
Abstract
Background:
The present study aimed at evaluating the diagnostic value of lung transthoracic ultrasonography (TTUS) and lower extremity sonography versus computed tomography pulmonary angiography (CTPA) in the diagnosis of pulmonary embolus (PE).
Materials and Methods:
This study was performed on 104 patients with clinically suspected PE. CTPA and D-dimer was performed on all patients. Wells’ deep vein thrombosis criteria (WDVTC) was evaluated and recorded at the patient’s admission. Finally, the results of adding venous and lung sonography scores to the WDVTC with and without the results of D-dimer test were analyzed for predicting the diagnosis of PE.
Results:
There were 104 patients clinically suspected of having a PE and enrolled in the study. A PE was confirmed in 37.5% of this cohort. WDVTC had a sensitivity and specificity of 94.87% and 80.00%, respectively, to predict PE. When adding D-dimer to the WDVTC for patients unlikely to have a PE (WDVTC≤4), the sensitivity and specificity of positive D-dimer in diagnosis of PE were 94.87% and 56.92%, respectively (P < .001).
Conclusion:
According to these study results, the modification of the WDVTC along with the results of lung TTUS and lower extremity venous sonogram significantly increase the diagnostic power for PE.
The patient’s incidence rate of pulmonary embolism (PE) is 69/100 000 per year and a mortality rate of 9/100 000. 1 Symptoms of PE are typically nonspecific, and clinical signs and symptoms may be masked by coexisting conditions. 2 Therefore, the diagnosis of PE has always been a challenge for specialists and requires a variety of invasive and noninvasive diagnostic techniques as well as a strong clinical suspicion. 3
The standard diagnostic test for patients with suspected PE is computed tomography angiography (CTA); however, a number of conditions such as practicing in low-resource settings or dealing with patients with renal failure or morbid obesity have limited its application. Radiologic contrast media sensitivity and nephropathy are also considered as serious side effects. 4
The D-dimer test is a useful nonspecific biomarker with high negative predictive value in ruling out fewer probable cases. 5 Therefore, according to international medical guidelines, it is recommended to use D-dimer in low probable clinical settings in conjunction with probability scores like the Wells score (Ws). 6 In addition, PE can be found in about 50% of cases with deep vein thrombosis (DVT) and is usually asymptomatic, therefore increasing data support using bedside ultrasonography (US) as a noninvasive diagnostic tool.7–9
In fact, bedside US is a rapid, safe, and potent diagnostic tool that can help physicians to evaluate their critical cases in a more accurate and timely manner. 7 Furthermore, it can be used at any time and place for patients regardless of the variables of age, pregnancy, kidney failure, or contrast allergy.3,10
Transthoracic ultrasonography (TTUS) is a new diagnostic modality for evaluating diffuse or localized pulmonary diseases, especially in pediatric or emergency departments.11–13
Given the advantages of using US and TTUS, researchers have aimed at combining the findings of these technologies with the Ws scores to improve the accuracy of the Wells’ diagnostic criteria. 14 This study evaluated the diagnostic value of adding TTUS and lower limb sonography findings to the Wells’ criteria. The combined scoring was compared with the results of the pulmonary CT angiography (CTPA) in clinically suspected PE cases referred from two hospitals.
Materials and Methods
Patients and inclusion criteria
This was a cross-sectional study of all clinically suspected PE patients referred from two hospitals during 2017–2018. Based on previously conducted studies 13 as well as the 82.4% sensitivity of TTUS compared to CTPA for detecting PE, a power analysis of 80%, with a 95% confidence level, an error of 0.1%, and a probability ratio of 0.5% was set. Conveniently, 112 cases were selected as the sample using a nonprobability sampling method.
The study inclusion criterion was based on the clinical suspicion of PE according to clinical signs and symptoms and the Ws criteria. The exclusion criteria were a history of pulmonary parenchymal lesions, previous lung surgery, obesity (>120 kg), and those unstable patients unable to be transfer from the emergency department to CT.
Considering the aforementioned criteria, five patients were excluded from the study due to hemodynamically unstable conditions, and three were excluded due to previous lung lesions (2/3 had metastatic lung cancer, and one had an occupational lung injury). Therefore, based on study criteria, 104 patients were invited and provided written consent for the research study.
Study Design
Initially, all of the 104 patients were screened to obtain their Ws criteria, vital signs, admitted symptoms, and D-dimer levels and were recorded.
At the same time, bedside TTUS (to evaluate lung and heart) and three-points lower extremity venous compression US were completed.
CTPA was performed for all patients to confirm or rule out the diagnosis of PE. A single radiologist that was blind to the cases and to the study provided a report on CTPA imaging study.
D-dimer analysis
The D-dimer levels were checked, and values higher than 500 μg/L were considered to be a positive result. 15
Sonography
A gray-scale, three-point compression US was completed to detect a possible lower extremity DVT. This was completed with a linear probe (10 MgHz; SHENZHEN Mindray Bio-Medical electronics Co., LTD, China). Both lower limbs were evaluated at femoral, saphenofemoral junction, and popliteal vein to document the presence or absence of venous compression. 16
Bedside TTUS was completed across both lungs to evaluate for pleural effusion and lesions with a curvilinear transducer (6 MgHz; SHENZHEN Mindray Bio-Medical electronics Co., LTD, China). This was done by adjusting the depth of the image to approximately 2 to 3 cm. The following criteria were used to interpret ultrasonographic findings: (1) PE was highly considered when two or more characteristic triangular or rounded pleura-based lesions were demonstrated, (2) PE was considered moderately probable when there was one typical lesion with slight adjacent pleural effusion, (3) PE was considered nonspecific when there was a subpleural lesion less than 5 mm in size or there was just slight pleural effusion, and (4) PE was not established when there was a normal chest sonogram 16 (Figure 1).
