
Abstract
Endovenous ablation is a common procedure performed on the superficial veins of the lower extremities to treat symptoms of venous insufficiency and varicose veins. While endovenous ablation is a minimally invasive procedure, patients may develop thrombotic complications including endovenous heat-induced thrombosis. Endovenous heat-induced thrombosis is a rare complication of thrombus extension from the superficial vein into or near the deep system postprocedure. In this case report, a female with a history of recent endovenous ablation presented to the emergency department with symptoms of a pulmonary embolism. Sonographic evaluation of the right lower extremity revealed extension of thrombus from the ablated superficial vein into the common femoral vein. Thrombus was also noted in the left lower extremity extending from the ablated superficial vein to approximately the saphenofemoral junction. While the left lower extremity was being interrogated, the thrombus was documented, via a cine clip, liberating from the occluded great saphenous vein. Further assessment utilizing computed tomography revealed bilateral pulmonary emboli. This unique case emphasizes the importance of sonographic evaluation post-endovenous ablation.
It is estimated that as many as 25% of women in the United States have varicose veins, with many patients opting to seek medical intervention to reduce symptoms. 1 Presenting as enlarged and tortuous superficial veins, varicose veins occur when venous valves are damaged or incompetent, causing blood to pool in the superficial vessels. Treatment options for varicose veins consist of nonsurgical and surgical interventions, with surgical options including surgical ligation, sclerotherapy, and endovenous ablation. 2 Endovenous ablation (EVA) is considered the modality of choice for venous insufficiency and varicose vein treatment. 3 Although EVA is a minimally invasive procedure, there is a risk of thrombotic complications, including endovenous heat-induced thrombosis (EHIT), deep vein thrombosis (DVT), and a subsequent risk of pulmonary embolism (PE). 4 EHIT is a rare thrombotic complication of thrombus extension from the superficial vein into or near the deep system post-EVA procedure. 5 Untreated, the complications of PE can be fatal. 6 Thus, sonographic evaluation of the affected area post-EVA is generally accepted in the clinical setting to ensure early detection and treatment of thrombotic complications. With early sonographic detection and subsequent treatment, patients can expect a normal recovery with little to no symptoms.
Case Report
A 72-year-old female presented to the emergency department (ED) with complaints of stabbing pain in her lower right chest that radiated to her back. The patient had been experiencing pain, shortness of breath, and nausea for approximately 5 hours. It was noted that the patient had undergone a bilateral radiofrequency ablation (RFA) of the great saphenous veins approximately 10 days prior to arriving to the ED. At the time, she stated she had been taking two low-dose aspirins every day since the procedure and was recently on an extended car ride. Thus, a bilateral lower extremity venous duplex exam and a computed tomography (CT) exam were ordered under the suspicion of DVT and possible PE. Sonographic evaluation of the right lower extremity revealed extension of thrombus from the ablated superficial vein into the common femoral vein (Figure 1). Thrombus was also noted in the left lower extremity extending from the ablated superficial vein to approximately the saphenofemoral junction (SFJ). While the left lower extremity was being interrogated, the thrombus was documented, via a cine clip, liberating from the occluded great saphenous vein and traveling through the common femoral vein in the direction of venous flow (Figure 2 and Video 1 in the Supplemental Material available online). The remainder of the exam was unremarkable.
