
Abstract
Lipoma arborescens is a rare synovial lesion characterized by villous proliferation of the synovial membrane and replacement of subsynovial tissue with mature fat cells. The knee joint is the most frequently affected site, particularly in the suprapatellar pouch. However, there have been few reports regarding shoulder involvement, including the glenohumeral joint and subacromial subdeltoid bursa, associated with rotator cuff tear. This article reviews the case of a 67-year-old man who presented with lipoma arborescens of the left shoulder, associated with a rotator cuff tear. Sonography revealed a fluid collection with thickening of the synovial membrane with hyperechoic villous proliferation, located in the subdeltoid bursa. An arthroscopic synovectomy and rotator cuff repair were performed. Arthroscopic findings included yellow frond-like synovial proliferation of the synovium. Postoperatively, the patient was asymptomatic, and the lesion did not recur. Although magnetic resonance imaging is the first-line imaging modality for diagnosis of this lesion, sonography may be used initially for evaluation of chronic joint swelling. In addition, it can be useful for detection of recurrence after synovectomy. This case illustrates the typical sonographic features of lipoma arborescens.
Lipoma arborescens is a rare synovial lesion characterized by villous proliferation of the synovial membrane and replacement of the subsynovial tissue, with mature fat cells. It most commonly affects the knee,1 –3 with few reports of other affected joints, including the shoulder.4 –9 Sonography can reveal a sonolucent effusion containing hyperechoic villous proliferation. In this article, a case of lipoma arborescens of the subdeltoid bursa associated with rotator cuff tear detected by sonography is discussed. In addition, sonography can be useful for the detection of recurrence after synovectomy.
