
Abstract
A pregnancy developing in the cornu is rare and accounts for less than 1% to 4% of ectopic pregnancies. This case describes a cornual heterotopic gestation occurring as a first pregnancy where both gestational sacs were anembryonic. Presented are subsequent 2D and 3D sonographic findings with laboratory changes following treatment in an ectopic systemic methotrexate protocol.
Heterotopic pregnancy occurs when an intrauterine and extrauterine pregnancy occur simultaneously. The incidence was estimated to be 1:30,000 in 1948. Current incidences of 1:1285–3800 spontaneous fertilizations have been published.1–4 With increasing assisted reproductive technologies (ART), the incidence may be as high as 1:100 in women undergoing in vitro fertilization and embryo transfer (IVF-ET).5–9 A pregnancy developing in the cornu is rare and accounts for less than 1% to 4% of ectopic pregnancies.7,10 Cornual pregnancies are of increased concern because of the risk for catastrophic hemorrhage and maternal morbidity, often because of a delay in definitive diagnosis. Anembryonic gestation is diagnosed when a gestational sac is identified measuring greater than 20 mm without evidence of a yolk sac or embryo. 11 This case describes a cornual heterotopic gestation where both gestational sacs were anembryonic. This is unusual in that this occurred as a first pregnancy with no medications involved. Presented are subsequent sonographic findings with laboratory changes following treatment.
Case Report
A woman in her early 20s, gravida 1, para 0, at 8 weeks 3 days gestation estimated from a certain last menstrual period, was referred for a sonographic examination to confirm and date an intrauterine pregnancy. The patient’s past medical history was unremarkable, with no pain or vaginal bleeding at the time of the examination.