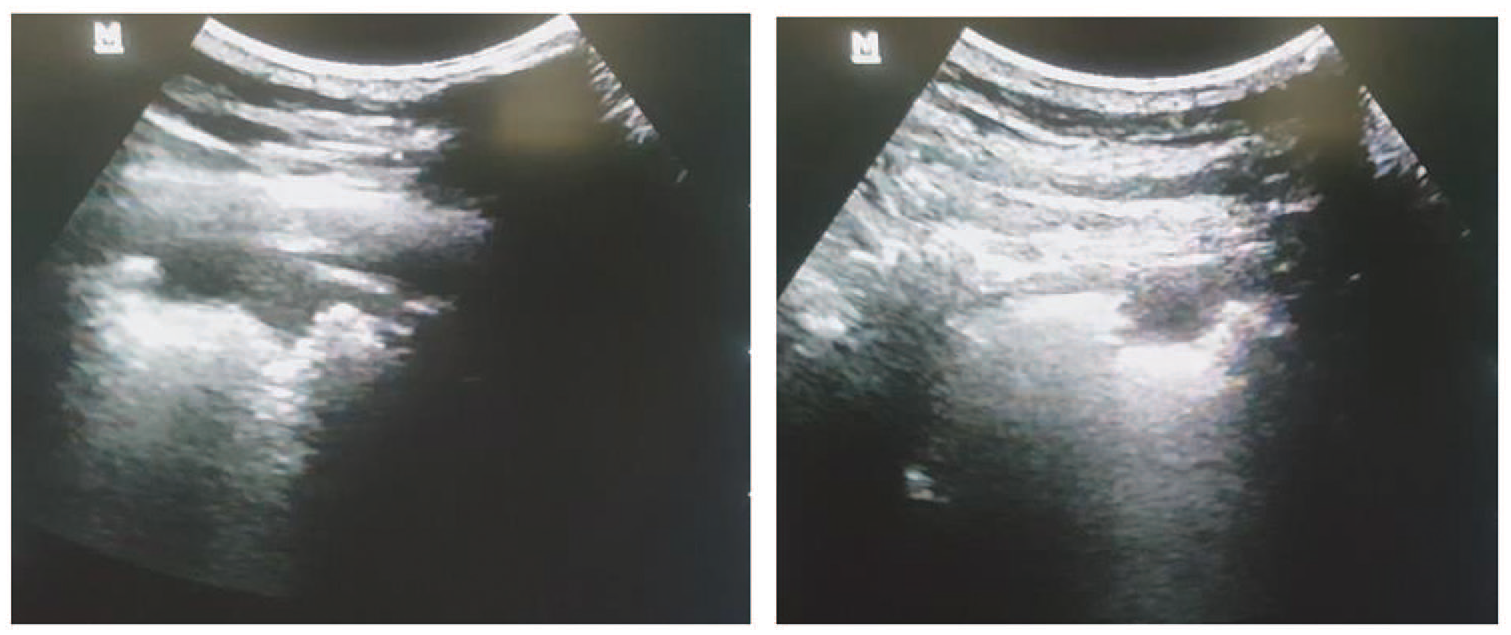
A subtle, pleural-based, hypodense parenchymal defect representing an area affected by pulmonary embolism is shown on transthoracic ultrasonography. The transducer is placed at the right posterior axillary line in a coronal plane.
Bedside echocardiography was used to evaluate the ratio of right ventricle size to left ventricle in long axis view (left 4th-5th intercostal space) or the presence of McConnell's sign in a four-chamber view. This was completed with a phased array transducer (3.2 MgHz; SHENZHEN Mindray Bio-Medical electronics Co., LTD, China).
US examinations were performed by an emergency medicine physician that participated and passed successfully a 7-day hands-on workshop (6 hours daily) based on cardiac, lung, and duplex venous compression. The 7-day workshop was a mix of theoretical and practical sessions.
Modified ultrasonography based on Wells' deep vein thrombosis criteria
The new Wells' deep vein thrombosis criteria (WDVTC) was defined by modifying the Wells’ criteria by replacing “signs and symptoms of DVT” with “venous ultrasound positive findings for DVT.” The :alternative diagnosis less likely than PE” was replaced with a diagnosis less likely for PE by lung and heart TTUS (Table 1).
Items of the Wells’ Score (Ws) and Modified Wells’ Criteria (USWs).