Case Report
A 67-year-old man experienced left shoulder pain for eight months, with no history of trauma to the shoulder. He presented to another hospital due to acute increase in pain. He was prescribed nonsteroidal anti-inflammatory drugs and received several intra-articular injections. He continued to experience pain and swelling of the shoulder and presented to the hospital.
The patient’s medical history was unremarkable. Physical examination revealed swelling of the shoulder joint with mildly restricted range of motion during flexion, abduction, external rotation, and internal rotation. No significant weakness or muscle atrophy of the upper extremity was evident. Laboratory tests showed no significant results. Acute-phase reactants were normal and a rheumatoid factor was absent.
Radiography of the shoulder did not reveal any abnormalities. Sonography of the anterior shoulder showed a fluid collection with thickening of the synovial membrane and hyperechoic frond-like projection, within the subdeltoid bursa (Figure 1A,B). A supraspinatus tendon tear was also detected (Figure 1C). Magnetic resonance imaging (MRI) revealed a subdeltoid effusion containing villous proliferation with signal intensity similar to fat and a full-thickness tear of the supraspinatus tendon (Figure 2).
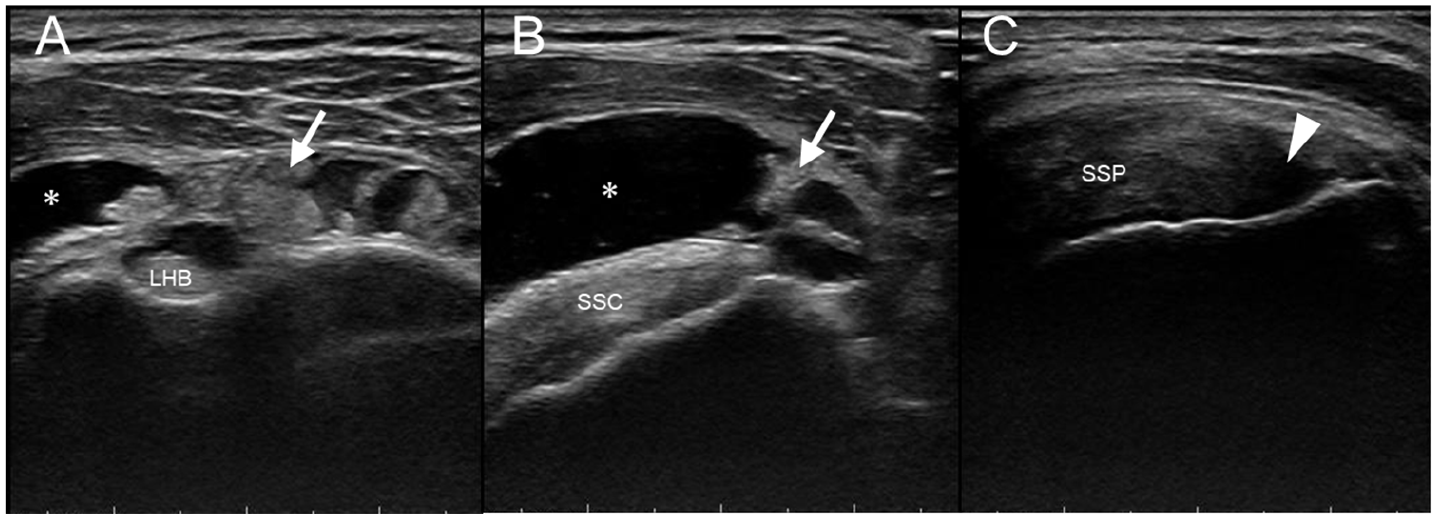
Sonographic image of the anterior left shoulder (A, B), showing a fluid collection (asterisk) with hyperechoic frond-like projections (arrows). (C) Supraspinatus tendon tear (arrowhead). LHB, long head of the biceps tendon; SSC, subscapularis tendon; SSP, supraspinatus tendon.
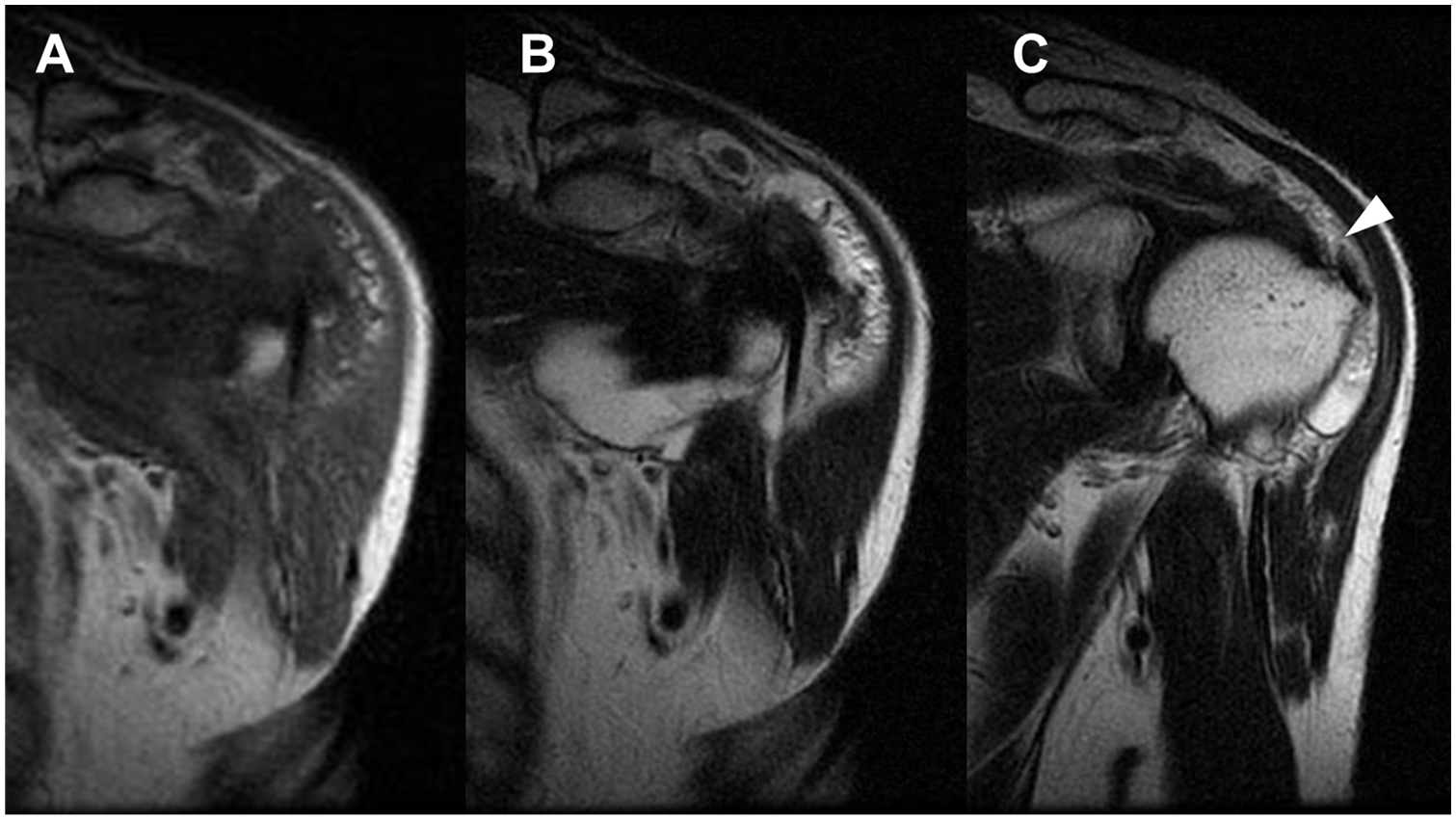
(A) T1- and (B) T2-weighted magnetic resonance images, revealing a subdeltoid effusion containing villous proliferation with signal intensity similar to fat. (C) Full-thickness tear of the supraspinatus tendon (arrowhead) is revealed on a T2-weighted image.
