
Abstract
Objective:
Critical thinking is an important skill that sonographers must develop beginning in educational programs and into professional practice. Critical thinking requires students to reflect on information, use judgment skills, and engage in higher levels of thinking, including analysis, interpretation, inference, evaluation, and explanation, to formulate reliable decisions.
Methods:
Current research related to critical thinking has focused on medicine, nursing, physical therapy, pharmacy, and dental programs, but there has been no description of assessing sonography students. The Dreyfus model has been used as a framework to describe acquired skills that reflects students’ progress from novice to expert clinicians. This model illustrates specific cognitive abilities that students develop as they advance in education.
Results:
This review of the literature describes critical thinking skills coupled with a framework to understand different levels of cognitive thinking, as well as how it can be assessed.
Conclusion:
To understand differences between undergraduate sonography students and experts, the Dreyfus model is an excellent model to recognize progression. It can be used with the Health Sciences Reasoning Test, which is a nationally recognized critical thinking examination that can ascertain different levels of health sciences students’ critical thinking skills.
Developing critical thinking skills is important for health providers to deliver quality care to patients. For educators, this task is challenging, and measuring student progress is often difficult. Instructors need to use various teaching strategies to promote growth and learning for all students. 1 Facione, 2 a leader in the field, has described critical thinking as a focused, reflective, and credible judgment that incorporates analysis, interpretation, and evaluation, which individuals perform each day. The definition of critical thinking has expanded to include specific cognitive abilities of analysis, interpretation, inference, evaluation, and explanation.3–5 The importance of critical thinking reaches all domains of health professions. It is paramount that educators teach students skills that will mature their cognitive abilities and evaluate student progress.
Dreyfus and Dreyfus 6 published a five-stage model to outline acquired skills to understand student progress from novice to expert thinkers. Since then, Field 7 and Persky and Robinson 8 used this model to illustrate how it applies to sonography skills and pharmacology, respectively. The model described how human intelligence is derived from everyday problem-solving skills, but proficiency intensifies as individuals move past abstract rules and experiences to higher levels of cognitive abilities. 6 The five stages of the Dreyfus model are novice, competence, proficient, expert, and mastery. The model was originally intended for flight training programs but has since found its place in health professions. Field 7 and Persky and Robinson 8 highlighted how the model advances students beyond analytical skills to relying on intuition, but Pena 9 challenged the importance of intuition in medicine because experts also must rely on reason when making appropriate medical decisions.
Current research about critical thinking is mainly focused on nursing, physical therapy, pharmacy, and dental education programs. There are significant publications describing tools that programs use to evaluate students’ critical thinking skills during didactic courses or as admission criteria for selecting desirable students.5,10,11 Currently, there is limited research regarding critical thinking of sonography students. Critical thinking in sonography requires students to constantly search for answers, provide rational explanations, and evaluate their own studies to correctly produce images that aid in diagnosing disease processes. 12 Thoirs and Sim 13 and Penny and Zachariason 12 described how imaging science educators are challenged with developing teaching methods to cultivate critical thinking skills and bridge the gap between theory and practice. In addition, educators need a reliable and valid tool to evaluate student progress.
Methods
The purpose of this review was to analyze the current state of critical thinking in health care and to ascertain if a reliable tool exists. In addition, this review was designed to secure literature that provided a measured difference between a novice’s and an expert’s cognitive abilities and experiences in sonography.
Results
Defining Critical Thinking and Its Importance in Health Care
The APA Delphi consensus described the skills and characteristics of critical thinkers, as well as the importance of fostering these dispositions in all areas of education to produce well-rounded students. The consensus defined critical thinking as a purposeful process, and it included how an individual interprets, analyzes, evaluates, deduces information, explains data, and self-reflects to reach a conclusion. 2 Presently, higher levels of education are required to report on critical thinking, and educators are challenged to nurture this intellectual concept in students. 14 For health professionals, the attributes of critical thinking support healthy clinical decision-making (CDM) skills, so it is imperative that health science students learn aptitudes to encourage growth from a novice to expert practitioner.
