
Abstract
The outbreak of a novel coronavirus (COVID-19) with symptoms that mimic bronchitis and other chest infections has created a need for quick diagnosis to prevent disease spread. Traditionally, computed tomography (CT) has been used as the primary method to identify infection and staging of the virus. While effective, repeated use of ionizing radiation, particularly in susceptible patient populations, can add risk as the disease is monitored through full recovery. Sonography of the chest may be a viable alternative for diagnosis and monitoring of COVID-19. In addition, new technology such as the remote robotic ultrasound equipment being used at Zhejiang Provincial People’s Hospital in Hangzhou, China, has the potential to facilitate sonographic evaluation with minimal disease exposure to the sonologist and to other patients by eliminating the need for patient transport to imaging facilities. Additional studies will need to be conducted to evaluate the effectiveness of sonography versus other imaging modalities in the diagnosis and treatment of COVID-19 and other novel diseases.
Background of COVID-19
The outbreak of a novel coronavirus (COVID-19) began within the city of Wuhan, in the province of Hubei, P.R. China. The virus quickly spread from person to person within the city and surrounding area, due in part to large gatherings in celebration of the Chinese Lunar New Year. At this time, it is believed that the spread of the virus began with the ingestion of food that originated in markets that also sold live animals. The travel of families between cities is likely a factor that expedited the spread of this deadly virus.
Origin of COVID-19 and Possible Zoonotic Origin
Current scientific evidence shows that COVID-19 originated within animals and evolved to spread within humans, classifying it as a bacterial zoonotic disease. The virus was initially designated as 2019-nCov, which denoted its novelty (n), disease type of coronavirus, (CoV), and its year of its discovery. 1 On February 11, 2020, the World Health Organization (WHO) officially named this new disease “COVID-19.” 2 The virus was first noted in December 2019 by scientist Leo Poon, a virologist at the School of Public Health at the University of Hong Kong. 3 The source was suspected to be either from seafood or cats, but new cases were soon confirmed in patients who were not exposed to either, 4 suggesting that person-to-person spread had occurred and was quickly accelerating the propagation of the virus in humans.5,6 Outbreaks of similar bacterial zoonotic epidemics have occurred previously, including severe acute respiratory syndrome (SARS-CoV) in 2003 and Middle East respiratory syndrome (MERS-CoV) in 2015.
Comparison of COVID-19 to SARS-CoV or MERS-CoV
Previous public health battles with other bacterial zoonotic diseases have helped to inform health care professionals on methods of handling COVID-19. The SARS-CoV epidemic, which resulted in 8098 confirmed cases and 774 fatalities, 1 was first identified in the Guangdong province of southern China. 3 SARS-CoV was a respiratory virus that also presented with diarrhea, fatigue, and kidney failure. 3 The MERS-CoV virus originated in Saudi Arabia and caused 2499 cases with 861 deaths. 1 The Centers for Disease Control and Prevention (CDC) determined that MERS-CoV had a much more fatal outcome than its predecessor, SARS-CoV. 3 While these epidemics are very concerning, the 2018 to 2019 influenza flu season within the United States (H1N1) resulted in 35.5 million cases and 34,200 deaths, many in the elderly and children. 7 That said, the novelty, rapid spread, and fatality rate of COVID-19 amplify the urgency of diagnosing and stopping its spread.
Public Health Emergency to Deal With Those Infected With COVID-19
This symposium will have only very formative statistics on the diagnosis of COVID-19, given the evolving nature of the epidemic. Many global health agencies have joined forces to assist the Chinese people in battling this virus, and as of January 30, 2020, the WHO has declared COVID-19 to be a “public health emergency of international concern.” 1 The worldwide incidence of possible COVID-19 cases jumped worldwide within the first few months to 91,320 cases spreading across dozens of countries and areas. 1 This pandemic has required global health agency cooperation and public health education as to the signs and symptoms of this developing disease.