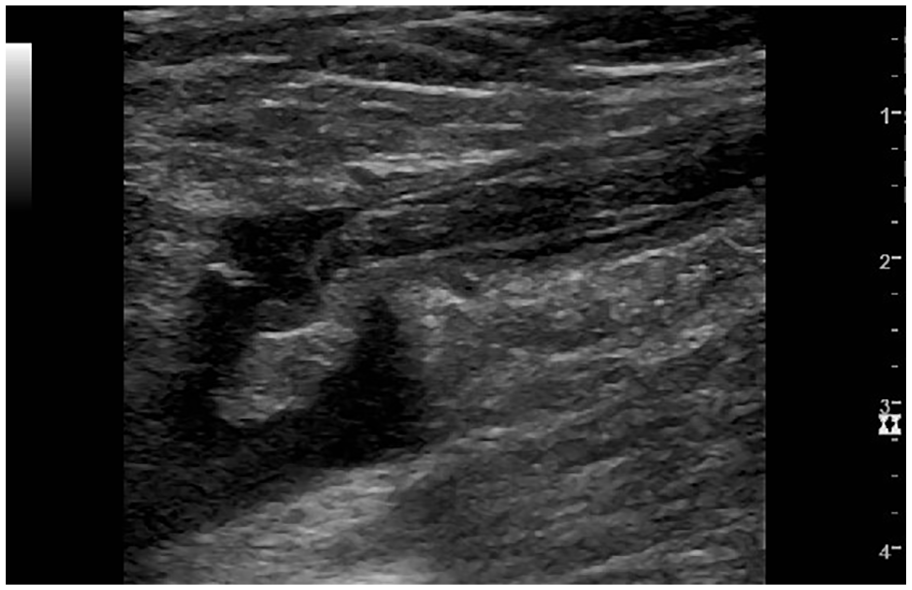
Thrombus in the right great saphenous vein (GSV) protruding into the right common femoral vein (CFV).
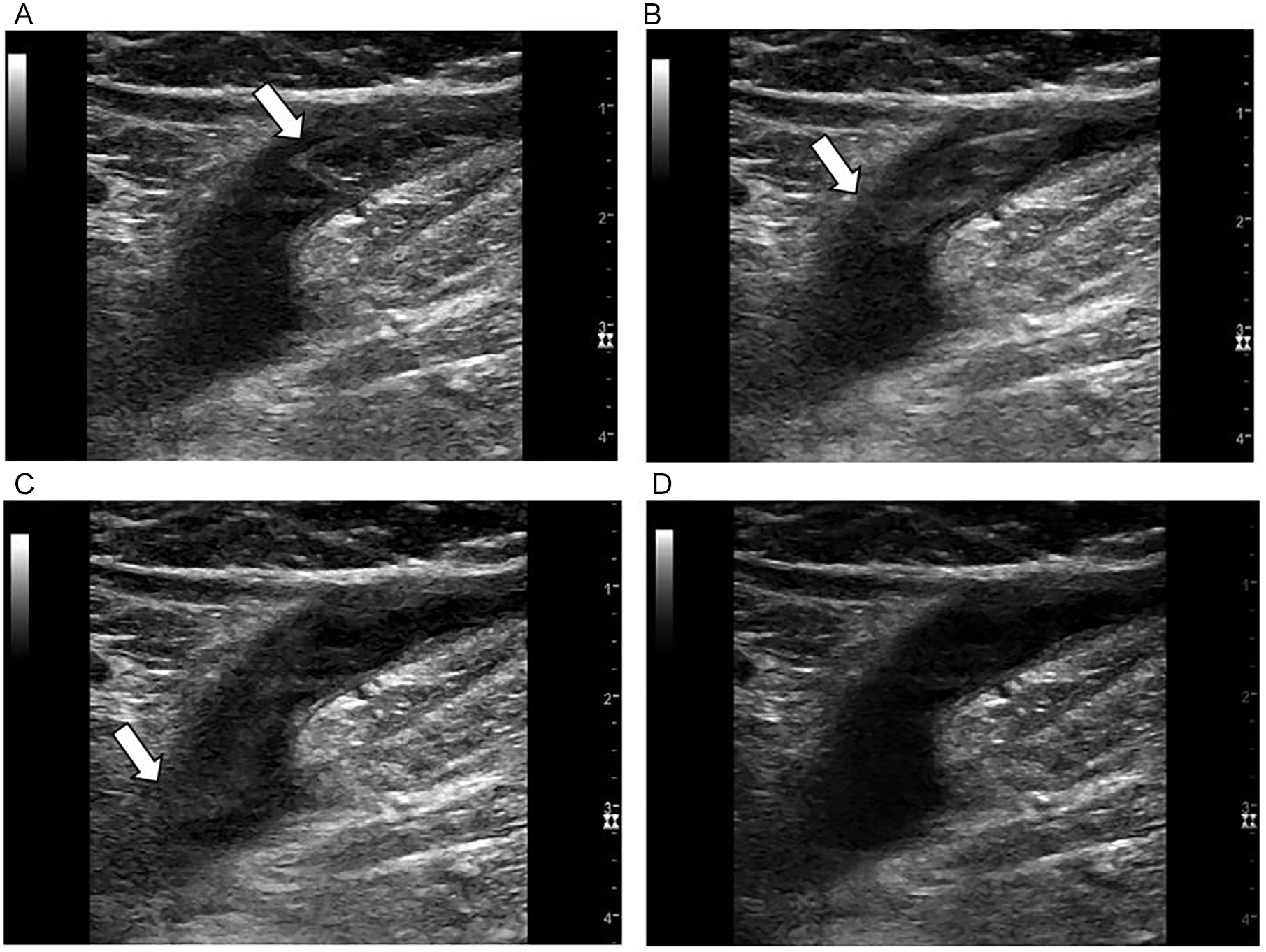
Thrombus documented liberating from the ablated great saphenous vein (GSV) and traveling through the common femoral vein (CFV). (A) Arrow indicating the proximal end of the thrombus at its initial location. (B) Arrow indicating the proximal end of the thrombus, now at the level of the saphenofemoral junction (SFJ). (C) Arrow indicating the proximal end of the thrombus as it travels into the CFV. (D) After the thrombus has completely passed through into the CFV.
The patient was also taken to the CT department for a CT pulmonary angiogram (CTPA). The evaluation revealed bilateral segmental and subsegmental PE. A cardiologist was consulted and reported that the thrombi in the great saphenous veins, with resultant thrombus embolization, were likely a provoked event due to recent EVA procedure in addition to a protracted car ride. Anticoagulation alone was recommended because the patient had no indication for advanced therapies.
Discussion
The venous system of the lower extremities is classified into three groups: deep veins, superficial veins, and perforator veins. Deep veins lie beneath the muscular fascia and drain the blood of the lower extremity up to the inferior vena cava (IVC). 7 The superficial veins lie above the muscular fascia and drain cutaneous microcirculation into the deep venous system. 7 This is made possible with veins known as perforator veins, which are small veins that connect the superficial and deep venous systems. In normal patients, blood flows from the superficial veins to the deep system. Nevertheless, when venous valves are damaged or incompetent, blood can pool in the vessel and cause it to swell. This process leads to the development of varicose veins, which present as enlarged and tortuous superficial veins. 8 Chronic venous disease, including varicose veins, affect around 25% of the adult population in developed countries. 9 Varicose veins can present with varying severity, causing discomfort, pain, and development of skin ulcers, and potentially result in the deterioration of patient’s quality of life.2,10 Currently, there are several treatment options for varicose veins, including traditional surgical ligation, sclerotherapy, and EVA. 2 However, EVA continues to be considered the treatment of choice for varicose veins. 3
Endovenous Ablation
