
Abstract
Introduction
Coronavirus disease 2019 (COVID-19), which was first detected in Wuhan, China, in late December 2019, caused major impacts on the lifestyle and physical and mental health status of faculty, staff, university students, and the general population.1, 2 The negative impacts of the COVID-19 health crisis on the daily lives of people working in educational centers are evident due to the changes observed in the levels and frequency of physical activity, quality and duration of sleep, food preparation and consumption, and body weight status.3–5 On the other hand, previous studies have shown a significant deterioration in glucose control during the pandemic. 6 These changes increase the risk of non-communicable diseases, such as type 2 diabetes mellitus, cardiovascular disease, and obesity; which, in turn, could increase the risk of mortality from COVID-19. 5 Therefore, effective guidance on the benefits of a healthy lifestyle is needed in university staff and the general population for the prevention of non-communicable diseases.
In fact, non-communicable diseases are common throughout the world and, in most cases, are due to an unhealthy lifestyle. 7 In particular, the increased consumption of high-calorie foods rich in saturated fats, free sugars, and low in fiber is one of the main causes of these diseases. 7 Likewise, social isolation due to the state of health emergency caused by COVID-19 and promoted by governments, has forced university teachers and staff to work from home, which has led to changes in lifestyle directly related to sedentary lifestyles, favoring excess body weight. 8 It is also worth mentioning that the transition from face-to-face to online work, added to the domestic burden, constitutes a challenge for most university workers, who had to improvise work spaces within their homes. 9
University personnel represent a vulnerable group to the development of various lifestyle-related diseases and the negative consequences of COVID-19. However, telehealth technology, considered the provision of medical care and clinical information by health professionals, can represent an effective, attractive, and rapid option for promotion and prevention through education about the benefits of leading a healthy lifestyle. 10 Especially in times of quarantine, telehealth can become a basic need for the university community and the general population. 11 This is possibly due to the fact that it allows real-time communication between a professional sharing valuable information on healthcare-related topics.
The use of telehealth technology has been previously described in the healthy lifestyle literature. 12 Some studies have demonstrated the positive impact of telehealth-based intervention programs on body weight control. 13 For example, a videoconference-based health coaching intervention study in a group of 30 adults with high body mass index (BMI) led to favorable changes in body weight, physical activity, and metabolic markers. 14 Similarly, other studies have evidenced the efficacy of telehealth-based lifestyle interventions in pre-diabetic participants. 15 While telehealth had previously been established as an effective technique associated with positive clinical outcomes through lifestyle changes, 16 however, the ongoing health crisis triggered a series of regulatory changes, which facilitated rapid widespread adoption. 17 In fact, during the COVID-19 pandemic, telehealth interventions have been developed that allowed patients to gain new experiences in the way they care for their health and decrease the costs of face-to-face care. 18
An intervention using telehealth technology with university teachers significantly improved knowledge levels on topics related to healthy eating and BMI. 13 Similarly, findings from a survey conducted during the pandemic of participants in other occupations highlight associations between digital literacy and healthy eating behaviors and health-related quality of life. 19 Therefore, telehealth represents an effective strategy to improve health and promote behavior change during times of health crisis, such as the COVID-19 pandemic.
However, there are few telehealth-based interventions carried out to improve lifestyles, prevent diabetes and obesity during the COVID-19 pandemic in university staff. Telehealth-based interventions need to be developed, as they could be considered as one of the alternatives to ensure timely care in the midst of the ongoing health emergency. Therefore, the objective of this study was to demonstrate how a telehealth program improves lifestyle, BMI, and glucose concentration in the staff of a private university during the COVID-19 pandemic.
Materials and methods
Study design and population
The study used a prospective and pre-experimental design model. The study protocol was approved by the Research Ethics Committee of the Universidad Peruana Unión (approval number: 2021-CE-EPG-000042). Prior to the implementation of this telehealth-based education program “Healthily”, distributed in 18 educational sessions over 18 weeks, informed consent was obtained from all participants. The study was conducted in accordance with the ethical criteria established by the 1975 Declaration of Helsinki and its subsequent modifications (Figure 1).

