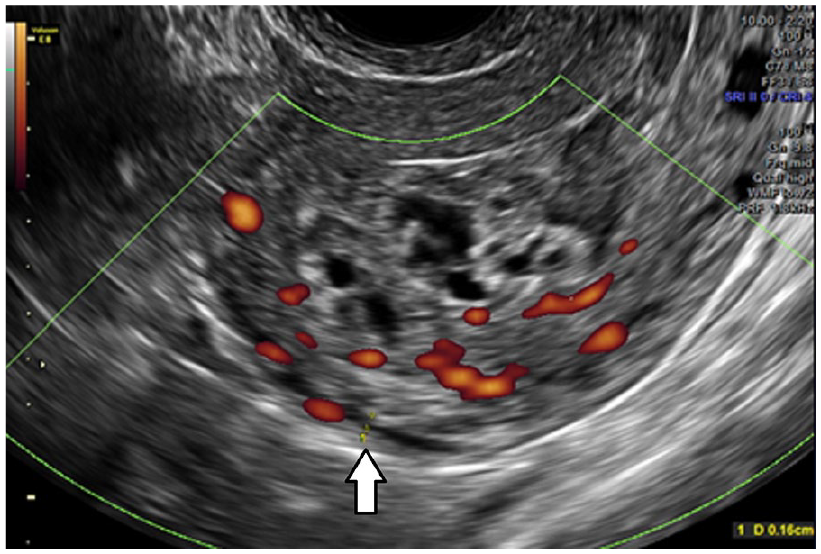
Sagittal view of uterus with transvaginal sonography and power Doppler angiography demonstrating increased vascularity, trophoblast proliferation. There was deep myometrial invasion up to 1.8 mm from the posterior uterine serosa, indicating the presence of an invasive molar pregnancy. Arrow shows distance between invasive molar pregnancy and uterine serosa.
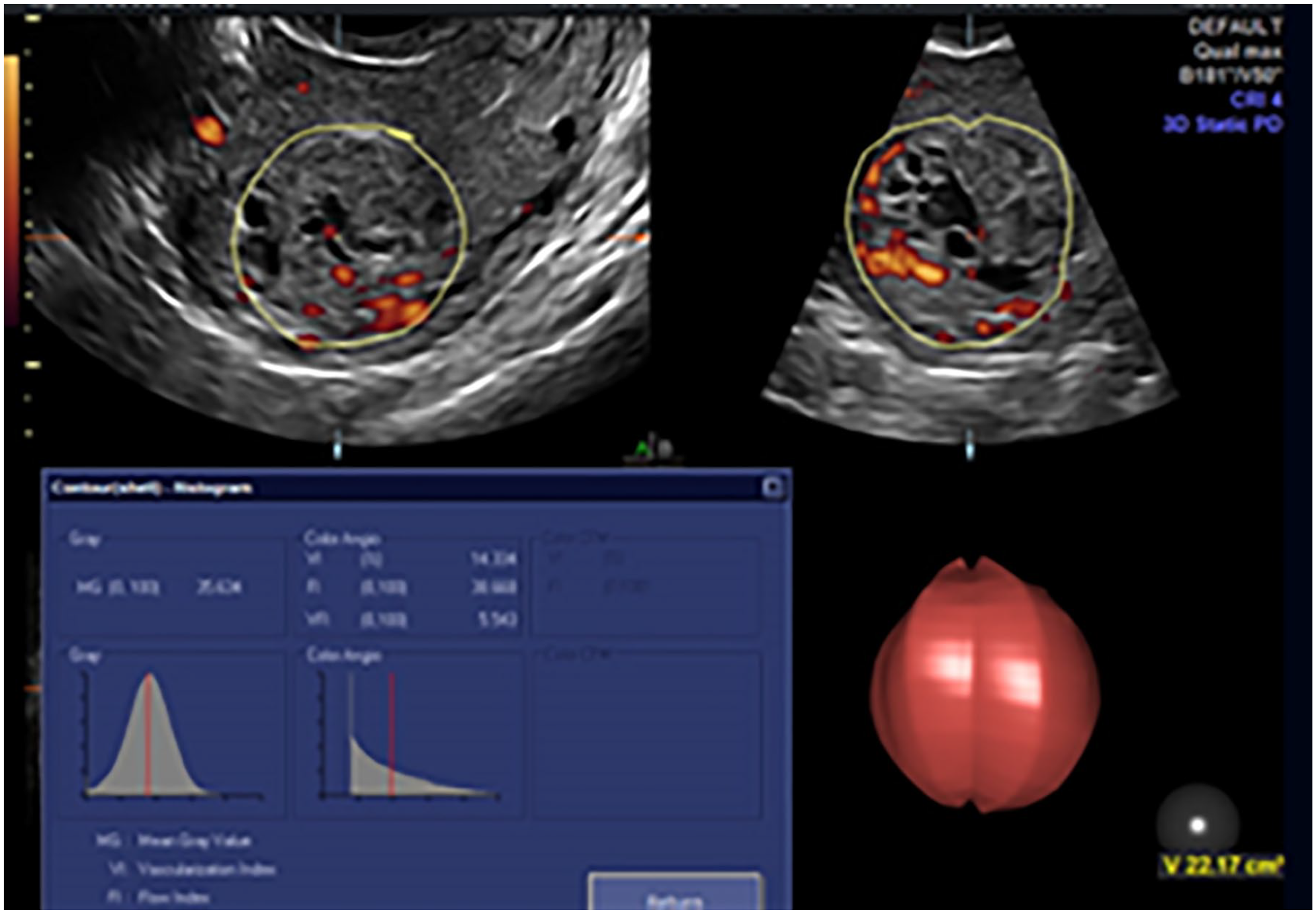
Three-dimensional transvaginal sonography histogram of the invasive molar pregnancy (IMP). It demonstrates a vascularity index of 13.3% (a percentage of voxels that reveal the presence of vascularity, within the acquired volume), consistent with the trophoblastic tissue invasion of the uterine wall, as expected with IMP.
Discussion
Whereas the diagnosis of IMP has relied on rising or plateauing hCG levels, after uterine evacuation of a benign molar pregnancy, 2DTVS and 3DTVS can document the extent of uterine invasion. 5 A complete molar pregnancy is associated with marked cystic changes and mass formation and is diagnosed sonographically, often with 2D sonography. A partial molar pregnancy presents with minor cystic changes of the placenta and remains often underdiagnosed sonographically. 6
There have been several published reports on the use of 3D sonographic features to diagnosis a molar pregnancy in the first trimester.7 –9 A uterine invasion was recently demonstrated with a cesarean scar pregnancy, which is an unusual type of ectopic pregnancy. 10 Such imaging may aid clinical decision-making with regard to whether more extensive medical treatment is appropriate or surgical intervention is indicated (e.g., hysterectomy). Current discussions related to scoring of GTD have not included any contribution to the sonographic diagnosis but rather, its histologic and hCG biomarker features. 3 Therefore, the question as to whether imaging (e.g., 2DTVS and 3DTVS) can consistently predict GTN invasion prior to hCG monitoring remains to be seen. However, the role of sonography may provide optimal management of this disorder and become more important as a diagnostic and treatment tool, supplementing traditional laboratory technologies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.