EVA is a minimally invasive procedure that utilizes radiofrequency or laser energy to purposely thrombose a vein by inducing endothelial injury to the superficial veins of the lower extremities. 3 Although EVA is a minimally invasive procedure, there is a risk of thrombotic complications, including EHIT, DVT, and a risk of subsequent PE. 4 EVA poses a unique risk of clinically induced thrombus propagating to or past the saphenofemoral or saphenopopliteal junction and into the deep system, termed EHIT. Kabnick et al 11 first introduced the term EHIT in 2005 to represent these post-EVA findings. A four-stage classification system was also established depending on the involvement of the deep system, with stage 1 having no involvement with the deep system (thrombus to or near the level of the junction) and stage 4 resulting in occlusion of the common femoral or popliteal vein.11,12
Multiple studies that assessed patients who had undergone EVA procedures discovered thrombotic complications.4,13–18 Reported incidence of EHIT in literature widely ranges from 0% to 8% post-EVA.3,5 The incidence of DVT and PE post-EVA has also been reported to range from 0.5% to 7.7% and 0.2% to 0.3%, respectively.2,4 A study conducted by Ryer et al, 19 including 488 patients who underwent a RFA procedure, detected EHIT in approximately 2% post-RFA procedure. Another retrospective study by Koramaz et al 20 reviewed records of 189 patients who underwent an EVLA procedure and found EHIT in approximately 1.6% of patients and no finding of DVT. Furthermore, a recent meta-analysis regarding the incidence of EHIT formation post-EVA pooled data from 52 studies and found that thrombotic events were uncommon findings. Of the 52 studies, 25 studies that yielded data on EHIT Classes 2-4 and DVTs revealed deep venous thrombotic events in 1.7% of cases. 18 Additionally, data was pooled from 26 studies that yielded data on EHIT Classes 2-4 and found thrombotic events in 1.4% of cases. 18 Further analysis also found similar incidence of EHIT Classes 2-4 between RFA (1.2%) and EVLA (1%), when analyzed separately, and deep venous thrombotic events (EHIT Classes 2-4 and DVTs) in 1.4% and 1.3% of cases, respectively. 18 Moreover, the meta-analysis reviewed 29 studies that yielded data on PEs and discovered PEs in 0.1% of cases. 18 Overall, thrombotic complications following EVA are small but definite. Thus, postoperative duplex exams of the affected area are generally recommended 1 to 2 weeks post-EVA to rule out DVT and EHIT.15,21 Early detection of thrombus is important for early treatment and to decrease the risk of developing life-threatening complications such as PE, which has a mortality rate of 11% to 23% if left untreated. 6
Etiology and Risk Factors
The etiology of EHIT is not well known, and no firm evidence has been published to guide its treatment. 18 Although there is a need for further research to fully understand EHIT, there are some known risk factors. The risk of developing EHIT or DVT after an EVA has been found to be greater in patients with previous history of DVT. 22 The same study also found superficial vein thrombus protrusion into the deep system, now referred to as EHIT, was more likely in patients who used aspirin, received treatment on their small saphenous vein (SSV), were male, or were in a hypercoagulable state. 