
Abstract
Objective:
Self-referral community cardiovascular screening programs (CCSPs) have a potential to reduce outcome events through early detection of disease. This study evaluated the characteristics of a population that could predict a positive test.
Materials and Methods:
Participants who completed a cardiovascular screening protocol were compared. The screening protocol included a blood pressure (BP), Doppler ankle brachial index (ABI) testing, a limited carotid sonogram, a limited aortic sonogram, electrocardiogram (ECG), and limited transthoracic echocardiogram (TTE).
Results:
Screenings were performed on 205 participants (58% female, 68 ± 9 years of age). Sixty-seven (34%) participants were abnormal in at least one of the following screening tests: ABI (2%), carotid sonogram (6%), aortic sonogram (3%), ECG (11%), and TTE (22%). Although 60.5% of the participants reported recent symptoms, there were no differences in normal or abnormal results of participants presenting with or without symptoms (P = .06). Income was not a predictor of abnormal test results (odds ratio, 0.76; 95% confidence interval, 0.55–0.97; P = .19). Multivariate analysis demonstrated, when controlling for age greater than 75 years, that participants taking BP medication was the only variable that predicted a positive test result.
Conclusion:
One-third of patient results were abnormal, regardless of symptoms or lack thereof, suggestive of subclinical disease. Further large-scale studies would demonstrate the role of CCSPs in risk stratifying participants.
Stroke and heart disease are a major public health problem in the United States and worldwide. Despite a decrease in cardiovascular mortality rates by 28.8% from 2003 to 2013, 1 cardiovascular disease (CVD) is the leading cause of death in men and women. 2 In 2015, national statistics estimate that the percentage of adults (60–79 years of age) with CVD was slightly higher in men at 69.1%, compared to 67.9% for women. 2 Total direct and indirect costs attributable to both stroke and heart disease in the United States are estimated to be $316.6 billion annually. In addition, associated hospital discharges nearly doubled from 3.3 million in 1970 to over 6.2 million in 2000.2,3 By 2030, total costs are estimated to increase to $918 billion with indirect costs increasing by 58%. 1 Cardiovascular mortality continues to be high, ranging from 245.2 deaths per 100,000 Americans age >65 years for stroke and 222.9 deaths per all 100,000 Americans for heart disease in 2013. 4 Over 1.2 million people have a heart attack yearly, and stroke occurs in almost 800,000 people yearly. 5
Community cardiovascular screening programs (CCSPs) are a self-referral, self-paid, open-access service and located in a variety of settings. This is in contrast to diagnostic services and testing that require documentation of symptoms and a physician referral for access to testing and treatment. Community cardiovascular screening provides the ability to detect a variety of significant cardiac and vascular diseases, including detection of structural, electrical, and mechanical heart disease6–12 along with peripheral vascular disease.13,14 These conditions contribute to stroke and cardiac disease resource burden for health services utilization and cost.15,16
Early detection of CVD and appropriate classification of patients into higher risk categories with more effective early treatment may reduce morbidity, decrease mortality, and improve quality of life. 17 However, there is continued uncertainty as to the benefit of CCSPs because of the lack of evidence in potential harm and cost comparison.18,19 The objective of this study was to examine participant demographics and screening results in a CCSP. Describing the age, sex, race, reported exercise frequency, history, and risk factors for CVD will help to characterize the risk profile of people presenting to a screening program provided in a variety of nonacute suburban community locations (e.g., mall, church, bank, and outpatient center).
Materials and Methods
Participants were prospectively recruited from a CCSP (locally branded: The Heart Report Card, which is a self-referral, self-paid screening offering not requiring a physician order in Lee County, Florida). After having the cardiovascular screening performed at four outpatient testing facilities or at a community venue (e.g., bank, church, or gated community), participants were asked to be included in the research study. Agreeable participants were consented if they were over 18 years of age. Participants answered questions about participant demographic characteristics and completed a health risk assessment. The health risk assessment inventoried race, marital status, sex, height, weight, exercise frequency, and health history, including heart history, cardiovascular (CV) risk factors including diabetes, high blood pressure, peripheral vascular disease, smoking history, and medications. Median 2015 income status, for Lee County ZIP codes in Florida, was used as a surrogate for socioeconomic status of presenting participants. All participants provided written, informed consent, and the study was approved by the institutional review committee at Lee Health, Fort Myers, Florida.