Because the patient had persistent pain, an arthroscopic synovectomy and rotator cuff repair was performed. Arthroscopic findings included yellow frond-like synovial proliferation of the synovium (Figure 3). After synovectomy, the supraspinatus tendon was repaired with suture anchors. Histologic examination revealed inflammatory changes in the synovial layer, and the synovial tissue was replaced by a villous mass composed of mature fat tissue (Figure 4). Nine months postoperatively, the patient was asymptomatic and his shoulder function was improved.
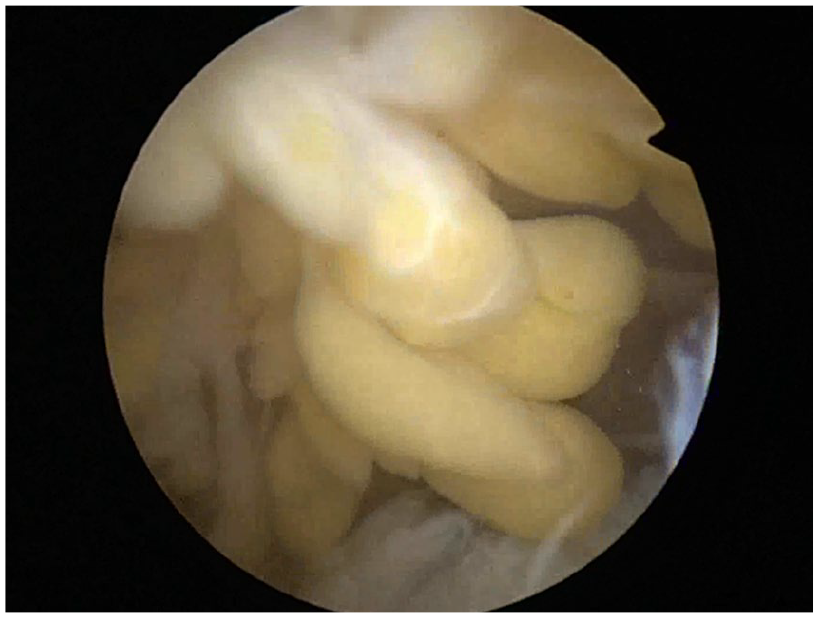
Arthroscopic findings of yellow frond-like proliferation of the synovium.
