
Abstract
Catheter obstruction is a serious complication associated with peritoneal dialysis (PD). Diagnostic imaging techniques play a role in the management of patients undergoing PD, mainly in detecting potential catheter-related complications. Imaging can help in the treatment decision process. Visualizing the obstruction and understanding the etiology are crucial for accurate management of patients and in determining therapeutic strategies. Although a PD catheter obstruction can be diagnosed using magnetic resonance imaging (MRI), ultrasonography (US) has been reported to be equally effective. The effectiveness of US and MRI in detecting PD catheter obstructions was compared in four pediatric patients. These cases demonstrate that US was more useful in visualizing PD obstruction compared with MRI. US can be repeated more conveniently and is noninvasive, especially in children. US can be considered an effective tool for diagnosing PD catheter obstruction in children.
Peritoneal catheter malfunction has been described as mechanical failure during dialysate inflow or outflow. It is a common problem for patients undergoing peritoneal dialysis (PD). Outflow failure occurs in 4% to 34.5% of patients undergoing PD. 1 This may be due to abnormal catheter position, fibrin deposition, omental wrapping, and entering of visceral organs such as tubal fimbria into the catheter. 1 Since the introduction of the first permanent silicone catheter in 1968, a wide variety of catheters and placement techniques have been developed to eliminate catheter malfunction. However, catheter-related problems are still not fully resolved for patients.2,3
The closure of a dialysis catheter is a serious condition in PD. Diagnostic imaging techniques play an important role in the treatment decision process and the management of patients undergoing PD, particularly for the detection of possible catheter-related complications. Visualizing the obstruction and understanding the etiology are crucial for accurate management of patients and for determining subsequent therapeutic strategies. However, in some cases, diagnosing PD obstructions may be difficult because of insufficient noninvasive imaging methods. Many of these PD catheter obstructions are often diagnosed with magnetic resonance imaging (MRI). Ultrasonography (US) has also been reported to be equally effective in diagnosing PD catheter obstructions. 4
Hence, the objective of this case study was to compare the effectiveness of US and MRI in the diagnosis of PD catheter obstructions among four pediatric patients.
Case Series Report
The selected patients (four female patients ranging in age from 2 years to 16 years) were treated with PD at a tertiary hospital. The swan-neck two-cuff catheter was used in all subjects. Numerous spaced holes of 0.5 mm in diameter found in the intra-abdominal area allowed the inflow and outflow of the dialysate throughout the peritoneal cavity. US was performed using Nemio XG (Toshiba-Canon Medical Systems, Inc, Tokyo, Japan) with a convex 3.75-MHz and a linear 8-MHz transducer. The PD catheter with its entire length was visualized as a “sandwich structure” consisting of a double-layered hyperechoic band depicting the anterior and posterior sides of the catheter (Figure 1).
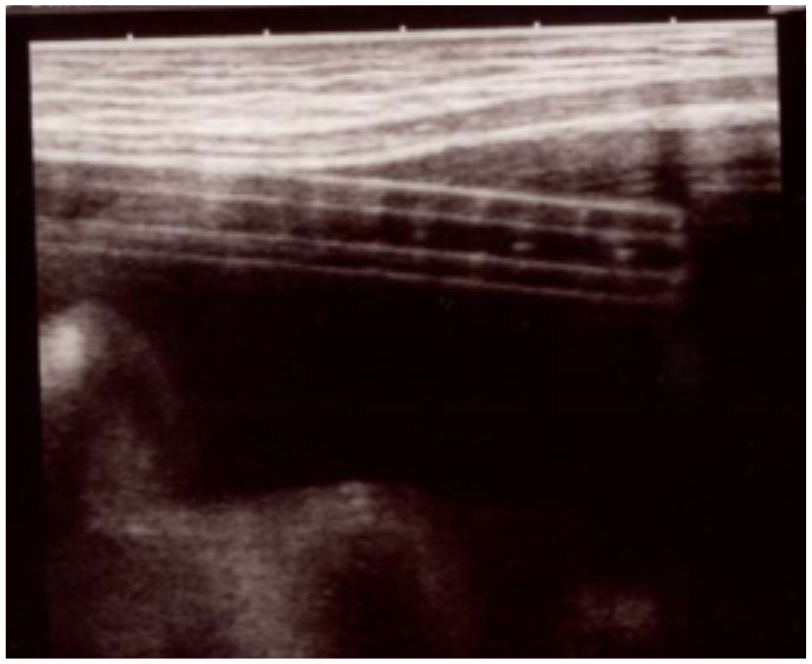
The peritoneal dialysis catheter resembles a “sandwich structure” consisting of a double-layered hyperechoic band representing the anterior and posterior sides of the catheter.