Cardiovascular testing included blood pressure, Doppler ankle brachial index (ABI) testing, a limited carotid sonogram, a limited aortic sonogram, electrocardiogram (ECG), and a limited transthoracic echocardiography (TTE). The detailed protocol used is presented in Figure 1. All testing was performed by registered sonographers (Registered Diagnostic Cardiac Sonographer, Registered Cardiac Sonographer, Registered Vascular Sonographer, and Registered Vascular Technologist) on equipment currently used for diagnostic testing in the health care system (CX50; Philips, Bothell, WA). All testing was completed within 20 to 30 minutes. All examinations were interpreted by a board-certified cardiologist with specialty credentialing in both cardiac and vascular interpretation. An on-call cardiologist was available for participants who had critical results defined as life-threatening findings.
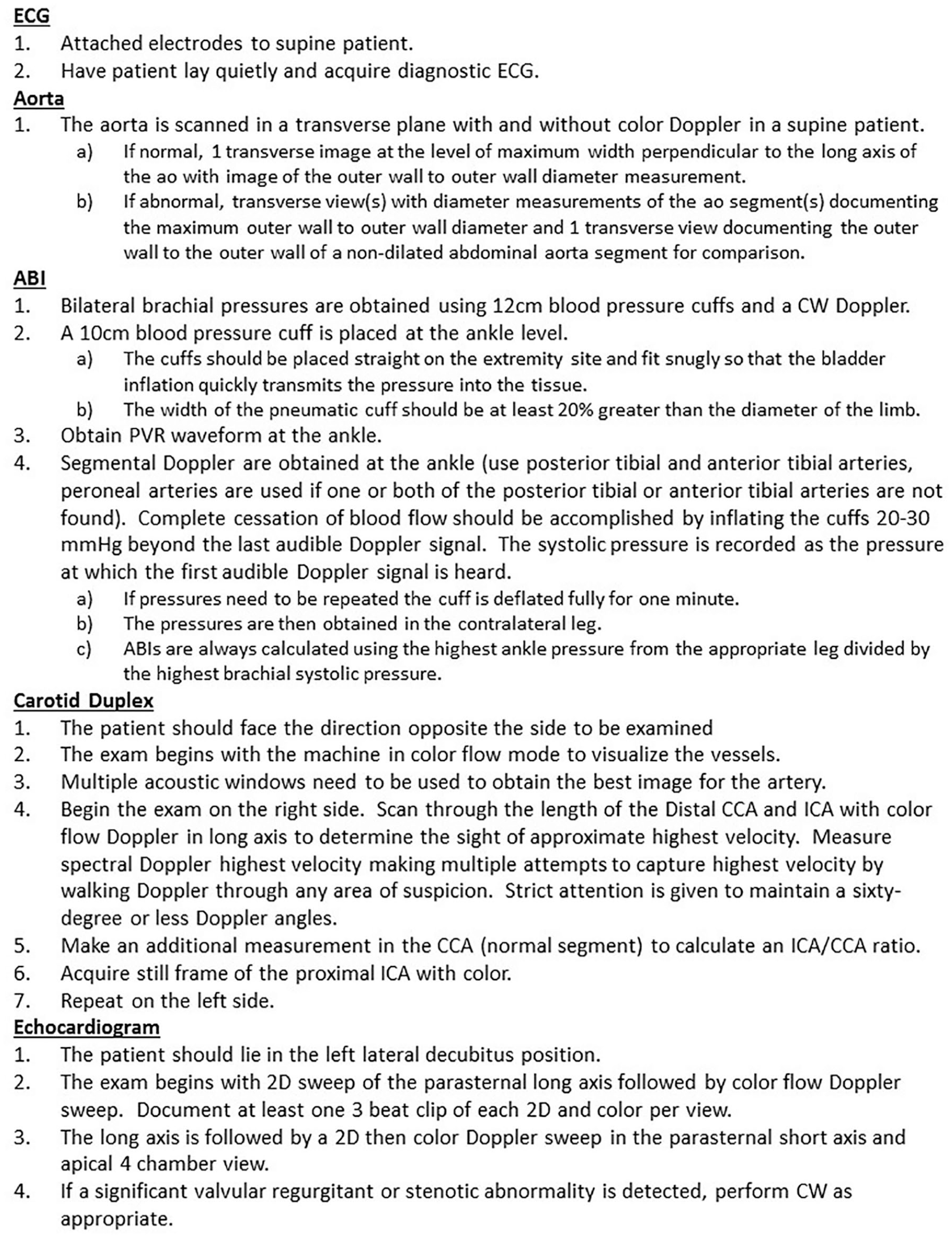
Protocol used in the community cardiovascular screening program testing. ABI, ankle brachial index; CCA, common carotid artery; CW, continuous wave; ECG, electrocardiogram; ICA, internal carotid artery; PVR, peripheral vascular resistance.