Study design of telehealth-based interventions on lifestyle, body mass index, and glucose concentration in university staff.
A preliminary survey was conducted regarding practices and beliefs about healthy lifestyles. Moreover, glucose concentration and anthropometric measurements, such as height and weight, were also evaluated; subsequently, BMI was calculated.
No sampling was performed because the population was small; all participants who agreed to participate and those who met the selection criteria were included. The sample size was calculated using the G*Power software program (3.1.9.7) considering a long effect size prediction (d = 0.8), 1-β = 0.93 and Type I error (α) of 0.05. Taking into account the prediction of a low to medium effect size (d = 0.4), the total sample size was (N) = 76. Taking into account the possibility of attrition of the participants during the follow-up of the program, 100 workers were considered to participate, however, 78 employees completed the study, and 22 employees were lost during the follow-up during the 18 weeks in the months of August and December 2021. The participants were staff from a private university located in the city of Tarapoto, Peru.
Implementation and development of the “healthily” program
After authorization to conduct the study, a virtual meeting was held with the participants through the Zoom Video Communications virtual platform to explain the objective of the study. Likewise, the election of the “Health Promoters” was carried out, who were responsible for leading, encouraging, and motivating the 10 “Healthy Groups” that were subsequently created. It should be noted that the instant messaging platform WhatsApp Messenger was used to form the groups, which were identified by the names of some biblical characters, such as “Paul,” “Gideon,” “Elijah,” among others. Afterwards, the participants were invited to the Medical Center of the Universidad Peruana Unión to apply the lifestyle practices and beliefs questionnaire, perform anthropometric evaluations and measure glucose concentration. These were the initial evaluations.
Two weeks after the initial assessments, participants were invited to a first training entitled: “Importance of lifestyle in health”, which was given for 35 min through the Zoom virtual platform by a physician specialized in lifestyle medicine. After the presentation, the participants asked questions to clarify their doubts about the content of the training. At the end of the initial program, all members received an encouraging message from the study's principal researcher and the “Health Promoters.”