Critical thinking is closely associated with CDM, often termed clinical reasoning.4,15 Most sonography programs focus on training, education, and the fine-motor skills required to produce diagnostic images. Sonography students must learn to process a vast amount of data, including a patient’s clinical symptoms, laboratory findings, history, and previous imaging studies, to assimilate specific sonographic information. Thoirs and Sim 13 explained while education builds this core foundation, critical thinking is the actual analytical process that forms clinical judgment. It is imperative students become proficient in critical thinking, so accurate and significant sonographic findings are produced to treat patients and enhance quality care.
There is much debate over a clear definition of critical thinking and if it is linked to clinical judgment or if the terms are interchangeable. Cazzell and Anderson 16 conducted a cross-sectional correlational study to investigate the connection between 11 critical thinking components and clinical judgment. They used four different instruments (Tower of Hanoi [TOH], Health Sciences Reasoning Test [HSRT], Lasater Clinical Judgement Rubric [LCJR], Objective Structured Clinical Evaluation [OSCE]) to explain the phenomena. Cazzell and Anderson 16 found that critical thinking and clinical judgment are two independent concepts and should be defined separately. Their study also revealed that gender and age are not strong predictors of critical thinking, but educational years, nationality, and health care experience have a significant correlation to critical thinking. Therefore, evaluating the scope of clinical reasoning is limited, so assessing critical thinking reflects a student’s ability to make decisions and accurate judgments. Allaire 17 illustrated how higher levels of critical thinking assist students to bridge knowledge to practice. They suggest that clinical reasoning is the mingling of critical thinking with data collection to direct patient care. Like the study by Cazzell and Anderson, 16 Cone et al. 18 argued clinical reasoning is a separate entity of critical thinking because it can be applied to a multitude of settings. Ultimately, students must learn to critically think to provide quality patient care. In addition, Huhn et al. 4 highlighted how the relationship between critical thinking and clinical reasoning is often misinterpreted. They also claimed clinical reasoning is the result of core critical thinking components of analysis, deduction, evaluation, induction, and inference that were developed by the APA Delphi consensus. 4
Frameworks for Critical Thinking
Sonographic reasoning method and CDM model
A systematic process is needed to help students move from theory to practice in clinical rotations and in an independent setting. Similar frameworks have been introduced by Penny and Zachariason 12 and Thoirs and Sim 13 to guide students through the CDM process. Penny and Zachariason 12 incorporated steps from the scientific method to develop a sonographic reasoning method (SRM) framework. The five-step process is a tool sonography educators can use to foster critical thinking and reasoning skills. The goal is to ensure students can apply traditional courses to clinical practice. The authors defined a mnemonic to help students recall the sequential steps in the process. Students can use the relatable term IMAGE to remember each phase of the process: “I” means to investigate patient history, “M” stands for making hypotheses, “A” is analyze with images, “G” represents gathering information, and “E” is evaluate the findings. While this framework might be suitable for some learners, it might not be appropriate for all levels of students.
The framework by Thoirs and Sim 13 is like the SRM introduced by Penny and Zachariason 12 ; however, this model added a reflection process. The use of this CDM model can scaffold student learning in clinical practice. The model is beneficial to students because it guides them to critically think and uses self-learning to deepen understanding. Clinicians can use the model to promote critical thinking for students to bridge the gap between formal didactic courses and clinical practice, and it presents a framework to address critical thinking for other educators to implement. While both frameworks are directly linked to sonography education, research on the effectiveness of each to sufficiently develop strong CDM by improving cognitive abilities remains to be proven.