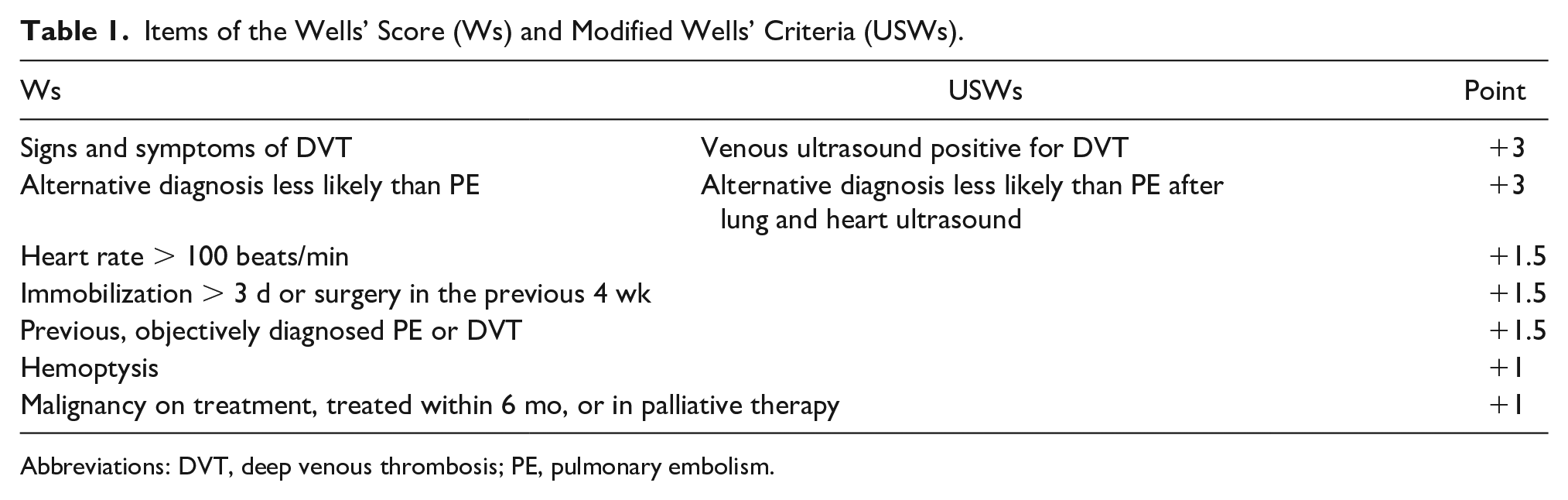
Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism.
Computed tomography pulmonary angiography
All CT angiographic examinations were performed by a 128-multi slice CT equipment (GE Light Speed 7.0 CT Scanner System; GE Medical Systems, Waukesha, WI, USA; Figure 2).
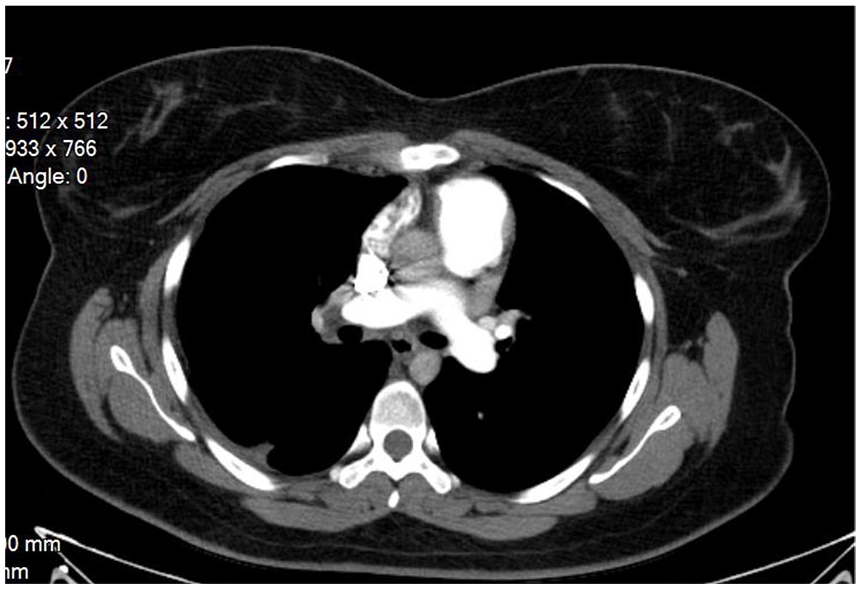
The mediastinal view of pulmonary embolism.
Outcomes
First, the clinical and demographic symptoms, signs, and parameters of patients were obtained and recorded. Then, D-dimer, venous US, and lung and heart TTUS were performed, and their results were recorded. The diagnostic values of the Wells’ criteria and WDVTC (with and without D-dimer values) were addressed.
Statistical analysis
SPSS software Version 22 was used to analyze the collected data. The data were expressed as means, ±standard deviation, or frequency (percentage). Independent samples t test and Fisher's exact test were, respectively, used to compare the means of quantitative variables and the frequency distribution of qualitative variables for patients with and without PE. Furthermore, a receiver operating characteristic (ROC) analysis was used to evaluate the sensitivity, specificity, positive, and negative predictive value of WDVTCs alone and in combination with D-dimer results. This was also compared with CT angiography for predicting PE. Significance levels less than P < .05 were considered in all analyses.
Results
Demographic and clinical factors
In the present study, CTPA was performed for 104 cases with a probable diagnosis of PE. There were 39 (37.5%) CTPA cases positive for PE, and 65 (62.5%) patients were negative.