Finally, once the program training was completed (at the end of 18 weeks), the participants were invited to come back to the Medical Center to apply the lifestyle practices and beliefs questionnaire, measure glucose concentration, weight, and height.
Training resources and tools
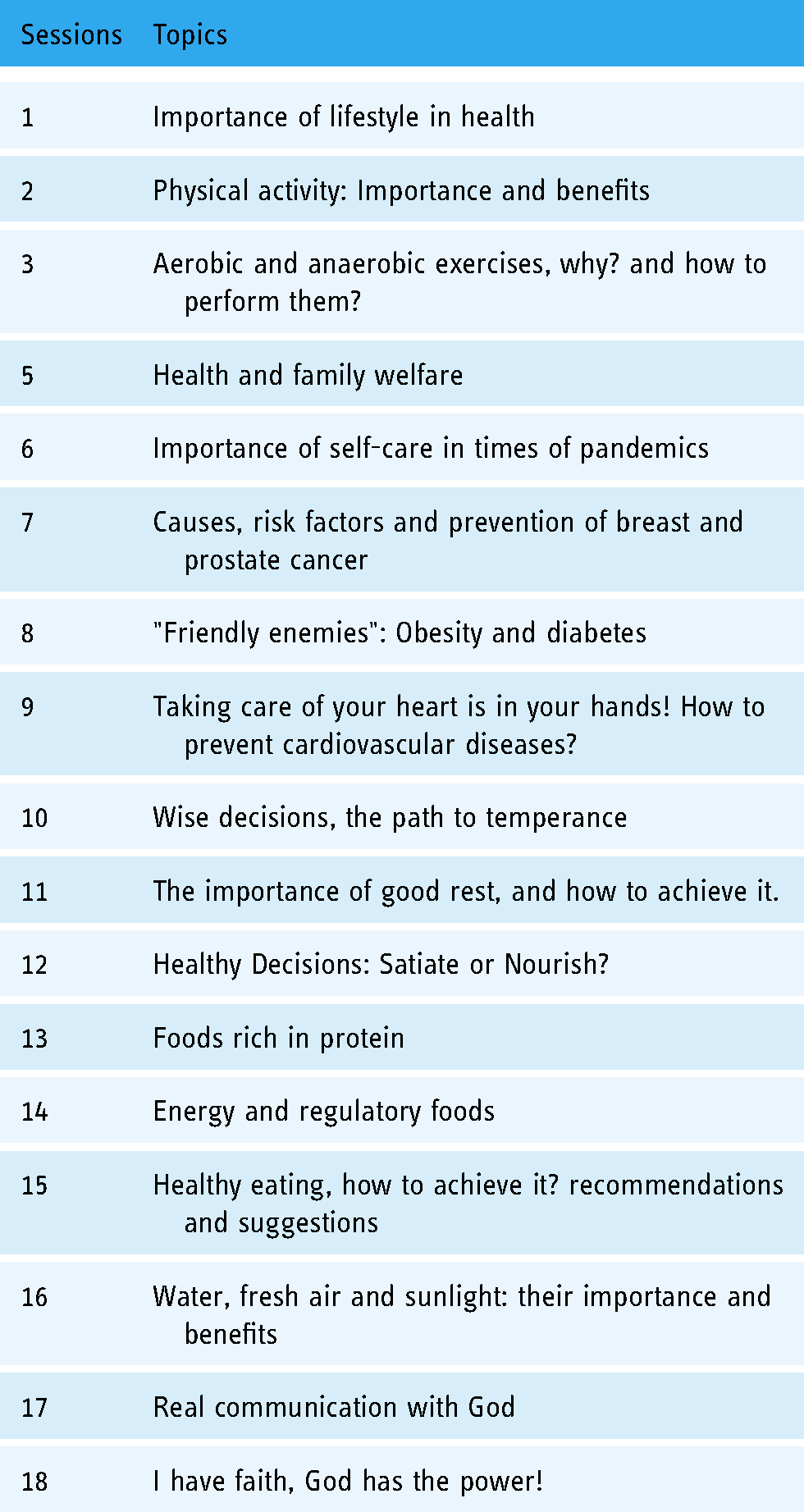
In advance, different specialists in topics related to health promotion, healthy lifestyles, and disease prevention were contacted for the development of the training described in Table 1. The topics were delivered using Microsoft PowerPoint and other learning tools, such as the free Kahoot platform and Google Forms for feedback.
Telehealth-based education program for university personnel.
Moreover, a web space (https://sites.google.com/upeu.edu.pe/healthily2021/inicio?authuser=0) was created using Google Sites, an online application offered by Google, where participants could view the entire program schedule, including information on speakers, weekly experiences, books, and audiovisual materials related to healthy lifestyles. In addition, recordings of the training sessions were made available for later viewing.
Sharing experiences
During the 18 weeks that the program lasted, a poster containing a motivational health message was shared weekly with the members of each group through the “Health Promoters” and WhatsApp Messenger, encouraging the members to share their experiences in relation to the training developed. Members voluntarily shared evidence (photos and videos) of their healthy experiences through social networks, such as WhatsApp Messenger and Facebook. Likewise, these healthy experiences were projected weekly during the training to encourage the participants.
Motivational strategy
All participants were able to view evidence of the experiences of the members of each group. Furthermore, the groups were rewarded according to the score achieved. The scores were represented as follows: a score of 100 meant that “all participants in the group (100%) submitted their experience”; 80 points meant that 80% of the participants submitted their experience; and a group with less than 80% participation received 60 points. At the end of the 18 weeks of the program, the scores were added up and the three groups with the highest scores received a dumbbell kit to motivate them to engage in physical activity.