All procedures performed in these studies involved human participants and were consented in accordance with the ethical standards of the hospital’s Institutional Review Committee. These consents were also informed by the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards (64th WMA General Assembly, Fortaleza, Brazil, October 2013). Additional informed consent for US and MRI examinations and to publish their cases was obtained from patients and/or their family members.
Patient Case 1
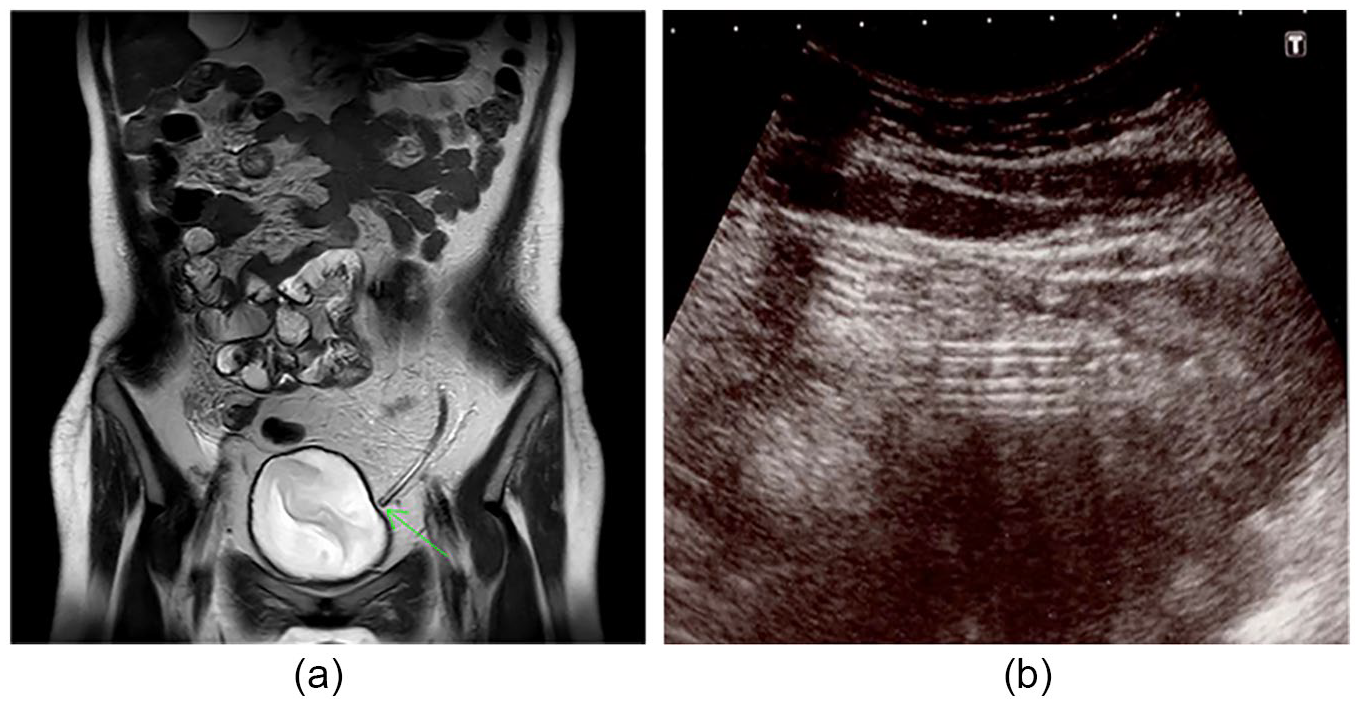
A 2-year-old girl with end-stage renal disease (ESRD), caused by steroid-resistant nephrotic syndrome, was introduced to continuous ambulatory PD (CAPD) at the hospital. Outflow failure was noted in this patient 2 weeks later. A radiograph of the kidney, ureter, and bladder (KUB) did not show catheter tip migration. Because of high levels of fibrin in the dialysate and slow outflow, urokinase and heparin were injected into the catheter. Although the speed of inflow and outflow was slow, complete absence of outflow occurred immediately after injection. To investigate and subsequently resolve the cause of the catheter obstruction, MRI and US were performed on this patient. MRI with T1-weighted image (T1WI) revealed a hyperintense signal. MRI with T2-weighted image (T2WI) revealed a hypointense signal that measured approximately 2 cm and was located 3 cm from the tip of the catheter (Figure 2a). US revealed a hyperechoic amorphous material as a homogeneous area at the same location (Figures 2b, c). Findings from both the MRI and US studies indicated catheter obstruction. Laparoscopic surgery was performed under general anesthesia to restore PD catheter function. Surgical findings revealed that the omentum entered a part of the catheter, as observed on MRI and US. After the obstruction was removed, catheter function resumed, and the patient continued receiving PD.