The gender of positive findings for PE were 30 (76.9%) men and 9 (23.1%) women. The mean age of positive cases was 51.26 ± 13.49 years (P < .05). This was compared to 34 (52.3%) men and 31 (47.7%) women that tested negative for PE and had a mean age of 59.31 ± 17.99 years (P < .05). Evaluating the clinical signs and symptoms for PE revealed that a frequency of diaphoresis, increased P2 heart sounds, and breathing wheeze were significantly higher compared to patients without PE (P < .05; Tables 2 and 3).
Symptoms of Presentation and Summary of Wells’ Criteria.
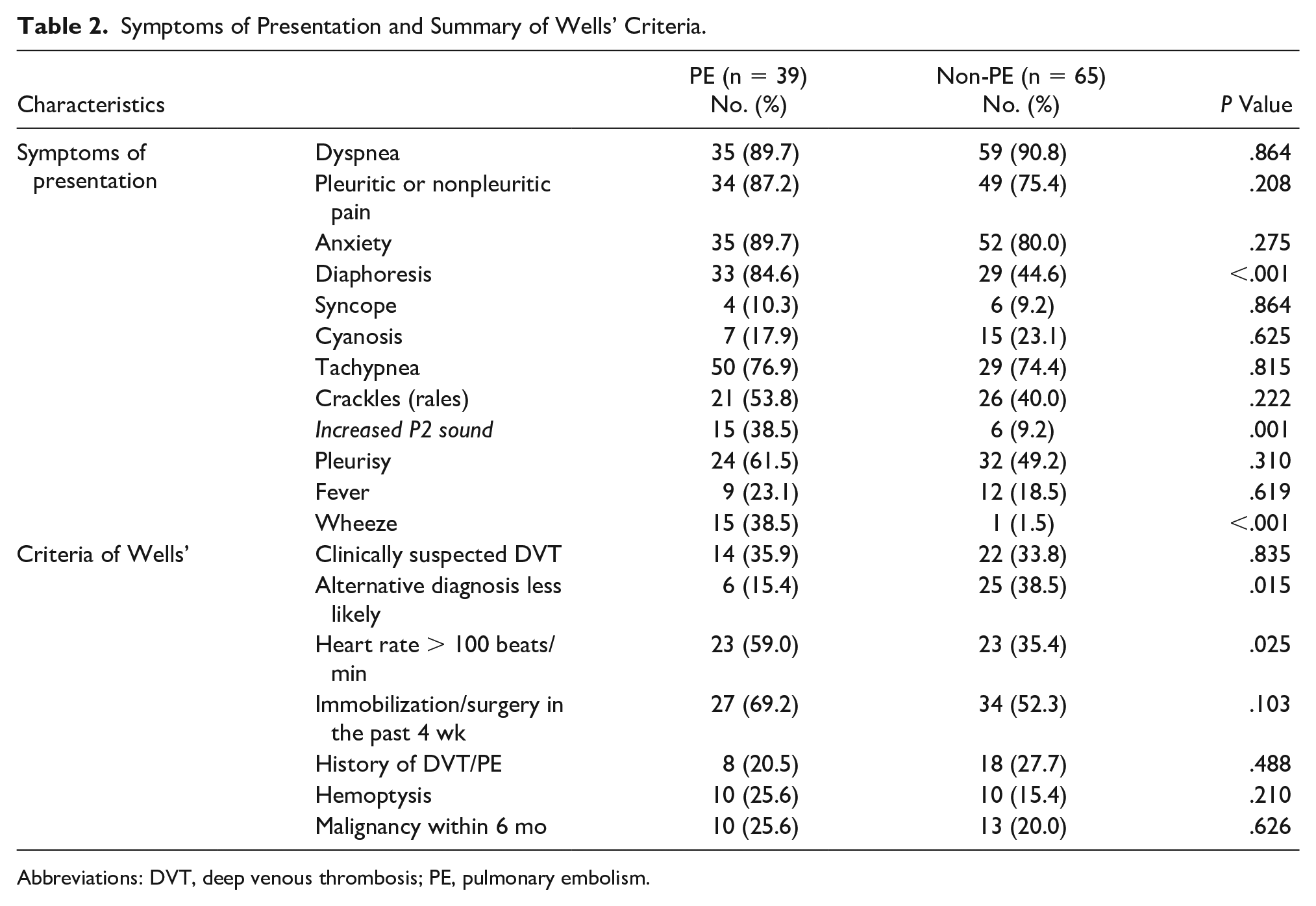
Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism.