Diagnosis by Identifying Patients With Acute Stages and Hospitalized Patients With Suspected COVID-19
Patients with this respiratory virus exhibit the following symptoms 8 :
Dyspnea
Fever
Cough
Myalgia
Fatigue
The recognized mode of transmission for COVID-19 is attributed to coming in contact with an infected patient’s body secretions. The coughing exhibited by these patients can put droplets into the air and promote airborne transmission, as can touching a common surface with secretions, such as after sneezing. 1 As of March 2020, there are no specific treatments for COVID-19, and the CDC is advising patients to take pain and fever medication, increase hydration, and get plenty of rest. 9 Health care workers are on the front lines of assessing these patients and must use universal precautions and personal protective equipment (PPE) to avoid contracting the virus. Vigorously washing hands for at least 20 seconds and keeping eyes, nose, and mouth covered are important ways to protect against contracting all types of viruses and bacteria.
Efforts to Diagnosis Patients Who Contracted COVID-19
Best practices for the diagnosis of COVID-19 are being developed by analyzing the response and results of efforts by Chinese scientists who are at the front lines of the disease. Physicians have been staffing local hospitals to treat those patients reporting with symptoms. Several nonessential medical service departments have canceled appointments to allow for volunteering in Wuhan, where a new 1000-bed hospital was recently constructed but staffing was not sufficient to handle the outbreak of the epidemic. 1 Many physicians and nurses volunteered from other provincial hospitals to staff the facility and assist in the diagnosis of these patients. The experiences that these brave health care workers encountered help to inform the rest of the global community in the development of diagnostic best practices.
Use of Computed Tomography of the Chest to Identify Infection and Staging of the Virus
The presenting symptoms of many patients are dyspnea and violent coughing, which can also mimic bronchitis. To better determine whether the patient has contracted a viral respiratory infection, such as COVID-19, radiography of the chest or computed tomography (CT) of the thorax is important. The American College of Radiology (ACR) has published criteria on the most appropriate diagnostic tool for documenting pathology in the lungs. For patients who have an acute respiratory illness with a positive examination, abnormal vital signs, or other risk factors, the most appropriate initial imaging is radiography of the chest (usually appropriate). This may be followed by sonography of the chest (may be appropriate). 10 Interestingly, after an initial chest radiograph, there is some disagreement as to the next best imaging choice, as a chest CT with intravenous (IV) contrast is also listed as “may be appropriate.” 11 As part of the lessons learned, chest CT findings are being provided on patients who were found to have coronal viral infections. Here is a formative list of some of the CT imaging appearances12,13:
Ground-glass opacity (86% of those patients imaged)
Bilateral distribution (76% of those patients imaged)
Peripheral distribution (33% of those patients imaged)
Consolidation (29% of those patients imaged)
Pleural effusion (0% of those patients imaged)
Lymphadenopathy (0% of those patients imaged)
This early CT information that has been provided is based on 21 patients with diagnosed COVID-19, but it should be noted that some of these patients also had normal imaging at their initial intake. 12 In the meantime, recommendations are being made that for patients who exhibit symptoms and have a CT with ground-glass opacity, the diagnosis of COVID-19 should be considered. 14 It is also important to remember that a normal chest CT does not exclude the potential for early stages of COVID-19. 14 The concern in Wuhan was the need to use of ionizing radiation on such a large scale, as well as other provinces across P.R. China. Given that the ACR did deem sonography of the chest as “usually appropriate,” it may be a suitable alternative, particularly for infected women and children. 10
Use of Lung Sonography of the Chest to Further Define the Area of the Lung Infected
The use of sonography as a diagnostic tool for assessing a respiratory infection may not seem to be the best diagnostic choice in the United States, but recent studies have given added evidence to its use. In a study by Elmahalawy et al., 15 sonography of chest was compared to the results of bedside radiography and CT for detecting pathology in critically ill patients. The study involved the imaging results of 130 mechanically ventilated and nonventilated patients in an intensive care unit (ICU). They found that to detect pneumonia, sonography of the chest demonstrated 93% sensitivity, 95% specificity, a positive predictive value of 98%, and a negative predictive value of 87%. 15 Sonography to detect pleural effusion has a similar predictive value and therefore was suggested as a best practice for their medical practice. 