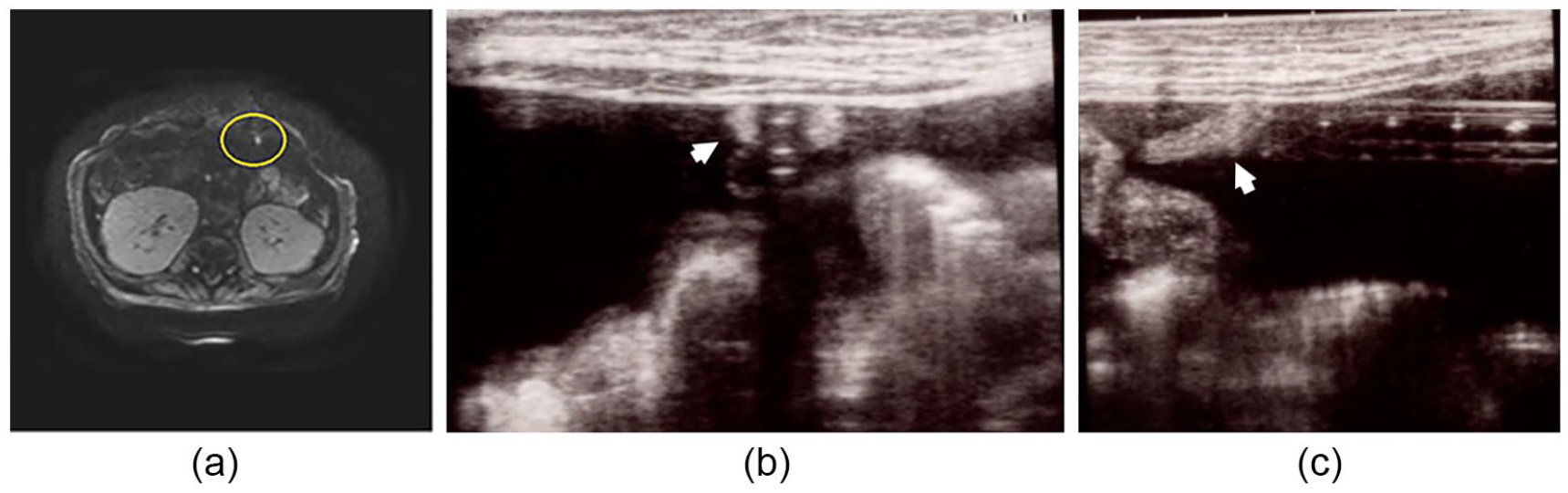
Magnetic resonance imaging (MRI) and ultrasonography (US) findings in patient case 1. (a) MRI with T1-wighted image revealed a high-signal area of approximately 2 cm, which was located 3 cm from the tip of the catheter, indicated by a circle. (b, c) US revealed a hyperechoic amorphous material as a homogeneous area around the side hole of the catheter in the transverse (b) and the longitudinal scans (c), as indicated by arrows.