Determination and Comparison of Gender, Age, and Clinical Factors of Patients With and Without Pulmonary Embolism (PE). a
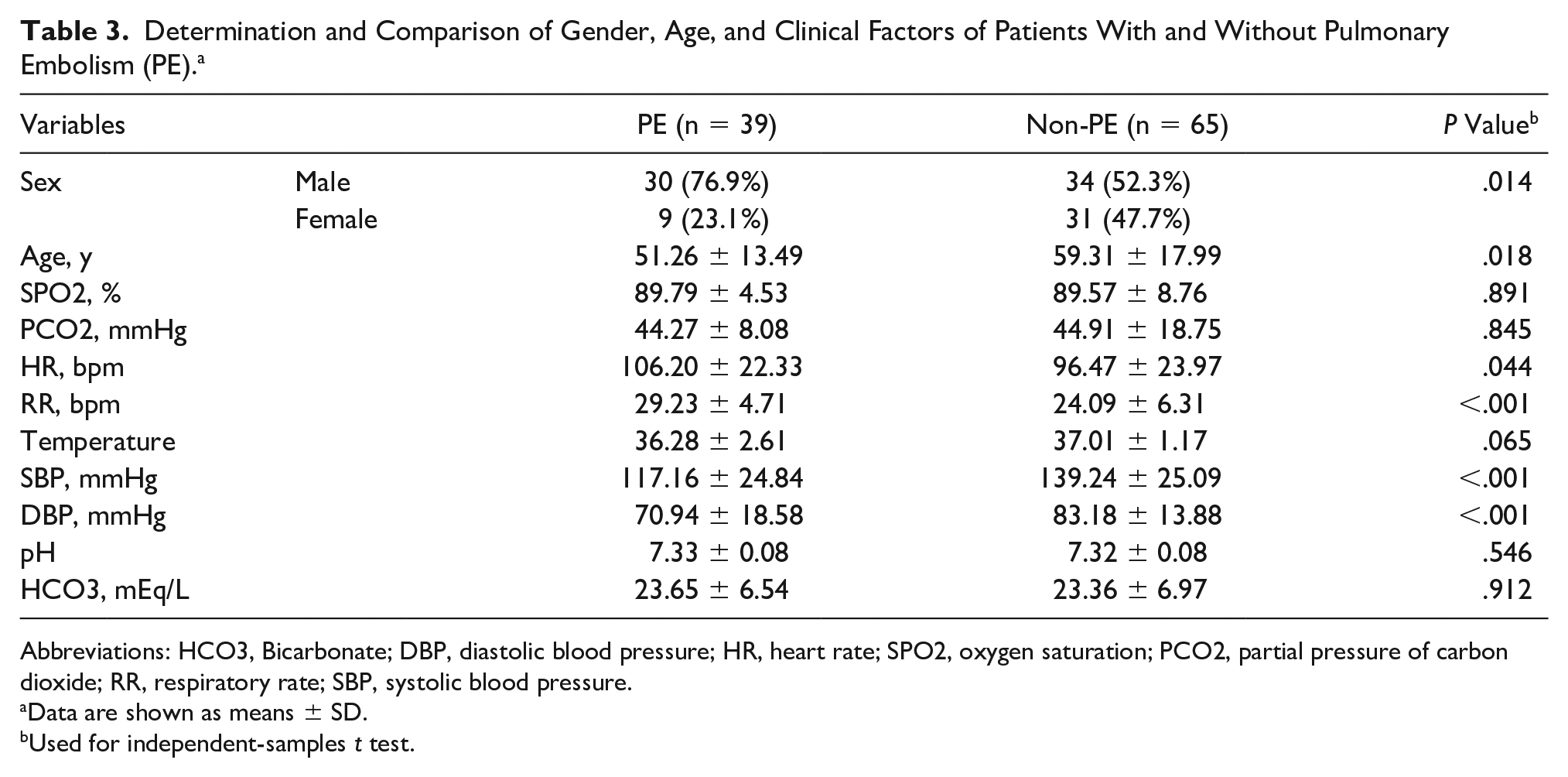
Abbreviations: HCO3, Bicarbonate; DBP, diastolic blood pressure; HR, heart rate; SPO2, oxygen saturation; PCO2, partial pressure of carbon dioxide; RR, respiratory rate; SBP, systolic blood pressure.
Data are shown as means ± SD.
Used for independent-samples t test.
In addition, the evaluation of the clinical factors indicated that heart and respiratory rates among patients with PE were 106.20 ± 22.33 and 29.23 ± 4.71 beats/min, respectively. It was higher than those of non-PE patients with the means of 96.47 ± 23.97 and 24.09 ± 6.31 beats/min, respectively (P < .05). In contrast, the systolic and diastolic blood pressures among PE patients were a mean of 117.16 ± 24.84 and 70.94 ± 18.58 mm HG, respectively. This was significantly lower than those patients without a PE, who had systolic and diastolic blood pressure means of 139.24 ± 25.09 and 83.18 ± 13.88 mm HG, respectively (Table 3).
D-dimer, Venous US, Lung and heart TTUS
The D-dimer was positive in 74.4% of PE patients and 76.9% of non-PE patients (P = .767). Furthermore, positive D-dimer (>500 μg/L) also had no significant diagnostic value for PE (area under curve [AUC] = 0.513, P = .771). But positive findings by venous duplex US and lung and heart TTUS were significant for PE (P < .001; Table 4).
Diagnostic Value of D-dimer, Venous US, and Lung and Heart TTUS.