Abnormal blood pressure was defined as a systolic pressure greater than 120 mm Hg and diastolic greater than 80 mm Hg. The screening was considered positive/abnormal if the following criterion was detected in these imaging tests: carotid sonogram, right- or left-sided internal carotid artery peak systolic velocity of greater than 125 cm/s was considered abnormal, and right or left internal carotid artery to common carotid artery ratio of greater than 2 was considered abnormal; aorta of greater than 3.0 cm was considered abnormal; ABI of less than 0.9 was considered abnormal; TTE, an ejection fraction of less than 50% or mild/moderate/severe mitral regurgitation, mitral stenosis, aortic insufficiency, aortic stenosis, or tricuspid regurgitation was considered abnormal; ECG was considered abnormal if any of the following was present: arrhythmia (atrial fibrillation or flutter) or conduction abnormalities (left atrial fascicular block, left or right bundle branch block, atrioventricular blocks, left ventricular hypertrophy by voltage, or nonspecific ST, T-wave, or Q-wave abnormalities).
Descriptive statistics for variables of interest were calculated for all participants. The frequencies of positive or abnormal screening results were determined for each type of screening test. If any of the screening tests were positive for abnormalities, the screening was considered abnormal. We performed t tests performed to compare the means for continuous variables and χ2 tests to compare proportions for categorical data. For all analyses, a P < .05 was considered statistically significant. Multivariate logistic regression analysis was performed to identify predictors of an abnormal screening from among varied descriptor variables, including ZIP code, age, sex, marital status, race, body mass index (BMI), reported history of diabetes, hypertension, family CV disease, smoking history, current smoker, having been on blood pressure– or cholesterol-lowering medications, vitamin use, or exercise frequency. A standard deviation was calculated from the distribution of the income sample. Income cutoffs were created as one standard deviation from the median. Data were analyzed using the SPSS software (version 23.0 for Windows; SPSS, Inc., an IBM Company, Chicago, IL).
Results
Participants were screened and consented between December 2014 and October 2016. Of 205 enrolled, 68 (33.2%) were abnormal in at least one of the following screening tests: ABI, 5 (2.5%); carotid sonogram, 13 (6.4%); aortic sonogram, 5 (2.5%); ECG, 23 (11.2%); and TTE, 45 (22.2%). Table 1 provides the demographic characteristics showing no difference between the normal and abnormal imaging group in age, sex, marital status, race, participant physical exercise frequency, or reported symptoms. Participants with abnormal imaging results were found to have peripheral vascular disease (P = .04) more frequently and were on blood pressure medications (P = .02). ECG was abnormal in 49 (33.2%) participants, with atrial fibrillation or flutter in 5 (3.4%), conduction abnormalities in 12 (8.1%), left ventricular hypertrophy in 10 (6.8%), nonspecific ST T-wave abnormalities in 9 (6.1%), and Q-wave abnormalities in 13 (8.8%). Vascular (ABI, carotid sonogram, or aortic sonogram) imaging was abnormal in 19 (9.3%) of participants. Echocardiographic imaging was abnormal in 45 (22.2%) participants, with 37 having heart valve abnormalities, 5 having wall motion abnormalities, and 3 having both heart valve and wall motion abnormalities. The severity of detected valvular abnormalities is as follows: 28 with mild mitral regurgitation, 10 with moderate mitral regurgitation, 1 with moderate mitral stenosis, 15 with mild aortic insufficiency, 4 with moderate aortic insufficiency, 1 with severe aortic insufficiency, 1 with mild aortic stenosis, 14 with mild tricuspid regurgitation, 7 with moderate tricuspid regurgitation, and 1 with severe tricuspid regurgitation. When evaluating the number of positive tests per patient, 50 (24.4%) had one positive test in the screening, 13 (6.3%) participants had abnormal findings in two tests, and 5 (2.4%) participants had abnormal findings in three tests during their screening. Although not considered a positive imaging result, blood pressure was elevated in 118 (57.6%) of participants. No critical or life-threatening results were detected with the screening cardiovascular imaging.