Patient Case 2
A 2-year-old girl with ESRD caused by steroid-resistant nephrotic syndrome was introduced to CAPD. Outflow failure was noted 2 months later. A KUB radiograph did not show catheter tip migration. Because of high levels of fibrin in the dialysate and slow outflow, urokinase and heparin were injected into the catheter. However, the outflow did not improve, and there was subsequently complete absence of outflow. To investigate and resolve the cause of the catheter obstruction, MRI and US were performed. MRI with T1WI revealed a hyperintense signal in the area of the catheter. MRI with T2WI revealed a hypointense signal at approximately 1.5 cm from the tip of the catheter (Figure 3a). US revealed hyperechoic materials around the tip of the catheter (Figure 3b) and in the catheter lumen at the side holes, which was the same site as that found on MRI (Figure 3c). The diagnostic findings from both MRI and US were indicative of obstruction. Laparoscopic surgery was performed under general anesthesia to restore PD catheter function. Surgical findings revealed that the omentum strayed from the side holes of the catheter, similar to what was observed on MRI and US. Moreover, the fallopian tube strayed into the tip of the catheter, observed only on US. Catheter obstructions were released, and the patient continued PD.
Magnetic resonance imaging (MRI) and ultrasonography (US) findings in patient case 2. (a) MRI with T2-weighted image revealed a low-signal area at approximately 1.5 cm from the tip of the catheter, as indicated by an arrow. (b, c) US revealed hyperechoic materials at the lumen in the side holes of the catheter around the tip (b) and around the tip of the catheter (c), as indicated by arrows.
Patient Case 3
A 13-year-old girl with ESRD caused by microscopic polyangiitis was introduced to PD at 12 years of age. The omentum was partially resected to prevent it from entering the PD catheter. However, outflow failure occurred 1 year later. A KUB radiograph again demonstrated no catheter tip migration. Moreover, no catheter outflow was detected. To investigate and subsequently resolve the cause of the catheter obstruction, MRI and US were performed. MRI with T2WI revealed a hypointense signal at approximately 3 cm from the tip of the catheter (Figure 4a). US revealed hyperechoic materials at the same site as that found on MRI (Figure 4b) and around the tip of the catheter (Figure 4c). Findings of both MRI and US were diagnostic for obstruction. Laparoscopic surgery was performed under general anesthesia to restore PD catheter function. The surgical findings revealed that the ovary strayed into the side holes of the catheter, similar to what was observed on MRI and US (Figure 5a), and the fallopian tube strayed into the tip of the catheter, as observed only on US (Figure 5b). Catheter obstructions were released, and the patient continued PD.
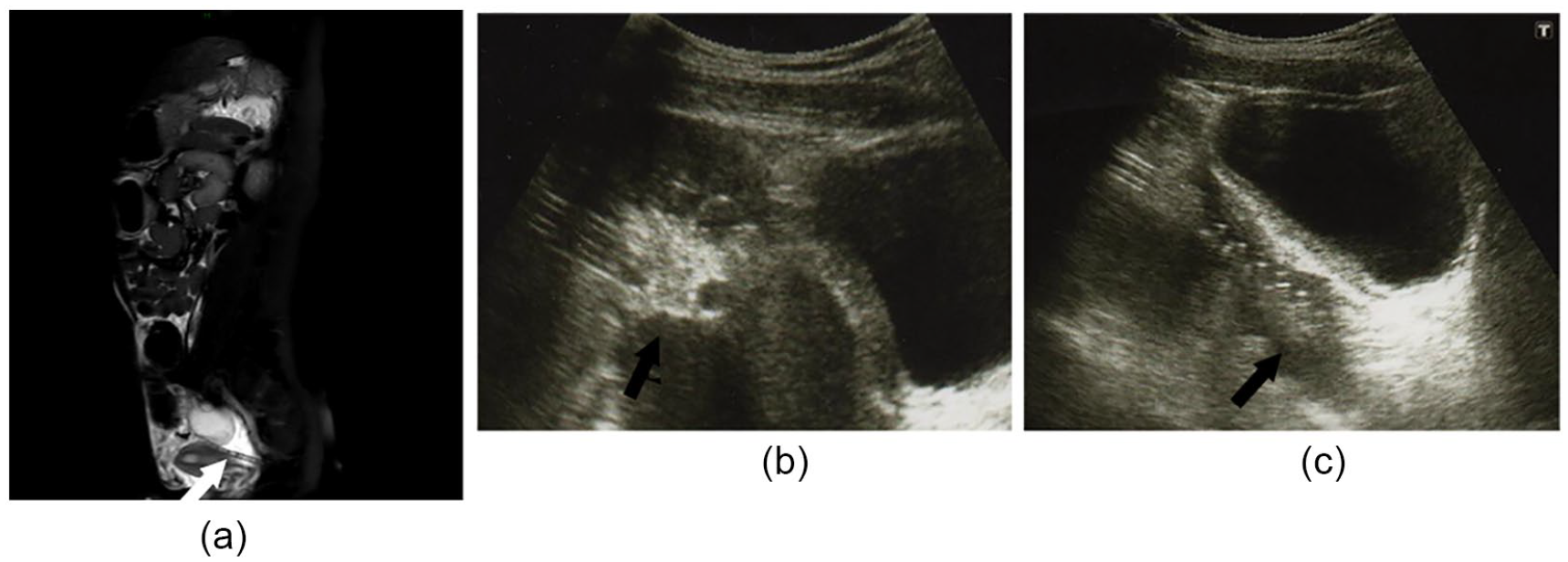
Magnetic resonance imaging (MRI) and ultrasonography (US) findings in patient case 3. MRI with T2-weighted image revealed a low-signal area at approximately 3 cm from the tip of the catheter, as indicated by an arrow (a). US revealed hyperechoic materials around the side holes (b) and the tip of the catheter (c), as indicated by arrows.