Lifestyle beliefs and practices questionnaire
Lifestyle practices and beliefs were measured by means of a questionnaire validated in the Peruvian population. 20 This questionnaire consists of 42 items covering dimensions such as physical activity and sports, recreation, self-care, eating habits, sleep, and trust in God. It also contains a Likert-type scale where never = 1, sometimes = 2, and always = 3. The instrument is divided into two categories with a total score of 126; where a score of 41–105 corresponds to an unhealthy lifestyle, while scores ranging from 106 to 126 indicate a healthy lifestyle. The instrument proved to be reliable according to Cronbach's alpha score (α = 0.8); similarly, the reliability of the questionnaire was observed according to Aiken's V with a score = 1.0. 20
Measurement of anthropometric data
Anthropometric data, such as weight and height, were collected. For weight assessment, a SECA 700 mechanical column scale with a capacity of 220 kg and a measuring range of 60 to 200 cm (SECA®, Hamburg, Germany) was used. Participants were instructed to remove excess clothing, shoes, and objects, such as wallets, watches, among others. In addition, BMI was calculated using the Quetelet index reference and classified according to the technical guide for the anthropometric assessment of adults of the Peruvian Ministry of Health 21 ; underweight BMI < 18.5; normal weight: BMI ≥ 18.5–24.9; overweight: BMI 25–29.9; obesity: BMI > 30 kg/m2.
Glucose concentration measurement
Data on glucose concentration were collected using the Exactive Vital UVP315 glucometer with its respective lancets and test strips. Likewise, prior to sample collection, the participant was asked to go to the health center during the first two hours of the morning, after 12 h of fasting. As part of the extraction process, the puncture site was disinfected for the extraction of the blood drop. The criteria of the Clinical Practice Guidelines for the Diagnosis, Treatment, and Control of type 2 diabetes mellitus were used as a reference. 22 Glucose concentration >126 mg/dL was considered as hyperglycemia.
Statistical analysis
Previously, the normality of the sample was tested using the Kolmogorov Smirnov statistical test. The descriptive analysis of the data, such as age, sex, marital status, among others, was performed using mean (M) and standard deviation (SD), absolute frequency and percentages, and the skewness and kurtosis coefficients to analyze the behavior of the variables. Differences in lifestyle practices and belief scores, BMI, and glucose concentration before and after the program were performed using the Wilcoxon nonparametric statistical test. The data were processed and analyzed using statistical packages through the free software R 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org) and SPSS, version 27 (SPSS Inc., Chicago, IL, USA). P values (p-value) less than 0.05 were considered as statistical significance.
Results
The sociodemographic characteristics of the program participants are described in Table 2. The mean age of the participants was 36.47 ± 10.79 (age range: 24 years–62 years). A higher proportion of male participants was observed (65.4%), and 73.1% were married. The intervention program targeted workers coming from the coast (26.9%), highlands (25.6%), and Amazonia (47.4%) of Peru.
Sociodemographic characteristics of telehealth program participants (n = 78).

Note: M: mean; SD: standard deviation.
Table 3 describes the average scores of the participants on lifestyle beliefs and practices, BMI, and glucose variables before and after the application of the intervention program. After application, it was observed that lifestyle practices and beliefs scores improved significantly by 3 points (93.33 ± 9.44 vs. 96.23 ± 9.32, p < 0.01), although this value translates to an unhealthy lifestyle. Regarding BMI, there was a significant decrease in the mean after applying for the program (from 25.23 ± 3.08 to 24.98 ± 2.98, p < 0.05). Finally, mean glucose level scores were reduced after the program compared to the baseline measurement (from 98.35 ± 6.70 to 97.45 ± 5.61), these differences were also significant (p < 0.01).
Mean, standard deviation, distribution, difference of nonparametric measures and effect size.

Note: M: Mean; SD: standard deviation; S: skewness coefficient; K: kurtosis coefficient, MD: mean difference; p: probability of error; E. Size: effect size. * For the Wilcoxon test, the effect size is given by the paired Rank-Biserial correlation and through the Hodges–Lehmann estimator.