The Dreyfus model
Dreyfus and Dreyfus 6 first described the skills and experiences needed to move students from novice to expert thinkers. Field 7 depicted how the Dreyfus model could be used as a theoretical framework to explain various levels of critical thinking and move students from novice sonographer to a clinical mastery in the field. In addition, Persky and Robinson 8 used the model to illustrate how pharmacy students acquired aptitudes and critical thinking skills to move from novice to expert during their education. The Dreyfus framework focused on how a novice acquires new skills to be efficient in practice, and it is reliant on instructions rather than a timely trial-and-error approach. 6
Field 7 and Persky and Robinson 8 described specific attributes that students could develop to move from novice to mastery in their specific field. The Dreyfus framework defined the original model stages as novice, competent, proficient, expert, and master. 6 However, the model was revised after adaptation into health care education programs. Current literature uses the following terms to mimic Dreyfus’s original model: novice, advanced beginner, competent, proficient, and expert, 8 and some authors7,9 include a sixth stage, mastery.
Novice performers follow a set of rules when practicing. Individual knowledge at this introductory level lacks experience, and rigorous guidelines are followed without flexibility or responsibility. At this level, performance is sequential and does not allow for variations. 6 As students become competent, experiences are recalled and students proficiently interpret findings, but approaching situations is still stringent because they do not want to overlook less obvious and important findings. 7 During the proficient stage, students begin to have a holistic view of the situation but remain aware of personal limitations and seek help when necessary. No students graduate as experts, but for a practicing clinician to be an expert, intuition is relied upon heavily, with less dependency on analytical skills. They are confident in their decision-making aptitudes and take responsibility for their actions.7,8 Finally, the master stage slightly differs from the expert phase. As a master, clinicians minimally monitor themselves, and they are absorbed in the ease of practice. They can move effortlessly between levels of thinking, intuition is greatly valued, and their opinions and experiences are highly regarded.6,7
However, Pena 9 disagreed that experts and masters rely substantially on intuition for all clinical reasoning decisions because intuition suggests that a person acts in an automatic fashion, with little effort or reflection. In addition, Pena 9 cautioned against the intuitive nature of the Dreyfus model but did agree the model identified some skill acquisitions that reflect knowledge and learning through critical thinking. Field 7 described that intuition is not the only quality of experts and masters, but clinicians at this level are able to effortlessly move between analytical thinking skills and applying intuition; therefore, each provides a solid foundation for clinical reasoning. Comparable to Pena’s work, 9 Field 7 agreed intuition is not always acceptable or measurable. However, Field 7 acknowledged that the importance of the Dreyfus model was to describe acquired skills and not evaluate skills. This is important because Pena 9 based much of his criticism toward evaluation of the model, which was not the intention of Dreyfus and Dreyfus. 6
The Dreyfus model is an appropriate and suitable framework to understand sonography students’ and sonographers’ acquisition skills. The framework can assist educators to develop curricular and instructional strategies to foster critical thinking skills and grow professionals in sonography. As experience is expected to nurture critical thinking, this framework distinguishes specific skill attributions between novice, expert, and master sonographers.
Methodologies to Describe Evaluation of Critical Thinking
Critical thinking is an essential requirement in every health care field, and it is important to assess students’ cognitive abilities throughout educational programs. Many authors agree4,10,11,18 critical thinking is a methodical skill that guides practitioners’ actions, thought processes, and clinical judgment. It includes specific processes of interpretation, analysis, evaluation, inference, explanation, and self-regulation.5,10 Huhn et al. 11 conducted a study of physical therapists that compared novice students to experts. They used HSRT scores to identify differences in critical thinking skills between groups and evaluated construct validity of the HSRT. In a similar study, Hanlon et al. 10 used the HSRT to measure differences in critical thinking of first-year dental students compared to general dentists. They also aimed to establish construct validity of the HSRT to determine differences in critical thinking between novice and expert groups. According to both Huhn et al. 11 and Hanlon et al., 10 construct validity of the HSRT was supported by their findings, and the HSRT was a reliable tool to ascertain differences in critical thinking skills of novice and expert clinicians. While these studies explored critical thinking abilities of physical therapy and dental students, other studies by Nornoo et al. 5 and Cone et al. 18 used the HSRT to evaluate changes in pharmacy students’ critical thinking skills at various points in their education. They found the HSRT was a valid tool to identify changes in critical thinking skills of pharmacy students over a short period.