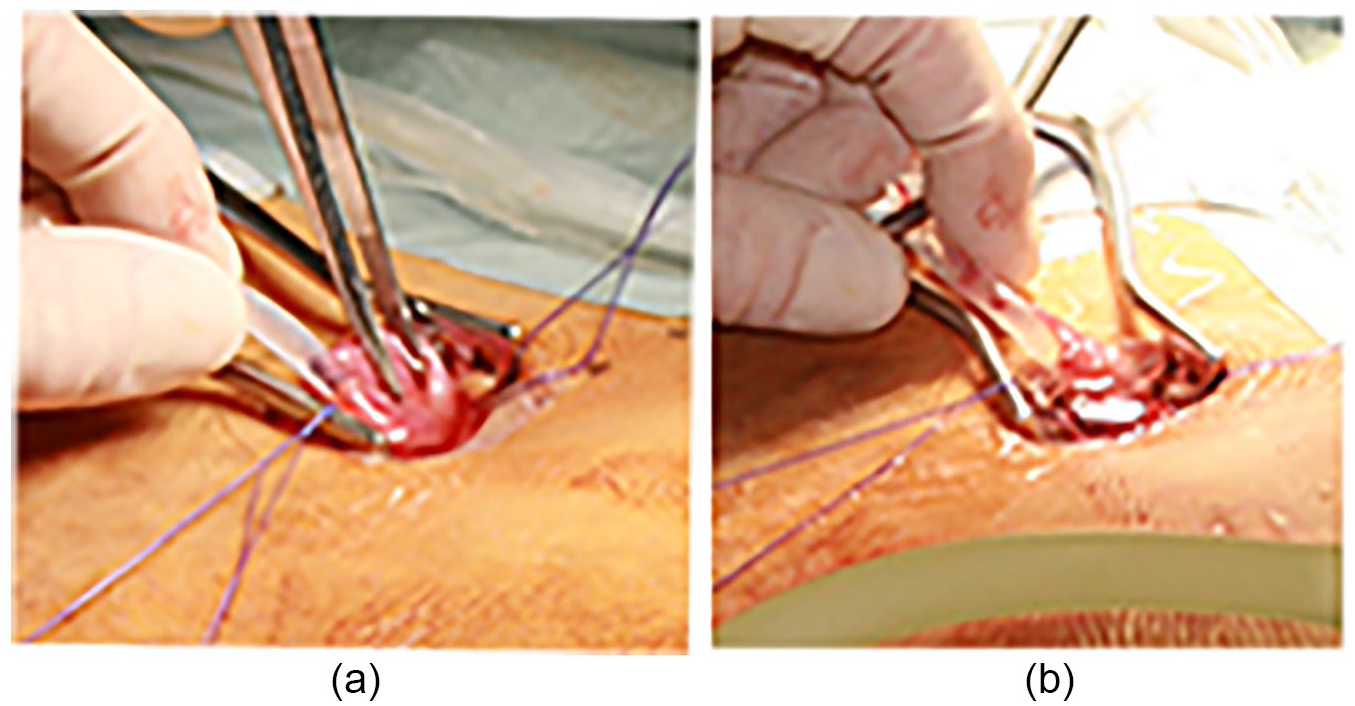
An ovary is observed on the catheter’s center side (a) and fallopian tube on the peripheral side (b).