Figures 2, 3, and 4 show the effect of the telehealth intervention program on lifestyle practices and beliefs, BMI, and glucose concentration, respectively. In relation to the time of application of the program (before and after), significant variations are observed in the scores of lifestyle practices and beliefs (p < 0.01), BMI (p < 0.05), and glucose concentration (p < 0.01) before and after the intervention program.

Lifestyle practices and beliefs before and after the telehealth intervention program. Note: t Student (77) = −6.754, p = 2.416e-09, g Hedges = − 0.757, CI95% [−1.012, −0.509], npairs = 78.
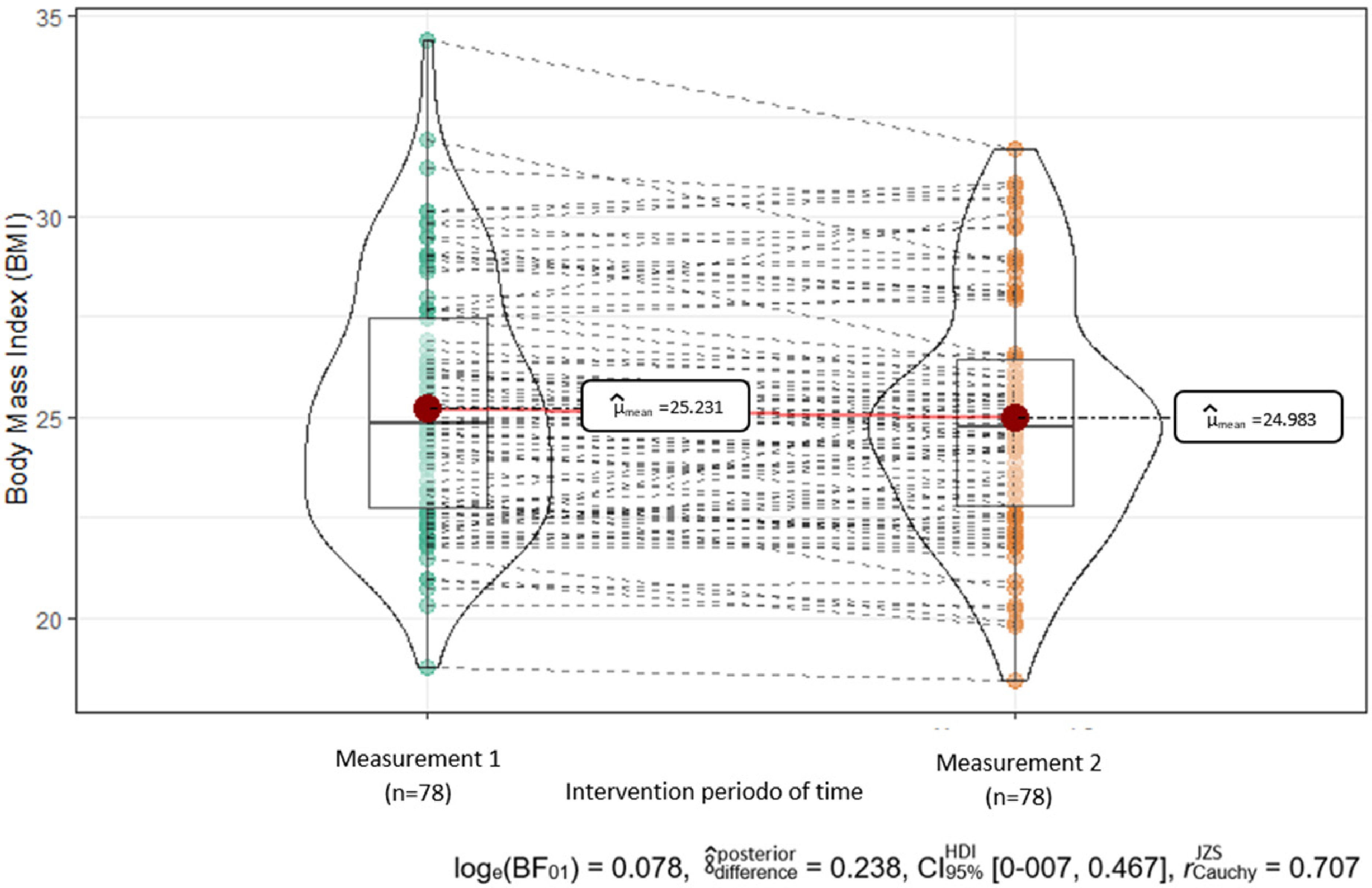
Body mass index (BMI) before and after the telehealth intervention program. Note: t Student (77) = 2.063, p = 0.042, g Hedges = −0.231, CI95% [0.008, 0.456], npairs = 78.