15 Unfortunately, the use of portable radiography and CT equipment was not described in the methods section, so it was difficult to determine whether the age or sophistication of the machines used could play a factor in the comparison. Likewise, the sonography equipment was also not described, other than a handheld micro convex transducer, 5 to 9 MHz. 15 These results would have been better replicated had the methodology been more clearly provided. An additional recent study by Ellington et al. 16 focused on the role that chest sonography could play in the diagnosis of respiratory pathology in pediatrics. In their study, 453 children were enrolled, and of those, 133 had pneumonia, 103 had asthma with bronchitis, and 143 had upper respiratory tract infections. This comparative study, much like the previous one, demonstrated that sonography of the pediatric chest, for consolidation of infection, had a sensitivity of 80%, 100% specificity, and an area under the prediction curve of 0.94. 16 These values increased when the sonogram was paired up with the results of a chest radiograph. 16 Thankfully, this study provided a much more descriptive methods section and identified its use of a Sonosite MicroMaxx (FujiFilm SonoSite, Inc. Bothel, WA) and a 13-6 MHz transducer, but the radiographic equipment was again not specified. This lack of equipment specificity makes the results hard to translate on a global scale to provide trustworthy recommendations. This also was the finding of a systematic review and meta-analysis of literature on the topic of lung sonography to diagnosis pneumonia in children. The authors reviewed 1042 articles, and of those, 76 were determined to be eligible for the review. 17 This systematic review and meta-analysis had the potential to provide the highest level of evidence for practitioners on the use of chest sonography for pediatric respiratory disease. Unfortunately, the lack of detail across all the articles reviewed made it difficult to determine if similar results could be obtained. The authors were only able to recommend that more rigorous methods must be used when obtaining sonography of the lungs so that the findings could be more easily translated to clinical practice. 17
Surveillance of the Stage of the Infection by Repeated Lung Sonography
The literature is not replete with recommendations for the use of chest sonography as a diagnostic surveillance tool. A case study of monitoring the recovery of an adult man with influenza H1N1 was published and was effective in this particular case, even though the patient was a smoker. 18 Upon presenting to the emergency department, he underwent a CT chest that demonstrated multiple bilateral areas of increased lung opacity. 18 In this case, the patient was intubated and was mechanically ventilated to restore his oxygen saturation. Sonography of the chest to monitor his treatment of the inflection was repeated three times, and the restoration of pleural gliding was used as a diagnostic sign of therapeutic success. 18 A similar cohort case study examined critically ill patients who contracted avian influenza A (H7N9) infection and were monitored with sonography. 19 These patients were followed in a serial manner with sonograms, and the results were correlated with their clinical findings and chest radiography. Besides documenting subpleural consolidations, the sonograms revealed numerous, confluent, or coalescing B-lines leading to opacities that corresponded to pleural thickening. 19 These low levels of evidence underscore the ongoing need to provide more evidence of the effectiveness of using sonography of the lung to monitor patient outcomes.
Lung Sonography to Monitor Treatment Effects
As of March 2020, there was indication that scientists at the Peter Doherty Institute of Infection and Immunity in Australia have been able to grow the virus in cell cultures. 1 This breakthrough lays the groundwork for developing and testing a vaccine. A Hong Kong University professor, Yuen Kwok-yung, reportedly has developed a potential vaccine, but it has not yet undergone basic science testing or clinical trial testing. 1 In preparation for a possible vaccine trial, we must also prepare to monitor its effect and dosing for children and the elderly. Sonography has an important role to play as physicians monitor treatment effects, especially considering the lasting effects to the lung tissue as a result of COVID-19. It has already been hypothesized that imaging of the long-term effects of this bacterial zoonotic disease may resemble lung tissue changes that resemble an acute lung injury. 14
People’s Hospital Remote Use of Lung Sonography to Detect Early Stages of COVID-19
In June 2019, Zhejiang Provincial People’s Hospital, China Telecom, and Huawei built the 5G AI Medical Innovative Lab in Hangzhou, China, which includes a robotic ultrasound system. This has allowed for the remote diagnosis of patients using chest sonography provided in hospitals in Zhejiang province and in other facilities. Chengzhong Peng, MD, and Ruizhong Ye, MD, completed lung sonograms on two suspected patients with the use of the remote robotic ultrasound system. These were the first successful remote sonographic examinations on suspected patients with COVID-19 during the initial outbreak in China. 20 They began by controlling a robotic arm 40 miles away at a hospital in Tongxiang, Zhejiang. The patient in that facility had the ultrasound transducer applied to the chest and was directed remotely. Instantaneously, chest sonograms were sent to Peng or Ye’s computer in Hangzhou. Within minutes, the sonographic report and diagnosis were sent back to the patient’s attending doctors in the hospital at Tongxiang. This is an example of how a highly sophisticated, remote sonogram of the chest can provide critical diagnosis information and assist in developing patient treatment plans.