Patient Case 4
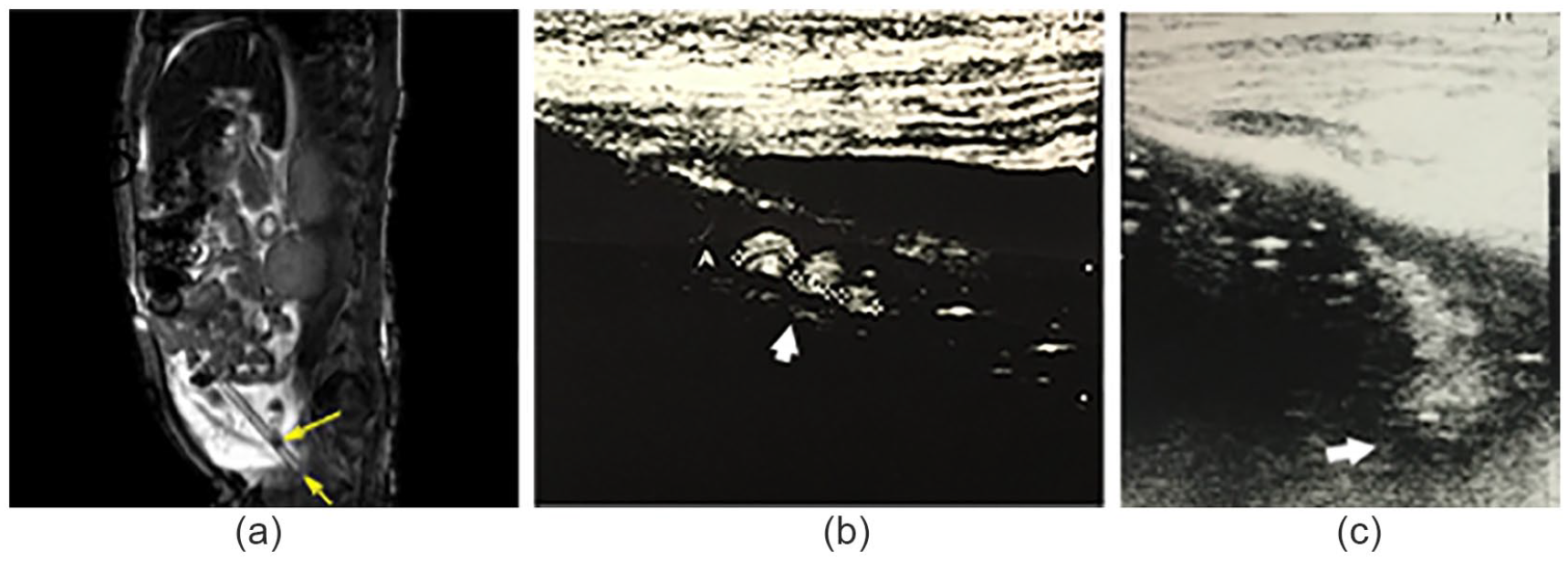
A 16-year-old girl with ESRD caused by type 1 glycogen storage disease was introduced to CAPD. However, the desired peritoneal effluent drainage was not achieved. A KUB radiograph revealed displacement of the catheter tip. This was corrected by performing an alpha replacement maneuver using a guidewire under fluoroscopy. However, the catheter outflow failure was not resolved. The catheter was injected with urokinase and heparin, but the inflow and outflow did not improve. To investigate and eventually resolve the cause of the catheter obstruction, MRI and US were performed. MRI with T2WI revealed a high signal around the catheter, but it was not clear whether the omentum had become entangled (Figure 6a). However, US revealed an amorphous structure as a homogeneous echoic area around the broad area of the catheter; hence, an omental occlusion around the catheter was suspected (Figure 6b). Laparoscopic surgery was performed under general anesthesia to restore the PD catheter function. Surgical findings revealed that the omentum was wrapped around the entire circumference of the catheter and strayed into the lumen; these findings were seen only on US. The catheter obstruction was released, and partial omental resection was performed. Subsequently, the catheter functioned properly, and the patient was able to continue PD.