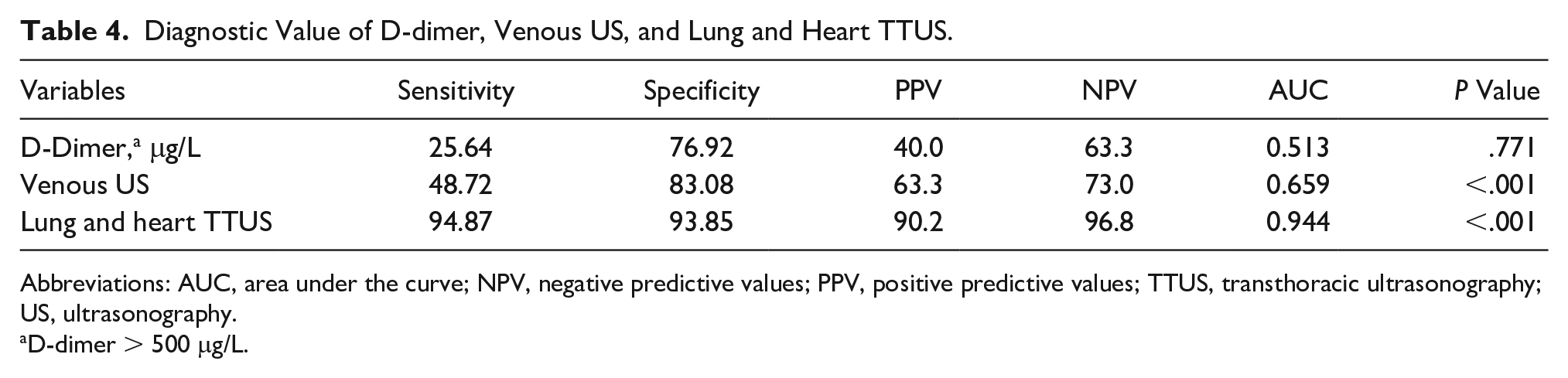
Abbreviations: AUC, area under the curve; NPV, negative predictive values; PPV, positive predictive values; TTUS, transthoracic ultrasonography; US, ultrasonography.
D-dimer > 500 μg/L.
Wells’ criteria versus WDVTCs
Wells’ criteria for the diagnosis of PE did not have a high diagnostic value (AUC = 0.502, P = .973). This was compared to WDVTCs with a cutoff point of 4 (AUC = 0.992, P < .001) and had significant diagnostic values for PE (Table 5, Figure 3).
Specification of the Diagnostic Value of Ws and USWs for PE.
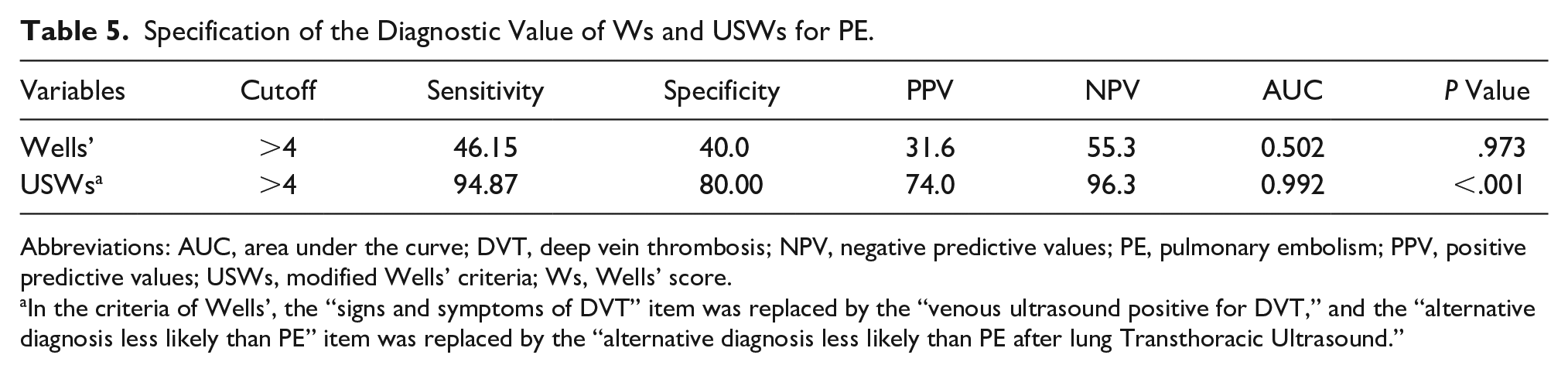
Abbreviations: AUC, area under the curve; DVT, deep vein thrombosis; NPV, negative predictive values; PE, pulmonary embolism; PPV, positive predictive values; USWs, modified Wells’ criteria; Ws, Wells’ score.
In the criteria of Wells’, the “signs and symptoms of DVT” item was replaced by the “venous ultrasound positive for DVT,” and the “alternative diagnosis less likely than PE” item was replaced by the “alternative diagnosis less likely than PE after lung Transthoracic Ultrasound.”