Equipment Type for Sonographic Assessment of the Lungs of Patients With Suspected COVID-19
The remote robotic ultrasound system used was the MGIUS-R3 system, which was developed by MGI Tech Co., Ltd. The MGIUS-R3 is the leading technology in remote sonographic diagnosis, which consists of two components that are connected through the Internet, uniting the sonologist and the hospitalized patient. The sonologist conducts the patient’s sonogram through use of the robotic arm located at the patient’s bedside (see Figure 1). The sonographic examination is directed by an assistant operating the mock probe in the host hospital (see Figure 2). Due to the high volume of sonographic images and dynamic clips taken during the examination, the MGIUS-R3 requires an extremely high-quality Internet connection. For example, it may transport 2 GB of images during one chest sonographic examination. The 5G Internet with high speed, stability, and low latency provides a stable, secure, and fast Internet for the MGIUS-R3 system. 20
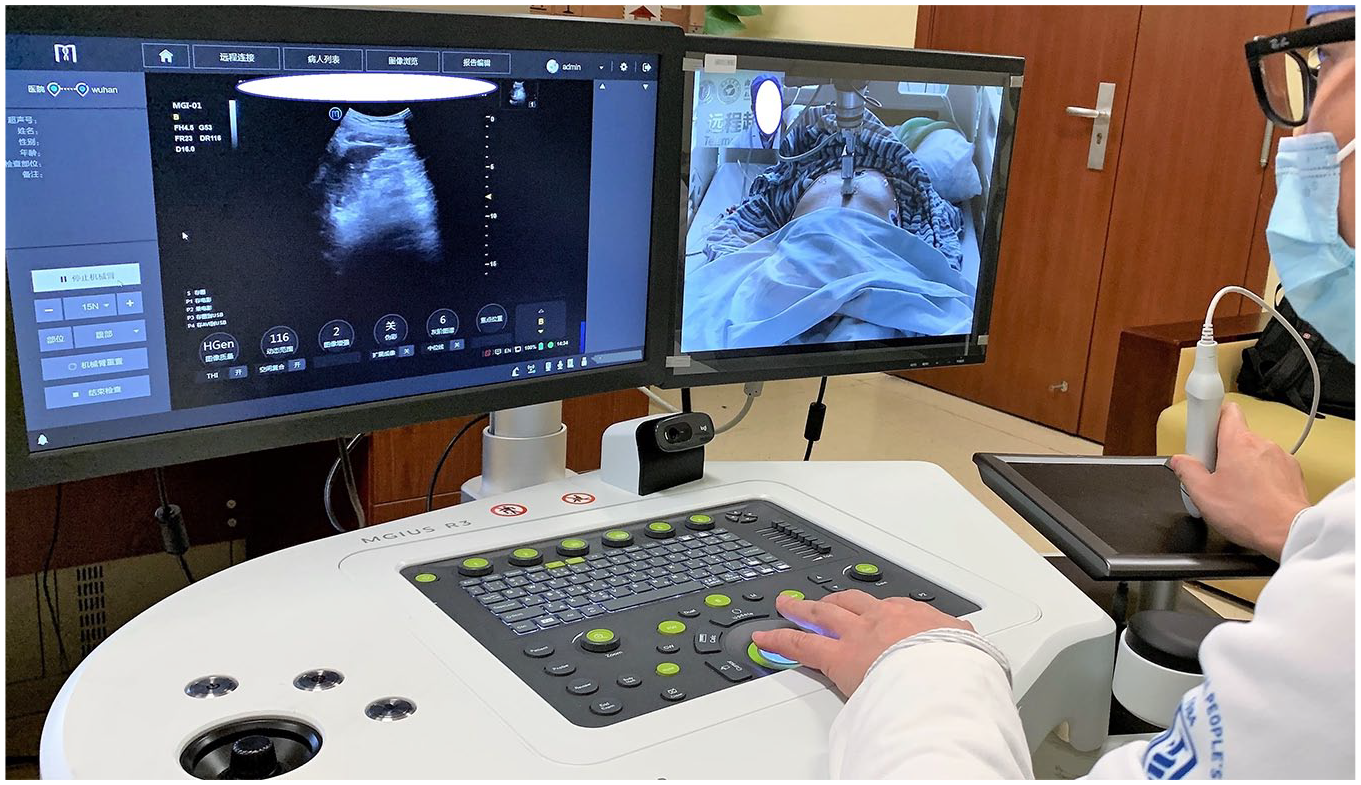
Sonologist using the MGIUS-R3 system to conduct an actual patient sonogram to determine whether suspected COVID-19 has produced pathologic changes in the lung tissue.