Magnetic resonance imaging (MRI) and ultrasonography (US) findings in patient case 4. MRI with T2-weighted image revealed that there was no clear high signal around the catheter (a). US revealed an amorphous material as a homogeneous echoic area around the broad area of the catheter (b).
Discussion
This case series reported on four patients with PD catheter obstruction (Table 1). Patient ages ranged from 2 years to 16 years, and all patients were all females. The causes of catheter obstructions in the patients presented were omental wrapping around the catheter in 3 patients and catheter entrance into the fallopian tube in 2 patients and into the ovary in 1 patient. US detected all causes of catheter obstructions. On MRI, it was difficult to detect four of seven obstructions. In this case series, US better visualized the source of the PD catheter obstruction than MRI did.
Summary of Cases.
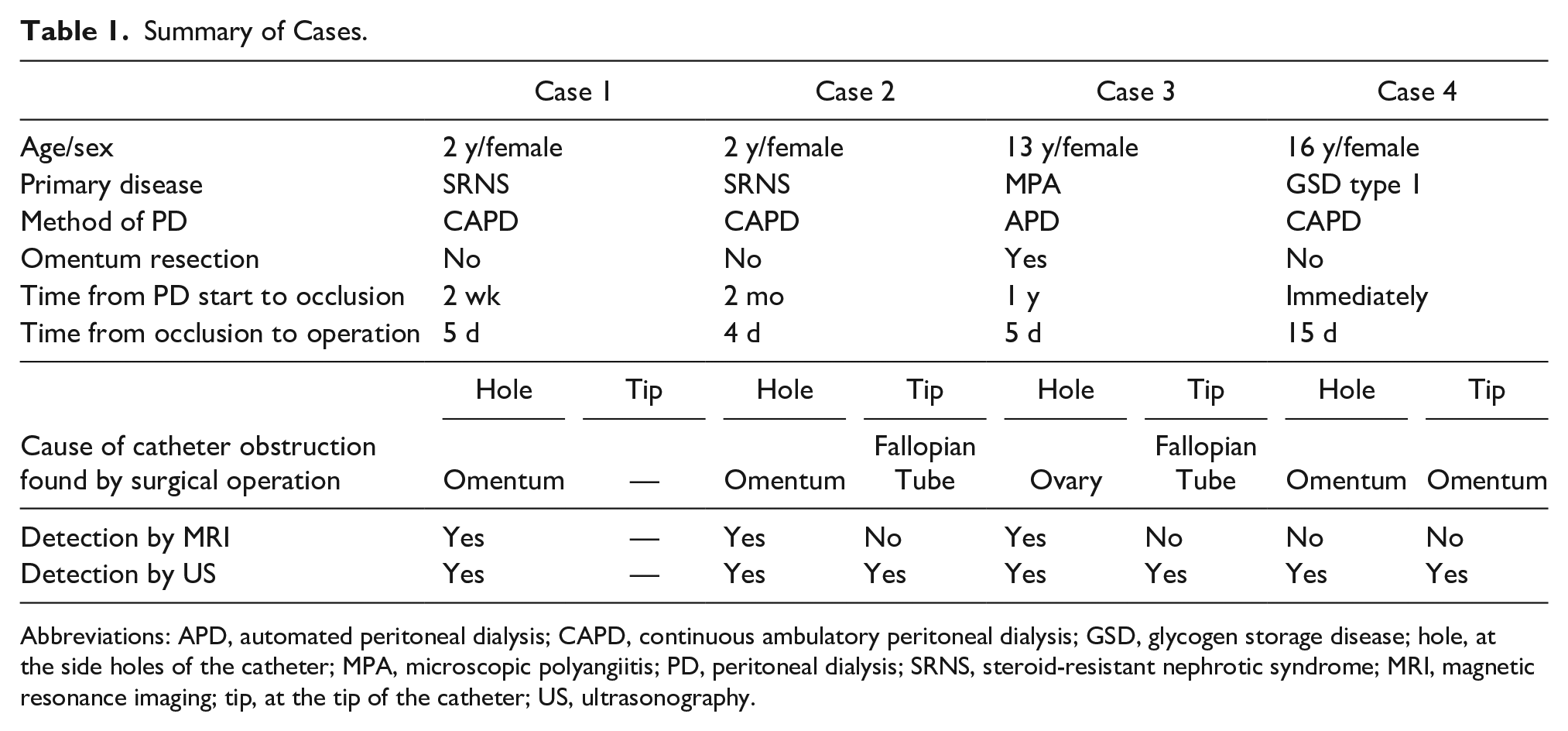
Abbreviations: APD, automated peritoneal dialysis; CAPD, continuous ambulatory peritoneal dialysis; GSD, glycogen storage disease; hole, at the side holes of the catheter; MPA, microscopic polyangiitis; PD, peritoneal dialysis; SRNS, steroid-resistant nephrotic syndrome; MRI, magnetic resonance imaging; tip, at the tip of the catheter; US, ultrasonography.