All these studies4,5,10,11,18 supported the value of the HSRT to measure changes in critical thinking skills. The methodologies in these studies are similar, but the novice-expert method used by Hanlon et al. 10 and Huhn et al. 11 identified differences in critical thinking skills of novice students compared to an expert cohort. Huhn et al. 11 described how novices in a health science field critically think of situations differently from experts. Novices tend to use deductive reasoning compared to inductive reasoning by experts. Modeling Hanlon et al. 10 and Huhn et al., 11 more research is needed to understand critical thinking of novice sonographers compared to experts. A sonography expert would be defined as having at least 5 years of experience and being in good standing with American Registry of Diagnostic Medical Sonographers (ARDMS). These types of studies are needed to better understand if the groups’ method of construct validity, described by Huhn et al., 11 can identify variable levels of critical thinking, the construct in this case, between similar but different groups.
Quasi-experimental designs have many qualities of experimental designs but lack randomization of study participants, similar groups, or both, but these types of designs are effective alternatives when a randomized control trial is not possible. 19 Previous studies10,11,20 used quasi-experimental designs to assess the construct validity of the HSRT to measure cognitive changes between various educational levels of clinicians. Each of the studies listed measured changes of physical therapy students, nursing students, and dental students, but no research was discovered to assess novice and expert sonographers’ critical thinking skills. Based upon previous research described, a quasi-experimental design is an appropriate method to determine differences in critical thinking skills between novice and experienced sonographers.
Tools Used to Evaluate Critical Thinking Skills
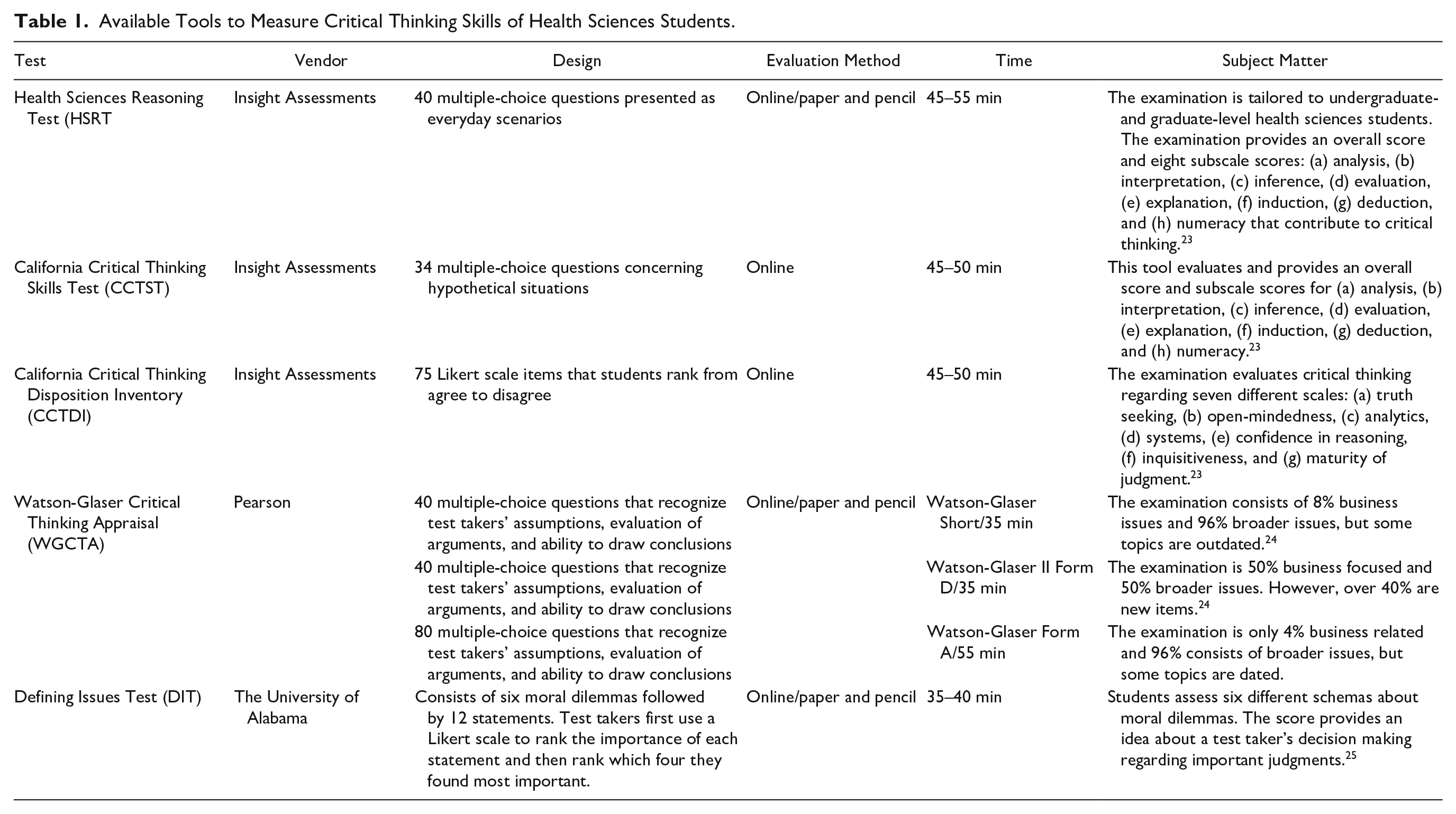
Educators can measure critical thinking skills by using one of three or a combination of validated and distinguished national examinations: the California Critical Thinking Skills Test (CCTST), the California Critical Thinking Disposition Inventory (CCTDI), and the HSRT (Table 1). 18 Huhn et al. 4 described how the Watson Glaser Critical Thinking Appraisal (WGCTA) test has been used to measure critical thinking skills, but its foundation is grounded in business assessments. The HSRT, created by authors of the CCTST, was developed for health science use, but a health science background is not required for students to challenge the examiantion.4,18 The HSRT is a 33-question multiple-choice test to measure critical thinking skills in undergraduate and graduate health science students, it is shorter compared to other assessments, and it provides an overall score along with subscores measuring analysis, inference, evaluation, induction, and deduction.4,18,20 The reliability of the HSRT is important, and it has been established by the Kuder-Richardson Formula 20. Sharp et al. 14 and Cazzell and Anderson 16 reported the internal consistency of 0.81, and reliability ranges from 0.77 to 0.84.16,20 Similar to reported reliability, subscale score reliability on the HSRT varies between 0.78 and 0.84. 16 Many studies have used the HSRT to measure changes in students’ critical thinking, and each determined it was a valid and reliable tool to evaluate cognitive abilities of students.4,10,11,14,17,18,20