22 Risk factors for EHIT have also been noted in literature to increase with age, prior history of clotting disorders, decreased distance from the site of ablation to the SFJ, and incorrect positioning of the catheter tip.3,10,12 Sadek et al 12 published findings that suggest that incidence of EHIT could be decreased by changing the standard treatment distance of the ablation site from SFJ to a distance from 2 cm to equal to or greater than 2.5 cm. Further research conducted by Shutze et al 23 found that the use of a water-specific laser fiber wavelength (1470 nm) has been shown to reduce the risk of thrombotic complications, such as EHIT, when compared to a hemoglobin-specific wavelength (810 nm). Shutze et al 23 also found that higher CEAP classification, vein diameter of greater than 7.5 mm, and simultaneous phlebectomy at the time of EVA are associated with increased risk of EHIT after EVLA.
Signs and Symptoms
Typical symptoms of thrombi in the deep veins include pain, heaviness, and cramps, which may slowly progress over several days. 24 DVT symptoms may suddenly accelerate and result in edema and discoloration of the limb. 24 Conversely, EHIT is typically asymptomatic. A recent study reported 87% of patients diagnosed with EHIT were asymptomatic, with the other 10% reporting pain and 2.9% reporting swelling. 25 This further dictates the importance of postoperative sonographic evaluation of these patients to rule out EHIT. Signs that thrombus has progressed to PE include elevation of pulmonary artery systolic pressure, chest pain, shortness of breath, syncope, and/or dry cough. 26 Depending on the size and severity of the PE, symptoms can range from mild to massive. 26 A PE is considered minor if it obstructs less than 50% of pulmonary blood flow. 26 A minor PE often does not have any clinical manifestations. Massive PEs occur when more than 50% of the pulmonary circulation is interrupted, resulting in various clinical symptoms of cardiac distress and the potential for cardiac arrest. 26
Sonography
Veins have weaker musculature and less elastic walls than their arterial counterparts. As a result, a normal vein will completely collapse when compressed by the transducer. When acute thrombus is visualized, the vein appears distended, shows partial or no compressibility and vascular flow is typically not noted in color or spectral Doppler. 27 On the other hand, when chronic thrombus is visualized, the vein is typically narrow or irregularly shaped, contains thrombus in the intraluminal space that is well attached to the vessel, and demonstrates partial compressibility. 27 According to American College of Radiology guidelines, compression, color Doppler, and spectral Doppler (with augmentation) should all be included in a venous duplex to successfully rule out thrombus. 27