Application of the ultrasound equipment at the bedside of a local hospital. An attendant was needed to make fine adjustments to the robotic armature and move the patient.
Sonographic Appearance of COVID-19 as the Replacement or Adjunct to CT
Chest sonography has great clinical potential in the diagnosis and surveillance of the current COVID-19 epidemic. Repeated ionizing radiation exposure through multiple chest CTs increases exposure for patients, particularly adding risk and difficulty to those in the ICU due to their limited mobility and fragility. There are additional concerns in the use of ionizing radiation on pediatric patients and pregnant women. The use of chest sonography should be considered a possible replacement or supplement to CT in the diagnosis of COVID-19, as well as monitoring treatment and recovery from this bacterial zoonotic disease.
Formative Assessment of the Feasibility and Reliability of Lung Sonography in the Diagnosis and Surveillance of COVID-19
Drs. Peng and Ye sonographically examined two suspected patients with COVID-19, using the MGIUS-R3 remote robotic system. From their experiences, the MGIUS-R3 system was user-friendly and provided high-resolution diagnostic images. Furthermore, the remote robotic ultrasound system made it possible to sonographically examine patients without increasing the risk to the physician. The technology also has the potential to keep the patient isolated and minimize patients moving around the hospital for imaging (CT or magnetic resonance imaging), reducing the chances of patient-to-patient or patient-to-provider transmission. That said, the remote ultrasound system does have limitations. Peng and Ye’s ongoing research found that an assistant is needed to adjust the robotic arm to the targeted location of the lung and also to adjust particular patient positions. Peng and Ye continue to investigate the feasibility and reliability of the MGIUS-R3 system, as the current outbreak of COVID-19 continues. Currently, the Chinese Society of Sonography et al. has recommended a road map or diagnostic algorithm for the diagnosis of COVID-19 (Figure 3). 21