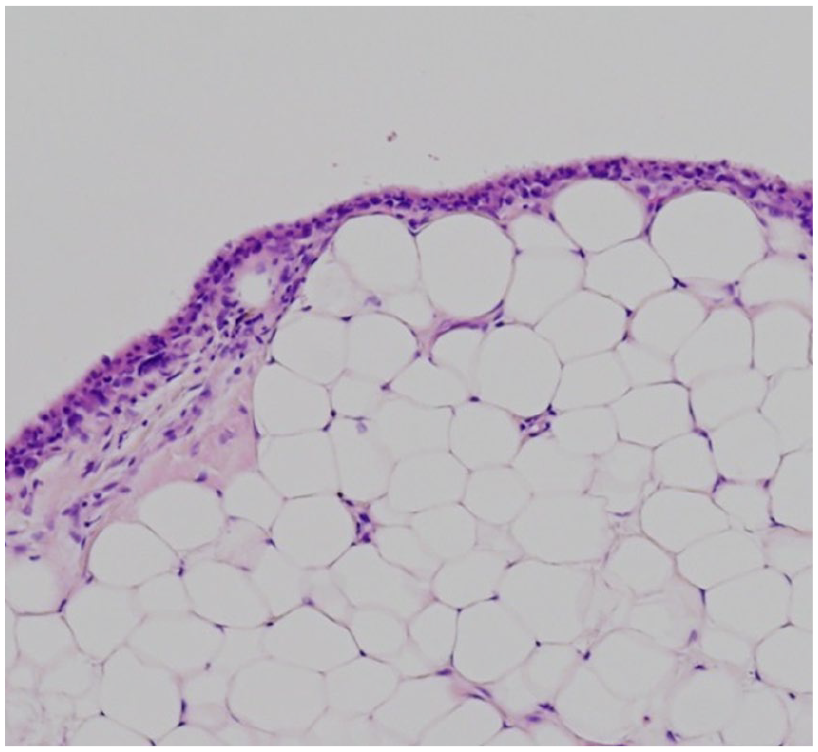
Histologic examination, showing inflammatory changes in the synovial layer and synovial tissue replaced by a villous mass composed of mature fat tissue (hematoxylin and eosin ×100).
Discussion
Lipoma arborescens is a benign villous proliferation of the synovium characterized by replacement of the subsynovial tissue with mature fat cells. The etiology of lipoma arborescens has not been clearly identified. It can be associated with degenerative joint disease, chronic rheumatoid arthritis, 10 psoriasis, 1 pseudogout, 11 or previous trauma. 12 Hallel et al. 13 reported that it is likely a reaction of the synovial tissue to inflammatory or traumatic stimuli rather than a true neoplastic lesion. The knee joint is the most frequently affected site, particularly in the suprapatellar pouch.1 –3 There have been several reports regarding shoulder involvement, including the glenohumeral joint4,5 and subacromial subdeltoid bursa, associated with rotator cuff tear.6 –9
Most cases of lipoma arborescens are diagnosed after an extensive use of magnetic resonance imaging (MRI) in clinical practice.14,15 Currently, MRI is the preferred imaging modality for the diagnosis because of its superiority in showing the nature of the content and morphologic features. The typical appearance of lipoma arborescens is a villous-like synovial mass with signal intensity similar to fat on all pulse sequences, which is suppressed with fat-suppression techniques.9,14,15 In addition, MRI is useful for excluding other synovial lesions that may present with similar clinical features, such as pigmented villonodular synovitis, synovial chondromatosis, rheumatoid arthritis, and synovial hemangioma. 9
Although MRI is the first-line imaging modality for diagnosis of this lesion, sonography may be used initially for evaluation of chronic joint swelling. Because of this, clinicians should know the typical sonographic features of lipoma arborescens. Several reports have described the sonographic features of lipoma arborescens of the knee joint,16,17 which include uniformly hyperechoic synovium-based frond-like villous projections within synovial effusion. This would be quite similar to its macroscopic morphologic characteristics. 16 Only one previous report described the typical sonographic features of lipoma arborescens of the shoulder. 6 In the case presented, sonography revealed a fluid collection with thickening of the synovial membrane and hyperechoic villous proliferation located in the subdeltoid bursa. Based on these findings, additional examinations for further diagnosis were performed. Sonography is an inexpensive and noninvasive modality that can be performed as an initial diagnostic step in evaluating synovial lesions before applying more expensive modalities. In addition, it can be useful for the detection of chronic joint swelling and evaluating for recurrence after synovectomy.
Conclusion
This is a case of lipoma arborescens of the subdeltoid bursa, associated with a rotator cuff tear and treated with an arthroscopic procedure. Although MRI is the first-line imaging modality for diagnosis of this lesion, this case highlights that sonography may be used initially for evaluation of chronic joint swelling. In addition, sonography can be useful for detection of recurrence after synovectomy. Because of this, clinicians should know the typical sonographic features of lipoma arborescens.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.