Despite the improvements observed in catheter-related survival, some complications remain as causes of morbidity and treatment failure in children on PD. 5 Catheter infections and peritonitis continue to be the most common complications of PD. 6 Moreover, US is an appropriate method to assess PD patients.7,8 A common noninfectious complication of PD catheters is catheter malfunction, which can occur for several reasons. First, catheter malposition causes migration, and this can be determined by reviewing a KUB radiograph. The radiograph can also be used to assess for kinks in the catheter and may be corrected by an alpha replacement maneuver, with a guidewire under fluoroscopy. This was illustrated in patient case 4. Second, intraluminal obstruction can be caused by fibrin strands, blood clots, and entrance of visceral organs into the catheter. In the cases presented, this was demonstrated by a high signal area in MRI with T1WI, a low signal area in MRI with T2WI, and a hypoechoic area on US in the catheter lumen. Fibrin strands and blood clots can be resolved by injecting urokinase and heparin or by mechanical removal using wire manipulation under fluoroscopy. Entrance into visceral organs is resolved by surgery. The third reason for catheter malfunction is extraluminal obstruction, which is mostly caused by the entanglement of the omentum. This can be noted with an amorphous structure such as a homogeneous echoic area on US. Unfortunately, it was not clear whether the omentum had become entangled. However, data on the role of imaging techniques in determining catheter obstructions are minimal.2–4,9 In some cases, the diagnosis of obstruction was made only after an invasive surgical approach. In these patients, US provided a high-resolution image of the peritoneal catheter. This allowed for visualization along the entire length of the catheter into the peritoneal cavity, the lumen, tracts, and intra-abdominal segments. Much of the diagnostic resolution was likely due to the ability to image children, who have a smaller body habitus than adults.
Based on the present cases, the efficacy between US and MRI for the diagnosis of PD catheter obstructions was compared. US detected obstructions that were supported with surgical findings but not as well as MRI did (Table 1). MRI was diagnostic for organs straying into the catheter, but it was difficult to observe whether organs wound around the catheter. In comparison, US was able to detect and diagnose both types of obstruction. Therefore, US detected and helped provide understanding of the etiology of catheter obstruction in these selected cases. Furthermore, US provides real-time imaging, and it can be an excellent tool in determining the location, size, and material of the obstruction. For these reasons, US has the potential to influence the subsequent therapeutic approach for patients. The present cases indicated that US can be the first choice of imaging technique when monitoring PD patients. US can be performed repeatedly anytime and anywhere, is noninvasive, and requires no ionizing radiation exposure.
This study had the following limitations. First, only a small sample of patients was included. Future studies with a higher number of patients are necessary to confirm these findings. As shown in all four cases, drainage failure occurred after injection of dialysate, which filled the abdomen and was easy to observe with US. The diagnosis using US would have been more difficult if the obstruction occurred after drainage and if the abdomen was not filled with dialysate. Involvement of the omentum in patient cases 1 and 2 occurred after PD started. The patients were hospitalized, and US was able to be performed sequentially for an accurate and quick diagnosis. In case 3, the abrupt deviation of the fallopian tube and ovary might have been due to the forceful application of negative pressure for approximately 4 hours. This was despite the continuous waste liquid failure alarm from the automated PD machine. In such cases, it may be important that automated PD be stopped and a US examination be performed at a hospital.
Conclusion
The present cases demonstrated that US was more useful in visualizing PD obstruction compared with MRI. In addition, US can be repeated more conveniently and is noninvasive, especially in children. This case series suggests that US can be an effective tool for diagnosing peritoneal catheter obstruction in children.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.