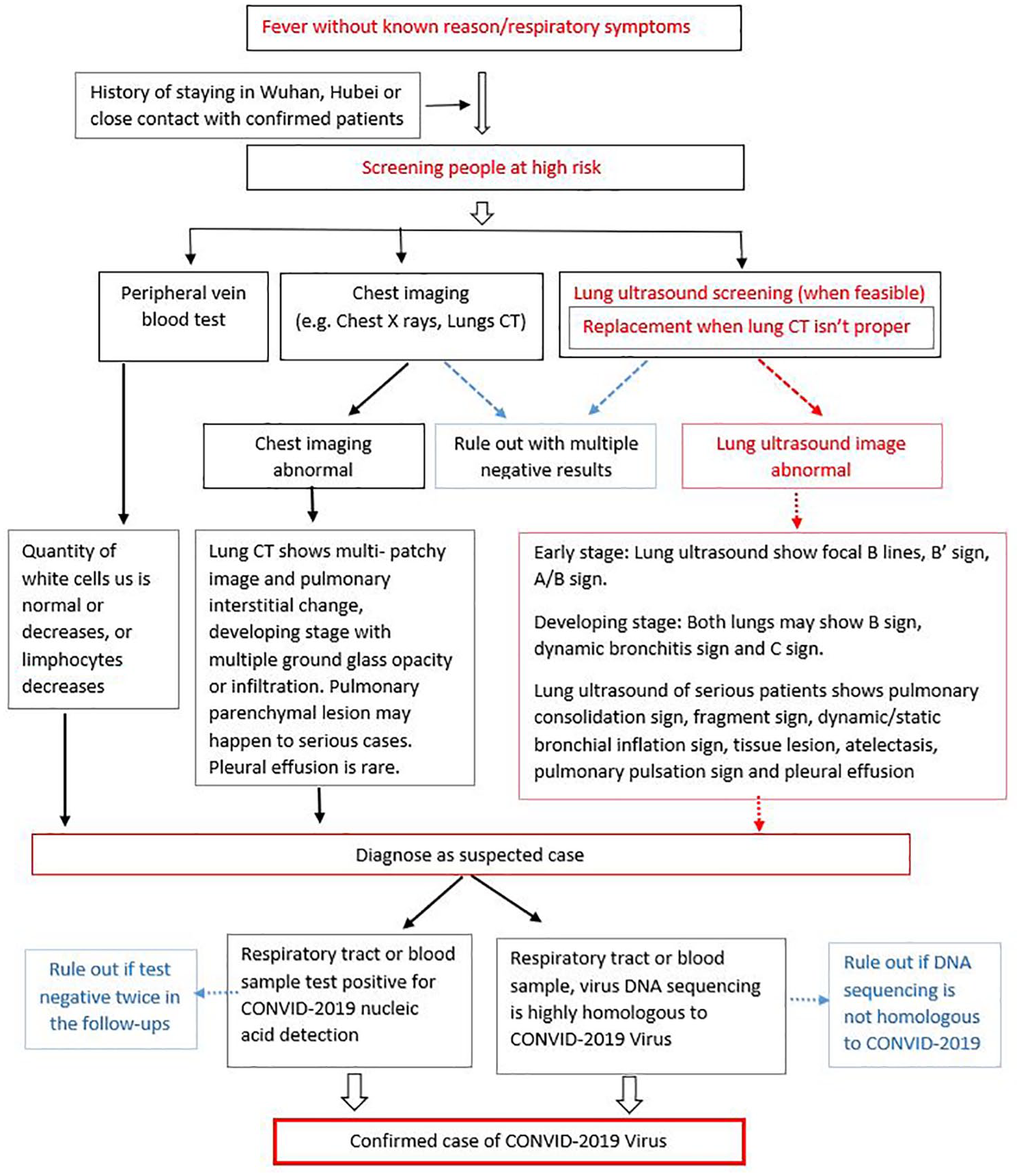
The Chinese Society of Sonography et al. has provided a diagnostic algorithm to be used in conducting a thorough diagnostic assessment of patients suspected of having a lung infection. This has been somewhat adapted in dealing with the volume of patients reporting with symptoms of COVID-19.
Summary and Next Diagnostic Steps for Combating COVID-19
This article provides an account of early diagnostic successes of sonologists in battling COVID-19 in P.R. China. Their anecdotal evidence and early results of using chest sonography to evaluate the lungs are timely and allow for more clinical evidence to be built. The use of sonography to evaluate the lungs, with either handheld ultrasound equipment or remote automation, has potential diagnostic advantages. There is great potential to reduce ionizing radiation exposure to patients while limiting the spread of disease through patient transport and provider intervention. At the same time, the use of chest sonography, both handheld imaging and remote automation, has diagnostic disadvantages. It does require that an assistant, with PPE, apply the transducer to the patient and also position him or her for optimum imaging. Given the low level of evidence, the sensitivity and specificity of the sonographic imaging results would need to be carefully monitored.
Although our colleagues in China are providing important formative assessments of patients suspected of having COVID-19, more diagnostic evidence will be needed to raise the appropriateness criteria for clinicians. Nevertheless, the lessons learned and low levels of diagnostic evidence provided by our colleagues open a new diagnostic application for sonography. Chest sonography and the diagnostic evaluation of the lungs have the potential to expedite and treat a wide variety of lung infections.
Footnotes
Acknowledgements
The authors acknowledge the hard work and continued bravery of the health care professionals battling COVID-19 and caring for patients with this illness.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.