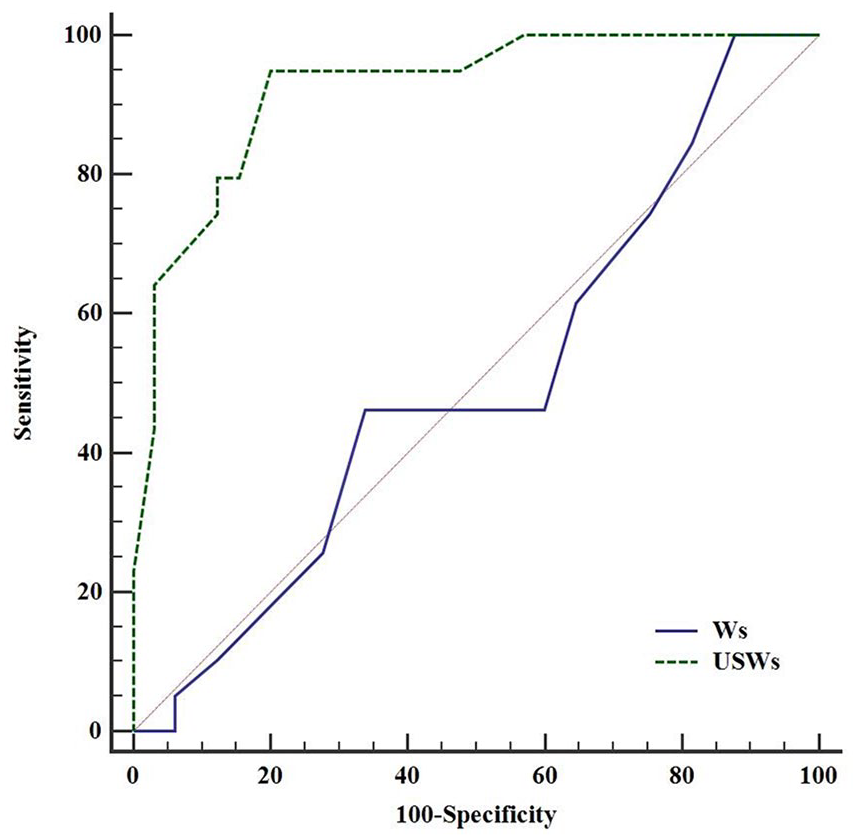
Receiver operating characteristic curve to compare the diagnostic value of the Wells’ criterion in combination with venous, lung, and heart sonography.
Combination of D-dimer and WDVTCs
Combining a positive D-dimer with WDVTCs > 4 had a sensitivity and specificity equal to 69.23% and 80%, respectively (P < .001). Moreover, the combination of positive D-dimer with WDVTCs ≤ 4 had a sensitivity and specificity of 94.87% and 56.92%, respectively (P < .001). In fact, it may be argued that a positive D-dimer had a higher sensitivity in non-PE patients. In addition, the diagnosis of negative PE with a negative D-dimer had a specificity of 100% and sensitivity of 23.08% in “unlikely PE” patients and had sensitivity of 100% and specificity of 25.64% in “likely PE” patients. In summary, to rule out a PE by negative D-dimer in unlikely patients had higher accuracy but did not have appropriate accuracy in likely PE patients (Table 6).
Specification of the Diagnostic Value of D-dimer Along With the Modified Wells’ (USWs) Criteria in PE Detection or Rule-Out.
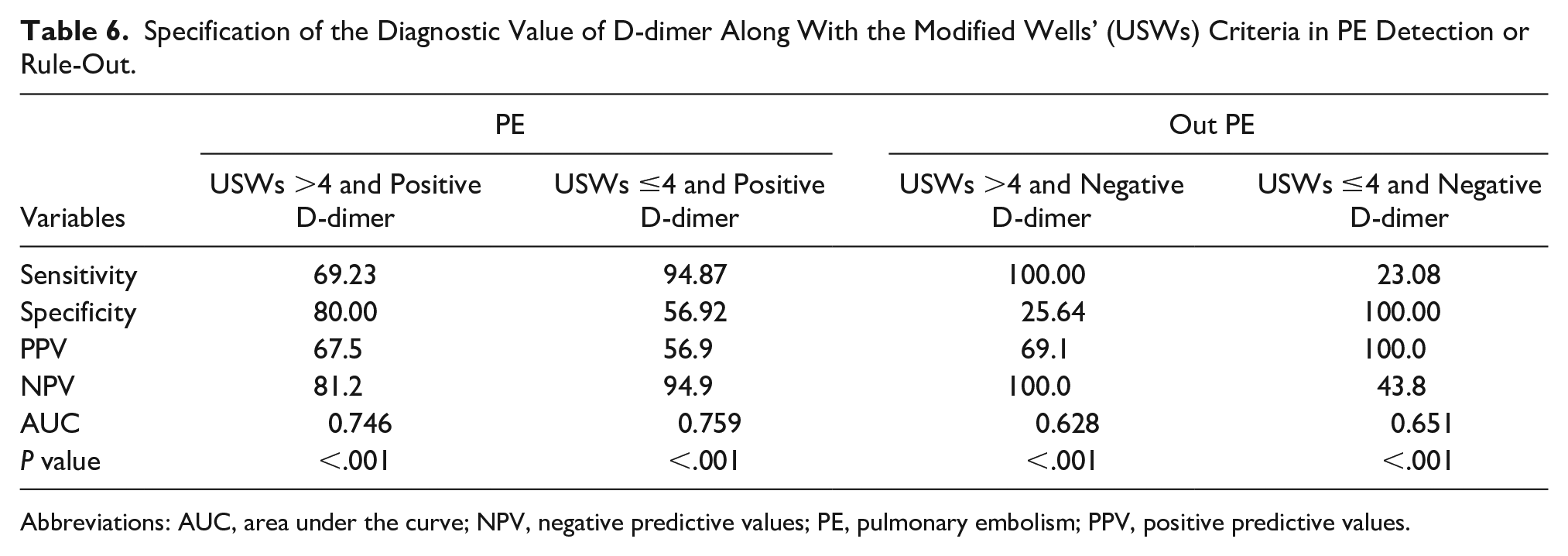
Abbreviations: AUC, area under the curve; NPV, negative predictive values; PE, pulmonary embolism; PPV, positive predictive values.