Mean (SD) and Frequency (Percentage) Across Descriptive Variables Among Participants With Normal Versus Abnormal Screening Results. a
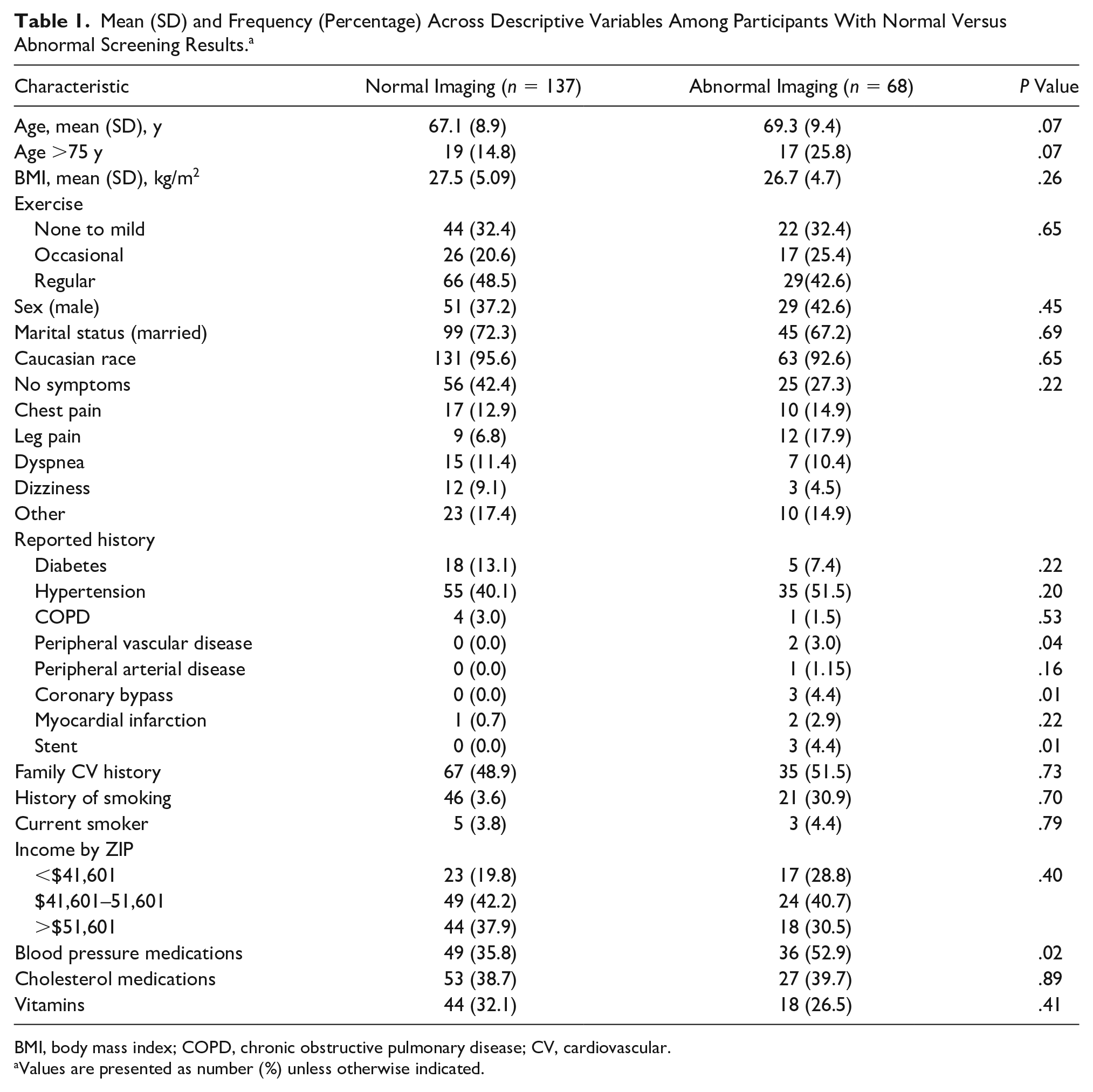
BMI, body mass index; COPD, chronic obstructive pulmonary disease; CV, cardiovascular.
Values are presented as number (%) unless otherwise indicated.
Although having symptoms did not predict a positive result, 124 (60.4%) of participants reported having recent symptoms: chest pain (14%), dyspnea (12%), leg pain (11%), and dizziness (8%). When comparing patient demographics between participants presenting with or without symptoms, those participants having symptoms were more likely to be older (69.6 ± 8.9 versus 65.3 ± 9.0, P = .02), exercise less (P < .01), have a history of smoking (P = .02), and be taking cholesterol medication (P = .05) (Table 2). In asymptomatic participants, testing was abnormal in the following screening tests: ABI (1.2%), carotid sonogram (4.9%), aortic sonogram (1.2%), ECG (16.0%), and TTE (19.7%).