EHIT presents with different sonographic appearance depending on which class it belongs to (Figure 3). 10 Class 1 EHIT describes thrombus that extends from the superficial vein to an area within close proximity to the SFJ but does not pass the junction. 12 Class 2 EHIT extends beyond the SFJ and occupies less than 50% of the vessel diameter. 12 Class 3 EHIT extends beyond the SFJ and occupies more than 50% of the vessel diameter. 12 Class 4 EHIT describes totally occlusive thrombus extending from the superficial vein to the deep vein. 12
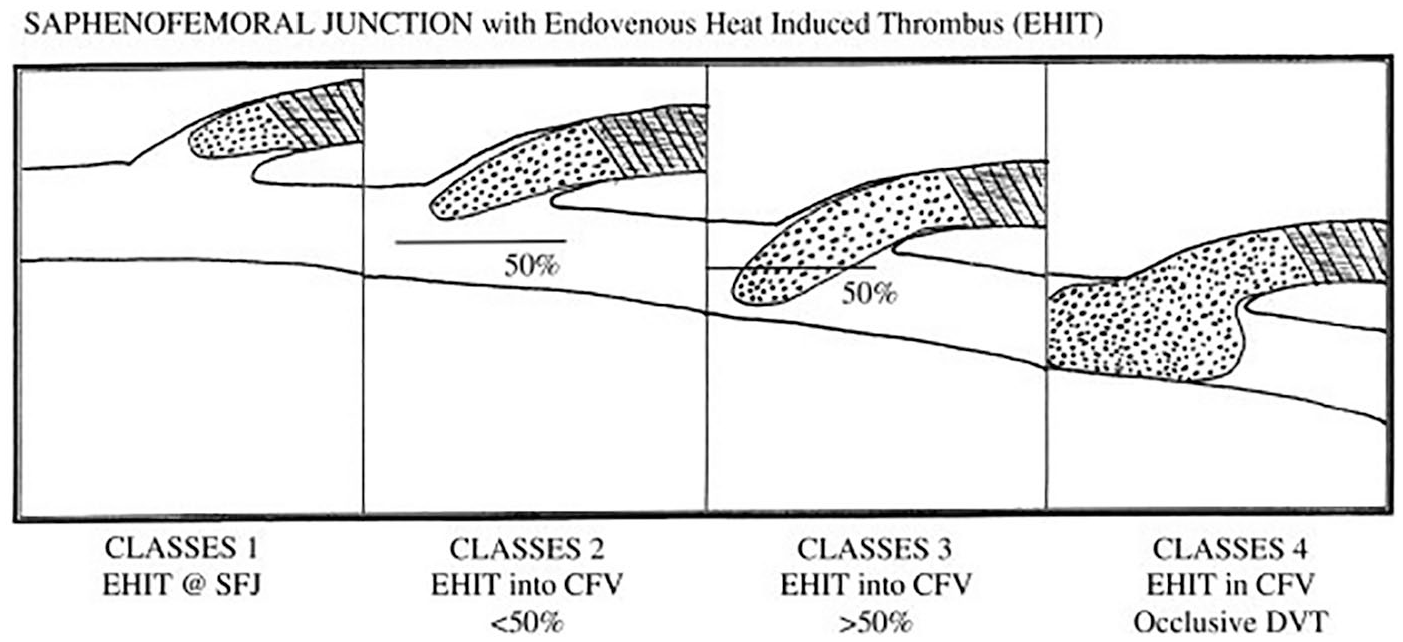
Schematic drawing of Classes 1 through 4 endovenous heat-induced thrombosis. Reprinted with permission from Elsevier. Frasier K, Latessa V: Minimally invasive vein therapy and treatment options for endovenous heat-induced thrombus. J Vasc Nurs 2008;26(2):p 5. 10
Other Imaging and Lab Values
Historically, contrast venography was widely used before sonography and is currently still regarded as the gold standard imaging technique for the diagnosis of thrombus. 27 However, venography is an invasive procedure that requires specially trained professionals and the use of large amounts of intravenous contrast. 27 Advantages of using sonography for the diagnosis of thrombus include efficiency, noninvasive method, cost efficiency, absence of ionizing radiation, and ability to be performed bedside. 27 Venous sonography is very accurate for the diagnosis of proximal DVT, with a sensitivity and specificity near 95%. 28
In addition to venography, other imaging tests to detect thrombus include CT and magnetic resonance imaging (MRI). 27 Although both CT and MRI have a sensitivity and specificity greater than 90%, these modalities are rarely used as they expose patients to ionizing radiation, are costly, and lack the portability of ultrasound. 28 Additionally, CTPA may be helpful in diagnosing thrombus once it has become a PE. 27 An alternative to imaging, a blood test for a protein called D-dimer, which is released as part of the blood clotting and breakdown process, can be used to test for the presence of thrombus. 29 However, such tests tend to have a high sensitivity but substantially low specificity. 27
Outcomes
Treatments for thrombus, as listed by the Centers for Disease Control and Prevention (CDC), are dependent on location and severity and include the following: anticoagulants, thrombolytics, IVC filters, and thrombectomy. 30 Anticoagulants, commonly referred to as blood thinners, include medications such as Heparin or Warfarin. These drugs reduce the coagulability of blood, preventing the thrombus from increasing in size, but they also put the patient at greater risk of bleeding. 30 Since the risk for bleeding with thrombolytics is much higher than anticoagulants, these drugs are reserved for cases of severe DVT. 30 IVC filters can be placed in the IVC to prevent mobile thrombus from becoming PEs when anticoagulation therapy and thrombolytics are ineffective. 31 Thrombectomy, or the surgical removal of a thrombus, may be necessary in some cases of thrombus and/or PE.