Available Tools to Measure Critical Thinking Skills of Health Sciences Students.
Huhn et al. 4 compared two physical therapy programs to ascertain if the HSRT could indicate a measurable change in students’ critical thinking. The researchers evaluated students three separate times in the program: upon entry into the program, before their final year, and upon graduation. This provided data over four years for analysis. They found the HSRT was an appropriate tool to measure changes of physical therapy students in critical thinking, and they were able to describe when the biggest change occurred because of various timings of sampling. They performed statistical analysis to compare schools and subtopics of the examination, and they provided descriptive data about students’ demographics to ensure students were nearly equal at baseline. Another study by Sharp et al. 14 used the HSRT to evaluate differences in critical thinking between allied health programs, the strength of the students’ critical thinking skills, and the difference in critical thinking skills between academic levels of learning. Like Sims and Thoirs, 15 they highlighted a gap in literature related to critical thinking skills of students in allied health programs compared to medicine and nursing programs. Students were tested only one time during Sharp et al.’s study, and the scores were compared to the HSRT test manual to determine what critical thinking category matched students’ cognitive abilities. The results indicated nearly 65% had weak critical thinking skills, 31% had moderate critical thinking skills, and almost 4% exhibited strong skills to critically think. The type of allied health program resulted in significant statistical differences, with dental hygiene achieving lower scores and cytotechnology having the highest. Academic levels resulted in bachelor participants having the lowest scores, but entry-level master program students scored higher than master-seeking degree participants. 14 Finally, Nornoo et al. 5 conducted a study to identify if a correlation existed between pharmacy students’ critical thinking insert assignment packet grades and HSRT scores. Their findings suggested a weak but significant correlation of package inserts to measure critical thinking skills of pharmacy students. 5
Contradicting the studies by Huhn et al. 4 and Sharp et al. 14 was a meta-analysis by Reale et al. 21 that only included longitudinal studies to understand critical thinking of a broad range of health science students. They reviewed studies that used the CCTST, HSRT, or Defining Issues Test (DIT) to evaluate students’ critical thinking skills, and the studies included must have tested students on at least two occasions. They excluded cross-sectional studies, literature that only tested students a single time during a program, and studies that did not use a valid tool like the previously stated critical thinking examinations. Data supported the CCTST and the DIT as useful tools to evaluate changes in cognitive abilities of students compared to mixed results of the HSRT. The CCTST and DIT showed representative changes in critical thinking over time, but the data did not document changes over time by the HSRT. Similarly, Carter and Welch 22 used a quasi-experiment to assess critical thinking skills. They used unfolding case studies to understand the effects of Associate degree nursing (ADN) students’ knowledge and critical thinking skills. Carter and Welch 22 used intact groups from the same course but different years to compare traditional teaching strategies to unfolding case studies, and they collected data by a pretest/posttest on two different content areas and by a pretest/posttest using the HSRT. In contrast to other studies4,14,18 but like findings by Reale et al., 21 Carter and Welch 22 did not find any correlation between HSRT results and increased critical thinking skills of nursing students.