Demographics of Symptomatic Versus Asymptomatic Participants. a
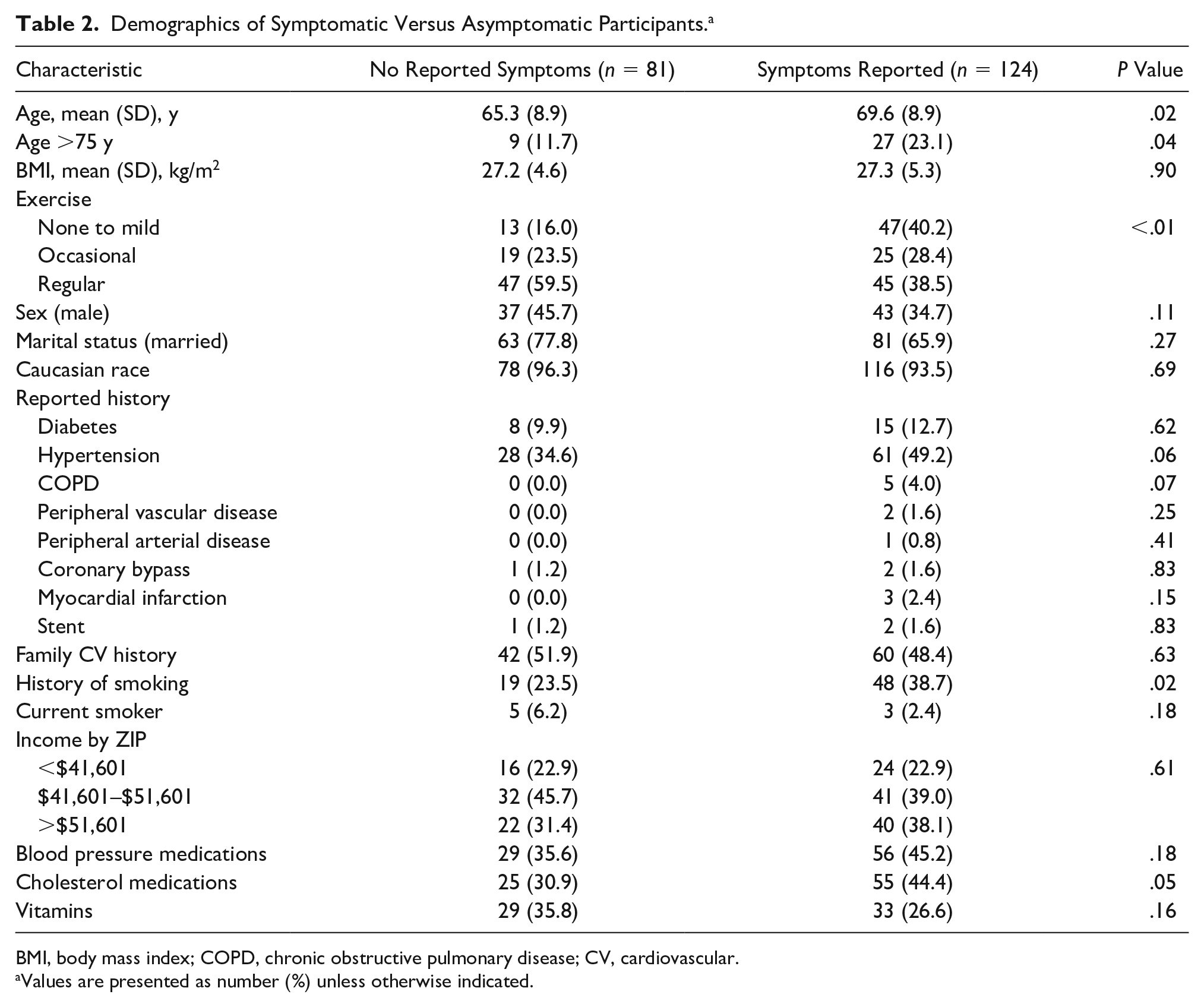
BMI, body mass index; COPD, chronic obstructive pulmonary disease; CV, cardiovascular.
Values are presented as number (%) unless otherwise indicated.
A comparison of participants to the county from which they present was completed. The median age of the screening population was 68.3 years, whereas the median age of people living in Lee County, Florida, was 46.3 years. 20 The screenings were performed in a variety of locations with ZIP codes having a median household income ranging from $40,038 to $59,161 in 2015. 21 Figure 2 compares the number of participants presenting for the screening compared to the household income from their presenting ZIP code. The median household income for Lee County was $46,601. Income data were unavailable in 30 (14.6%) of participants who presented from counties outside the state of Florida. Of participants having ZIP code information, 41.7% had an associated median household income between $41,601 and $51,601. Forty (22.9%) participants presented from ZIP codes with a median household income less than $41,601. Sixty-two (35.4%) participants presented from ZIP codes with a median household income more than $51,601. Household income was not a predictor of abnormal test result (P = .18).