In patients with a first unprovoked DVT or PE and high risk of bleeding, the American Academy of Chest Physicians recommends anticoagulation therapy be given for 3 months but should be extended without a scheduled stop date in patients with a low or moderate risk of bleeding. 32 However, anticoagulants should stop after 3 months of therapy in patients with an acute, proximal DVT provoked by surgery rather than shorter or longer treatment courses. 32 Currently, management and treatment of EHIT vary depending on physician preference because no firm evidence has been published to guide treatment. Initial published reports recommended thrombectomy; however, recent literature has moved toward anticoagulation as the preferred treatment option, with sonogram follow-up in many cases. 10 A recent cohort study by Lawrence et al 33 recommends treating Class 1 EHIT with either observation or anticoagulation and anticoagulation therapy alone for EHIT Classes 2-4. Knipp et al 34 recommends treating EHIT patients with anticoagulation for 1 week, followed by a repeat venous duplex ultrasound to determine the need for further therapy. A study by Ryer et al 19 found EHIT progression in 13% of patients managed with observation alone and thus suggests anticoagulation for all cases of EHIT. Despite the variance in the method of management, most reports agree anticoagulation, in the form of low molecular weight heparin, is sufficient for most instances of EHIT.10,18
Conclusion
Although EVA is a minimally invasive procedure, there is a small but definite risk of thrombotic complications, including EHIT, DVT, and a subsequent risk of PE. 4 With EHIT clinically presenting as asymptomatic, sonography plays an important role in postoperative surveillance to provide early detection and intervention if needed. While venography is considered the imaging gold standard for diagnosing thrombus, sonography continues to be a great choice for imaging post-EVA patients as it is noninvasive, cost-efficient and can be performed bedside. Sonography is both sensitive and specific for the detection of thrombus, at around 95% sensitivity and specificity. 28 Although management and treatment of EHIT vary depending on physician preference, many reports agree low molecular weight heparin is sufficient for most instances of EHIT.10,18 With early sonographic detection and subsequent treatment, patients can expect a normal recovery with little to no symptoms.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.