Glucose concentration levels before and after the telehealth intervention program. Note: VWilcoxon = 1777.5000, p = 0.004, Rank-Biserial = 0.391, CI95% [0.156, 0.584], npairs = 78.
Discussion
Telehealth intervention programs play an important role in promoting a healthy lifestyle among university staff, especially considering the health situation caused by the COVID-19 pandemic, where most university workers are forced to perform their work remotely, which, in turn, can lead to unhealthy behaviors, such as inadequate food consumption, physical inactivity, with notable consequences on BMI and glucose concentrations.8, 23 The current study aimed to demonstrate how a telehealth program improves lifestyle, BMI, and glucose concentration in university staff during the COVID-19 pandemic. The following main results have been found: (a) The participants' lifestyle scores improved significantly after the application of the program, although they did not reach a healthy lifestyle score (106–126 points), (b) in relation to BMI, the mean was significantly reduced after the intervention; finally, (c) it was observed that the mean glucose concentration was lower after the program compared to the initial values.
One of the relevant results of the current study is that an increase in lifestyle practices and beliefs scores was observed after the application of the program, although participants did not report an adequate lifestyle score. A healthy lifestyle encompasses healthy behaviors such as healthy eating, adequate rest, regular physical activity, among others. 24 In particular, healthy eating plays an essential role in disease prevention and health maintenance. There have always been calls for studies involving behavioral interventions to modify and improve eating habits. 25 In fact, a study using web-based and telehealth tools that included a dietary application for smartphones reported positive changes in eating habits. 26 Similarly, another study has reported that telehealth interventions can positively impact diet quality by encouraging adequate consumption of fruits, vegetables, and adequate intake of essential macronutrients and micronutrients. 27 Studies demonstrate the effectiveness of intervention programs in improving eating habits, one of the main components of lifestyle.25–27
Other dimensions of lifestyle, such as physical activity and adequate sleep were improved after telehealth-based interventions in the general population. 28 In fact, studies in other population groups have shown positive changes in physical activity and sleep quality in adults following telehealth interventions.29, 30 The use of telehealth technology-based interventions is feasible and effective, and may be associated with positive outcomes in promoting a healthy lifestyle in teachers, students, and university staff, as well as the general population. 31
Moreover, the findings of the current study have shown a significant decrease in the mean BMI of the participants after the application of the program, placing us within the normal range established by the World Health Organization. 32 These findings are similar to what was found in a study in which BMI scores were significantly decreased after healthy eating topics were taught for 18 weeks. 13 Moreover, a similar pattern was observed in other studies conducted in the general population reporting positive effects of telehealth interventions on BMI.31, 33 Our findings suggest that telehealth-based follow-up may promote healthy lifestyle and weight control in university staff during the COVID-19 pandemic. This is particularly important considering that university personnel were forced to carry out their academic and administrative work from home, which can lead to a sedentary lifestyle, favoring excess body weight. 8 In addition, obesity is a challenge for the university community and could be due to different factors, such as access to hypercaloric foods available in university canteens, and lack of physical activity linked to a possible work overload.13, 34, 35 Therefore, future studies should consider telehealth-based interventions aimed at proper workload management and adequate use of leisure time to prevent body weight gain.