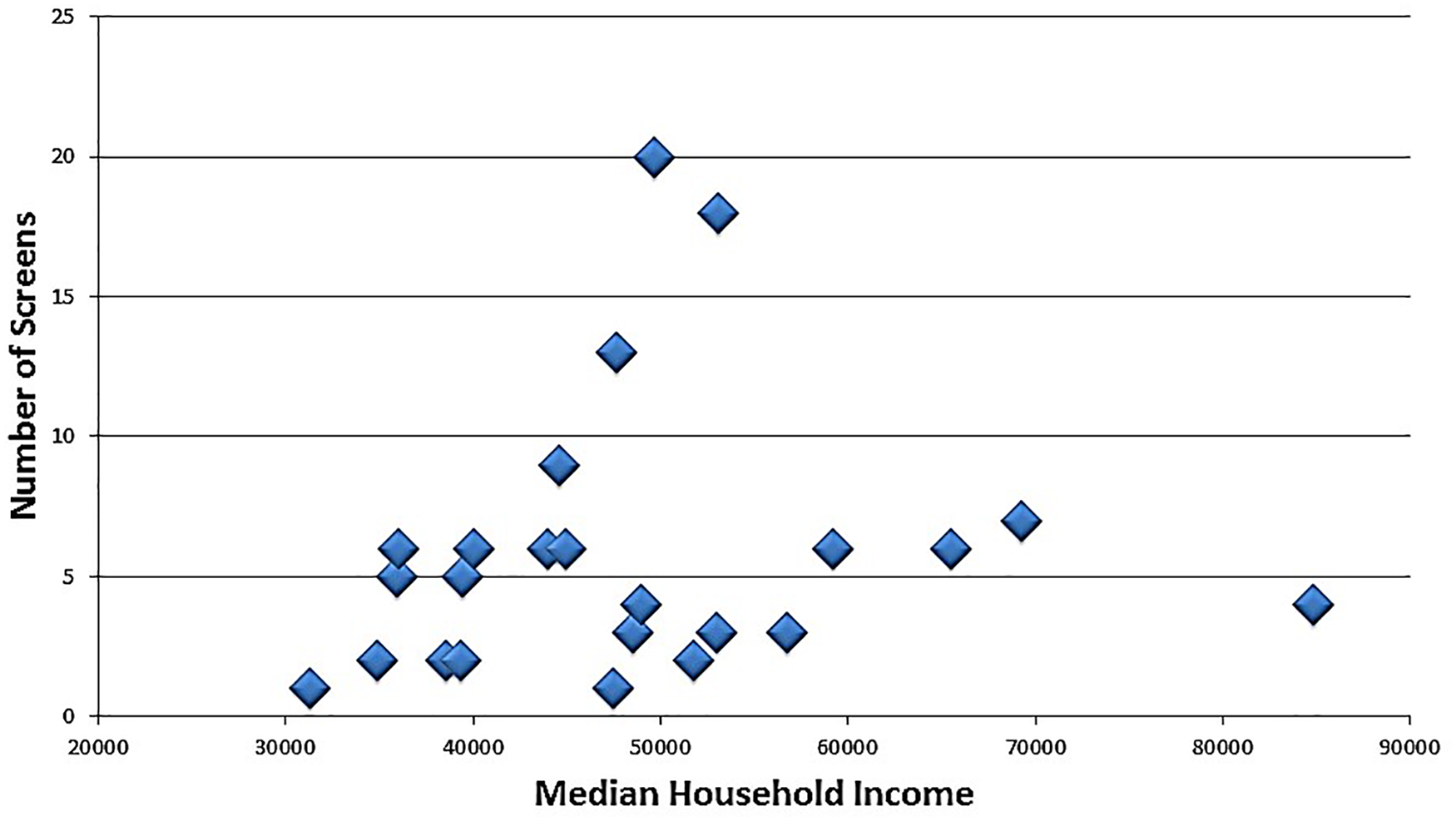
Number of screens performed with median household income distribution.