Discussion
A PE is a clinical emergency and needs to be rapidly identified. But without specific clinical symptoms and a diagnostic gold standard, this can be challenging. While radiographic testing with CT is the most common confirmatory exam, it is resource-intensive. CT also exposes the patient to ionizing radiation and potential contrast-related injuries, which underscores the risks to patients. 17 There are several clinical decision rules as an alternative means to evaluating and managing the risk of PE. Most of these rules are subjective factors and can frequently help in identifying those at low risk; however it is unlikely to properly exclude PE for those patients at moderate or high risk. Point-of-care ultrasonography is considered a powerful diagnostic tool and assists in the integration of clinical assessments. Bedside ultrasonography has many advantages, such as being noninvasive and having rapid results. Combining sonography with the traditional Ws system may help to improve the use of CTPA and decrease its use in unstable patients. The combined use of D-dimer with clinical scores, such as the Ws, and the use of CTPA for a final diagnosis is recommended. This has been highlighted in international guidelines for suspected PE as a way to optimize the diagnostic process. These rules may be sufficient in classifying suspected PE patients but may not be applicable for all patients.18,19
According to these study results, D-dimer alone had a sensitivity of 25.64% and a specificity of 76.92% but did not have an acceptable accuracy for PE. However, findings from venous duplex sonography, lung, and heart TTUS could have a significant diagnostic value for PE.
Previous studies have suggested that a D-dimer test alone has low diagnostic value for PE, whereas a negative D-dimer combined with low clinical probability (based on Ws) can rule out suspected PE.20–22 In fact, the D-dimer had a sensitivity of 96% to 98% and has a high negative predictive value in patients “unlikely for PE.” 5
Additionally, a meta-analysis published by Jiang et al. 23 found that lung TTUS had an average sensitivity and specificity of 85% and 83% and was effective for diagnosing PE. Another study revealed that the sensitivity, specificity, and accuracy of TTUS in patients with PE were 71.4%, 80.9%, and 87.1%, respectively. 24
The present study revealed that integrating sonography of the lung, heart, and lower limbs veins increased the accuracy of PE diagnosis. Actually, the accuracy of the Ws criteria significantly increased when the “signs and symptoms of DVT” item was replaced by the “positive venous duplex for DVT” and the “alternative diagnosis less likely than PE” item was replaced by the “normal lung and heart sonographic findings.” The WDVTCs had a sensitivity of 94.87%, specificity of 80.00%, and AUC of 0.99.
Consistent with the findings of the present study, Nazerian et al.’s 14 study also indicated the accuracy and specificity of Ws criteria as compared to the modified Ws criteria (combined results of lung and vascular ultrasound) to be 57.6% versus 69.6% and 68.2% versus 88.2%, respectively.
It may be argued that evaluation of some biomarkers (e.g., D-dimer) in emergency cases may not be feasible or that their evaluation alone may not be very effective in diagnosis of PE. However, their evaluation in combination with another diagnostic criterion such as sonography may yield better and more effective results. 25
Hence, to achieve a more precise diagnostic value, the combination of D-dimer with the WDVTCs criteria were considered, and it was found that positive D-dimer in “unlikely for PE” patients (WDVTCs ≤ 4) increased the sensitivity for PE, but its specificity and positive predictive value decreased. Moreover, it was revealed that in “unlikely PE” patients, WDVTCs ≤ 4 and a negative D-dimer had the best accuracy in ruling out PE. Consistent with the findings of the present study, Nazerian et al. 14 used the D-dimer along with Ws criteria for ruling out PE. This revealed that ruling out PE in patients with Ws ≤ 4 and negative D-dimer had a sensitivity, specificity, and failure rate of 98.2%, 36.8%, and 1.9%, respectively. Moreover, the sensitivity, specificity, and failure rate in Ws ≤ 4 and negative a D-dimer in patients were 99.1%, 44.6%, and 0.8%, respectively. In fact, in line with the present study, Nazerian et al. 14 declared the use of US or TTUS in addition to biomarkers such as D-dimer to be more effective and indicated that this combination can enhance diagnostics for PE.
Therefore, the current study results revealed that in “patients unlikely for PE with WDVTCs” (WDVTCs ≤ 4), a negative D-dimer was most accurate in ruling out PE. And it may be argued that the use of sonography of the lower extremity veins, lungs, and heart could have advantages in improving the diagnostic value of PE.
Limitations
Due to the small sample size and lack of randomization, further studies need to be performed. Furthermore, given that the accuracy of ultrasonography is highly operator dependent, the clinicians need sufficient training before conducting this type of research.
Conclusion
The authors suggest adding the results of sonography of the lower extremity veins, lungs, and heart to the Wells’ criteria in order to increase overall diagnostic value. Conversely, in cases with WDVTCs ≤ 4 and a negative D-dimer, PE can be ruled out with specificity equal to 100%. Therefore, it can be stated that the combination of WDVTCs with D-dimer may lead to an improved performance of the risk stratification and decreased application of CTPA in the diagnosis of PE while maintaining patient safety.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.