Diabetes represents one of the fastest growing health challenges during the last two decades 36 and the optimization of glycemic control is essential to delay its onset and decrease the progression of the associated chronic complications. 37 The COVID-19 pandemic has not only had a negative impact on people's weight status but also on metabolic markers, such as glucose. 23 Another important finding of the current study is that the mean glucose level scores were significantly reduced after the program from the baseline measurement. Telehealth-based lifestyle interventions are also effective in controlling glucose concentration. One possible justification is that our intervention focused on improving behaviors such as diet, physical activity, and aspects such as BMI, which, in turn, could favor these results. Previous studies have reported the efficacy of telehealth-based lifestyle interventions in pre-diabetic participants. 15 Additionally, a study conducted on diabetic patients during the COVID-19 pandemic identified that glycosylated hemoglobin values were significantly lower after education compared to baseline values at education. 38
The use of telehealth technology for behavior modification can become a tool to improve lifestyles, which could be a potential solution to promote healthy body weight and adequate glucose levels. 14 This is essential for university staff because they generally report obesity and poor sleep quality, inadequate nutrition, and sedentary lifestyles.39–41 In fact, the university is one of the most important settings that affect the eating habits and physical and mental well-being of faculty, staff, and students.42, 43 In addition, it is reported that teachers perform academic work in their free time, 35 this could lead to high levels of work-related stress, which in turn negatively impacts eating habits and physical activity. 44
Therefore, the use of motivation as part of the components of telehealth-based interventions is crucial for improving lifestyles to achieve a significant decrease in the risk of non-communicable diseases and avoid absenteeism of university faculty and staff due to medical conditions related to unhealthy behaviors. 45 In the current study, the researchers implemented a motivational component that included the creation of “Healthy Groups” led by “Health Promoters,” which could justify the results of the program by favoring its execution in a dynamic and fun way. This type of intervention can be effective and strategic in promoting the adoption of a healthy lifestyle.
Limitations
The study has some limitations and the authors are aware of this. First, in the study, a control group was not considered. In addition, the study sample was homogeneous in the sense that it was composed solely of university personnel from a single university in a specific region of Peru. Therefore, future studies should replicate our findings in diversified samples and randomly assign personnel to a control and intervention group. Similarly, it is considered a limitation that there was a high proportion of men in the study, which could be due in part to the overrepresentation of men and gender equality in university work. Finally, the lack of a longitudinal study that could verify that our findings could be sustained over time represents another limitation, although the study proved to be effective after 18 weeks of intervention.
Conclusion
In this study, we found that a telehealth-based education program was effective on lifestyle practices and beliefs, BMI, and glucose levels in a group of university staff during the COVID-19 pandemic. Although participants did not report an adequate lifestyle score; however, these findings could illustrate the willingness of university staff to collaborate with intervention programs by opting for healthy habits that can have a positive impact on the prevention of non-communicable diseases, such as obesity and diabetes.
Footnotes
Acknowledgments
The authors would like to thank all the participants in the study for their collaboration.
Contributorship
NMM and JS designed the study. NMM, JS, and YECM developed and shared the topics with the participants. AJCV and RAV wrote the first draft of the manuscript. JTC, SASA contributed to the study design, in addition, they co-authored the protocol. JAST and CCMG participated in data collection and reviewed the first draft. JS, YECM, and CCMG analyzed the data and reviewed several versions of the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Universidad Peruana Unión, Campus Tarapoto, Peru, through the Programa Maestro Plan de Desarrollo Salud Bienestar Universitario, (Grant 041- 2022/SA). However, the content of the study is the sole responsibility of the authors and does not necessarily represent the official opinion of Universidad Peruana Unión.
Ethical approval
The study protocol was approved by the Research Ethics Committee of the Universidad Peruana Unión (approval number: 2021-CE-EPG-000042).
Informed consent
Informed consent was obtained from all participants.
Guarantor
JS