Multivariate analysis for independent predictors of a positive/abnormal imaging test showed that when controlling for age greater than 75 years, blood pressure medication was the only predictor approaching significance for a positive test (odds ratio [OR], 1.87; 95% confidence interval [CI], 1.01–3.46; P = .05) (Table 3). No other factors were predictive of a positive test. This included an evaluation of demographic variables of income from ZIP code, age, sex, marital status, race, BMI, reported history of diabetes, hypertension, family CV disease, smoking history, current smoker, having been on blood pressure– or cholesterol-lowering medications, vitamin use, or exercise frequency.
Predictors of Any Positive/Abnormal Imaging Screening Result (n = 175).
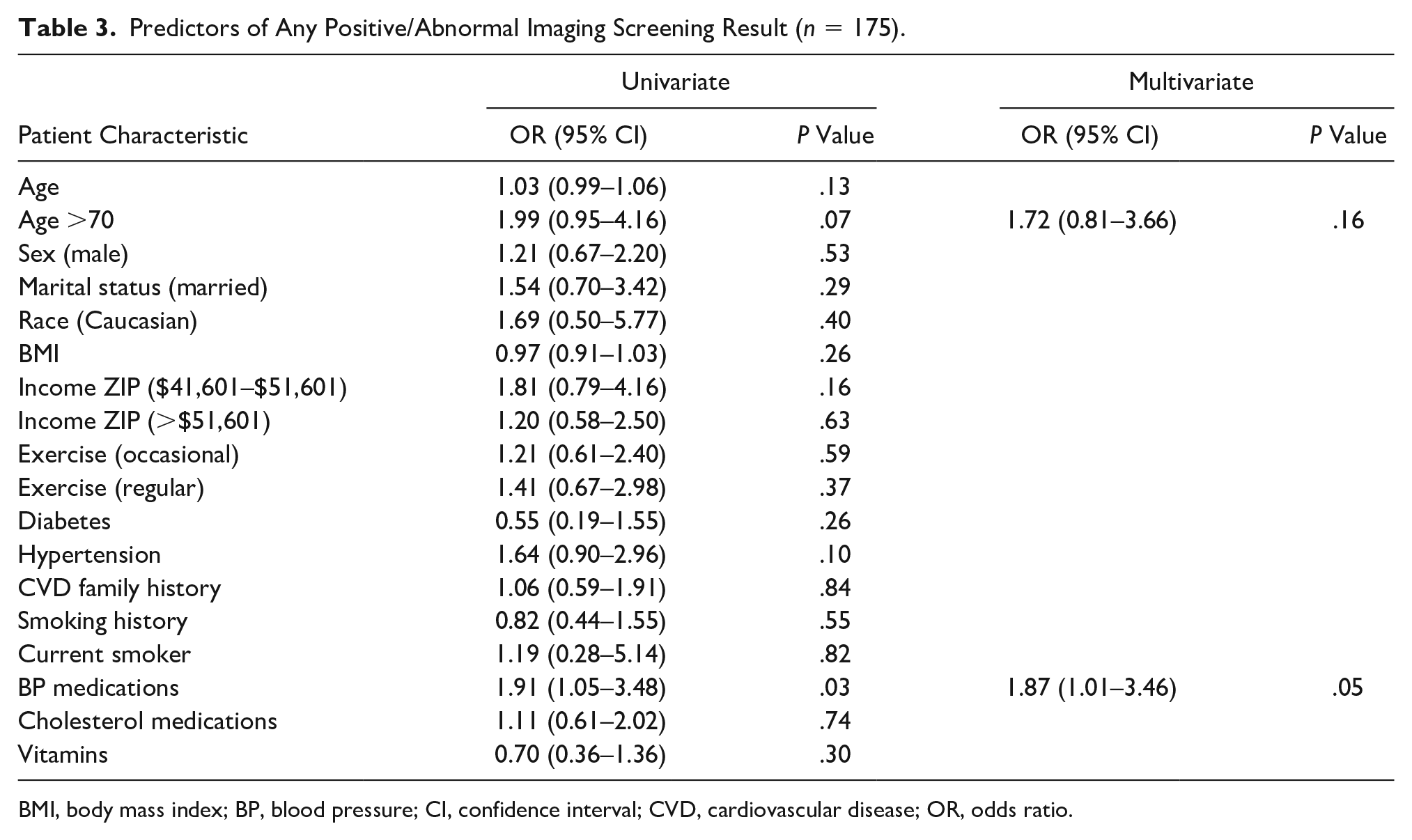
BMI, body mass index; BP, blood pressure; CI, confidence interval; CVD, cardiovascular disease; OR, odds ratio.