Simulation is a pedagogical tool used to improve critical thinking skills. Allaire 17 used the HSRT pretest/posttest design to measure students’ critical thinking skills after simulation learning experiences. The HSRT did not produce statistically significant differences in the mean scores of students, but when students were compared individually, some improved their scores from 2 to 6 points. Although the study did not result in statistically significant changes in critical thinking, it did prove once again that the HSRT was a reliable and valid tool to measure changes in cognitive abilities of students.
Conclusion
Several authors have defined critical thinking and described its importance to deliver quality health care, and health care providers must think analytically and intuitively to ensure patients receive the best care possible. Sonography educators need a reliable and valid method to assess cognitive skills, so instruction and curriculums can be tailored to meet student needs. Many health education programs, including pharmacy, physical therapy, dentistry, and nursing, are evaluating students’ cognitive abilities, and it is clear research is needed to explore sonography students’ critical thinking skills. Sonography educators need support to develop best practices to consistently assess students’ cognitive growth and reliably report findings.
Evidence-based research in other health education programs has established the capability of the HSRT to detect changes in cognitive skills when assessing different levels of experience between groups. Comparing novice to expert sonographers using the Dreyfus model of skills acquisition and incorporating an evaluation tool like the HSRT can be an effective method and instrument for educators to examine this phenomenon. The Dreyfus model describes the importance of instruction and experience to progress students from novice clinicians to expert practitioners during their careers. It also explains what skills are necessary to understand how students advance from analytical thinking to intuition and higher levels of critical thinking. By comparing novice students to expert sonographers, educators can recognize how important a variable like experience, for example, promotes cognitive abilities in sonography. Modeling the study by Huhn et al., 4 educators could also use the HSRT to assess sonography students at baseline and again at graduation to evaluate strengths and weaknesses of cognitive abilities. Some might also consider incorporating either the CDM framework introduced by Thoirs and Sim 13 or Penny and Zachariason’s 12 SRM to a curriculum and correlating findings using the HSRT. Although some research has contradicted using the HSRT as a tool to assess students, more data are needed to guide educators to conduct assessments that reflect increased cognitive abilities. It is imperative that sonography educators continue researching critical thinking of sonography students, highlight unique tools to cultivate cognitive abilities, and clearly outline how to reliably and consistently evaluate students’ aptitudes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.