Discussion
A primary outcome for this community CV screening program was that it was the first study to evaluate income range and cardiovascular screening and to demonstrate that socioeconomic status did not predict differing abnormal rates. Previous studies have suggested that targeted screening in lower socioeconomic areas may yield a higher rate of abnormalities, as some might suggest. 22 The current study would suggest no differentiation in rate of positive results by socioeconomic area; therefore, CCSPs may be beneficial in both low and high socioeconomic areas.
In addition, another important finding of this study was that only 39.5% (n = 81) of participants presenting for CCSP reported being asymptomatic, yet the 30.9% of asymptomatic participants had an abnormal result versus 34.7% of symptomatic participants (P = .57). Although the 2011 Appropriate Use Criteria published by the American Society of Echocardiography (ASE) and the American College of Cardiology (ACC) recommend screening for initial evaluation of heart function in asymptomatic subjects only rarely appropriate, 18 a CCSP may beneficial in detecting silent cardiovascular disease. In addition, the US Preventive Services Task Force released a statement against carotid sonographic screening in the asymptomatic general adult population due to the possibility of false-positive test results and unnecessary added testing. 23 The current study would suggest, however, that 4.9% of carotid disease could be missed using this approach. Carotid plaque detected with sonography may provide a risk algorithm and treatment guide for asymptomatic participants.24,25 Although the majority of these symptomatic study participants demonstrated a significant difference in the rate of detected screening abnormalities compared to those without symptoms, it suggests the need for CCSPs performed to detect silent (undiagnosed), asymptomatic, or subclinical disease, as well as their appropriate risk stratification and management.26,27
In comparison to other studies evaluating cardiovascular screening in the general population, 28 the current study participants were older, 67.9 years of age in the normal group versus 60.5 years cited as a control group of the general population. Sex was more frequently female (57.6%) versus 44.8% in previous screening studies evaluating the general population. The current study had a lower proportion of participants with hypertension (41.3%) versus 60.1% in a Danish population and a higher rate of diabetes (12.9% versus 4.3%). 28
These study participants’ prevalence of heart function abnormalities (21.9%), detected by TTE, was higher than studies that reported a detection rate of 1% to 14% for heart function abnormalities.9,10 This may be due to the screening of a population reporting no symptoms in comparative studies, whereas 59.5% of the current study participants reported having symptoms including chest pain, dyspnea, and dizziness. Previous studies screening “asymptomatic” participants and detecting new heart failure in 10% to 20% of the population 11 were more consistent with the current study, which demonstrated 19.7% of asymptomatic participants having abnormalities on the TTE. This study detected a positive ECG screening rate of 11.2%, which is similar to prior studies that demonstrated that 15% of the population requires follow-up testing after finding ECG abnormalities. 12
Carotid sonography was found to be abnormal in 12 (6%) participants, which is similar to a previous population screening for carotid disease demonstrating a 9% positive detection rate. 13 This study presents a lower detection rate than studies looking at a higher risk population with a subclinical plaque detection in 34% of participants. 27 This the first study to report ABI-positive screening rates (2.5%) in a CCSP. Four aortic abnormalities (2%) were found, which may be due to Centers for Medicare and Medicaid Services (CMS) currently paying for a onetime sonographic screening for abdominal aortic aneurysms (AAAs), given a physician referral. 29 The current study was consistent with previous studies, which have demonstrated the effectiveness of CCSPs to detect AAAs. 30
This prospective study provided similar demographic results comparted to prior studies 31 and has additional detailed imaging analysis of cardiac and vascular imaging results. The presenting participants were older than the general population, were primarily Caucasian, and could not be randomized, which limits generalizability of the results. A comparison to the demographics from the county in which the screenings were performed was completed, but this could not account for all characteristics. This study used only portable noninvasive imaging performed in a variety of community settings. No additional imaging (e.g., computed tomography) was used as part of the screenings. This screening strategy does not exclude participants reporting symptoms, which could increase the rate of detection of abnormalities. It is also not known if the participants were having the screening performed because they were dissatisfied with current health care or were being proactive about their health and wellness. A complete patient physical was not performed with associated clinical history and laboratory work, which could further clarify health and risk profiles in future studies. A larger, more diverse sample size would be necessary to validate if blood pressure medication continues to approach or reach significance in predicting a positive test.
Conclusion
This study may suggest that clinically silent cardiovascular disease may be present in a third of adult populations regardless of presenting subject symptomatology. Self-referred CCSPs may be valuable tool in detecting unrecognized CVD by using high-quality imaging equipment used by certified imaging technologists and credentialed physicians.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.