An endovaginal sonography examination was performed with a Philips IU22 (Philips Medical Systems, Bothell, Washington), using a 3- to 9-MHz vaginal transducer. A 2D standard examination of the uterus and adnexa and 3D volume sweeps using a sagittally acquired plane were taken of both areas. At the anticipated eight weeks three days menstrual age, one would expect to see an intrauterine gestational sac measuring approximately 29 mm, good visualization of an embryo with heart motion, an amniotic membrane surrounding the embryo, and a yolk sac between the amnion and the chorion.11–13
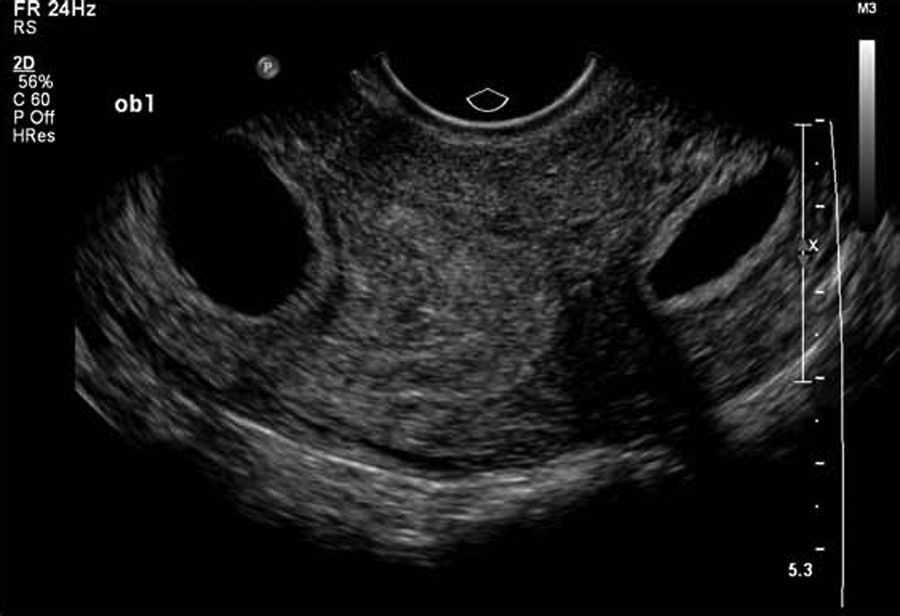
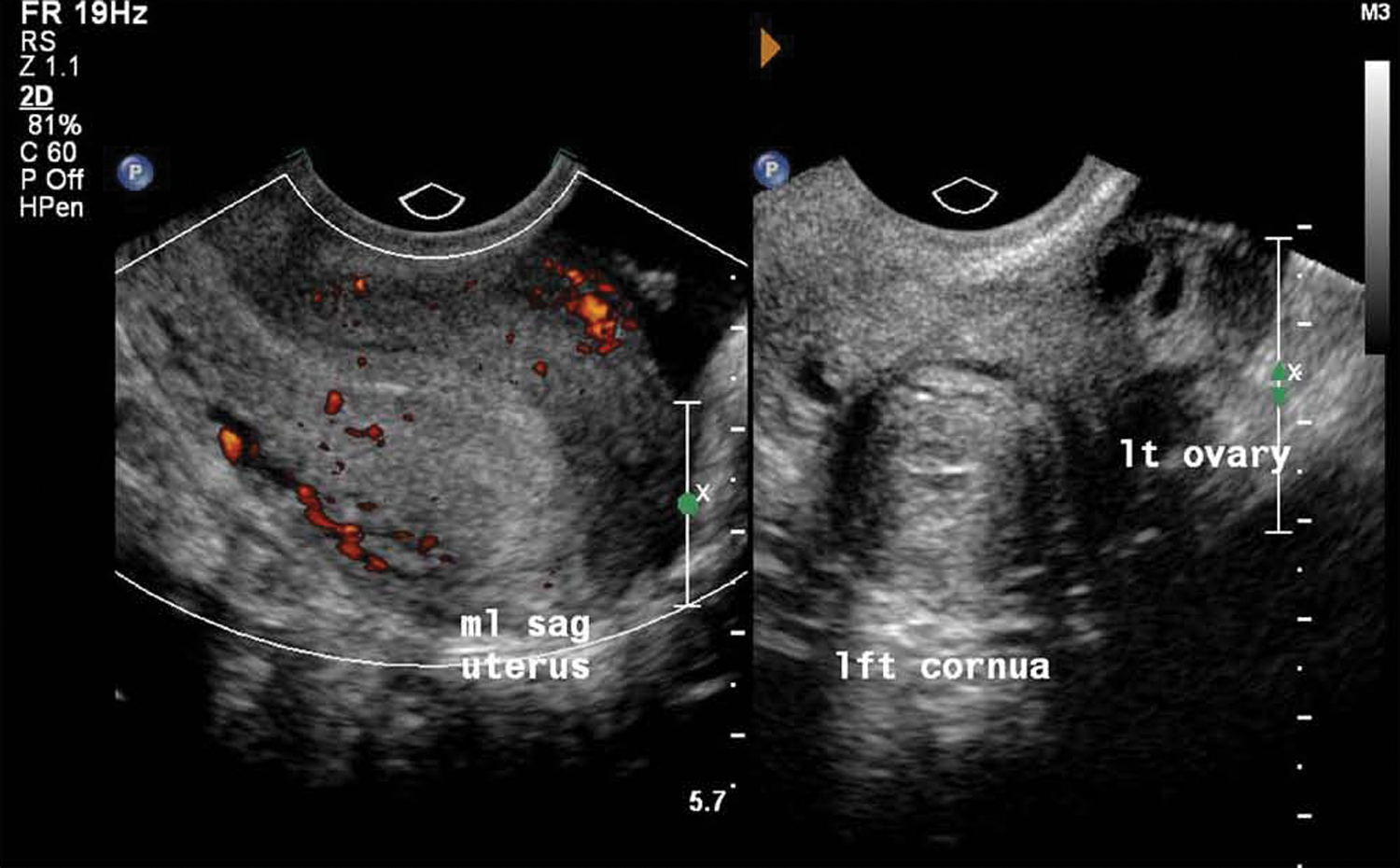
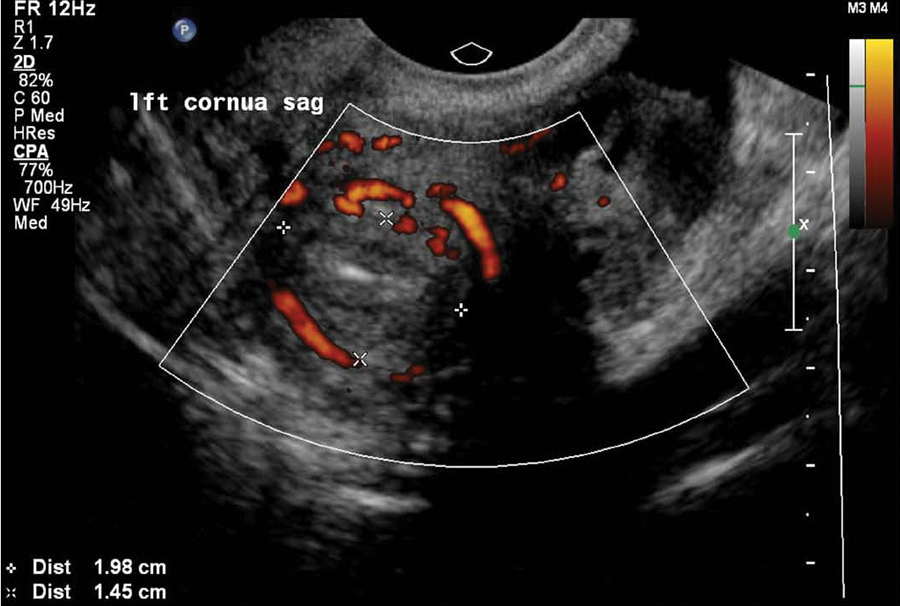
The sonography findings revealed a retroverted retroflexed uterus of normal size and contour. Both ovaries were well visualized and appeared normal in size and echo pattern. A well-circumscribed hypoechoic round structure consistent with an intrauterine gestational sac seen within the endometrial cavity, measuring 2.12 × 2.19 cm, was surrounded by a double decidual reaction (Figure 1). A circumferential hyperechoic rim surrounding the entire area with diffuse peripheral Doppler color was noted, thought to represent trophoblastic vascular flow. 2D and 3D volume reconstruction confirmed no evidence of a yolk sac or embryo (Figure 2A,B). A second oblong, more irregular-shaped structure seen within the left cornua, measuring 1.95 × 0.8 × 1.64 cm, also exhibited an echogenic rim and diffuse circumferential Doppler color flow—findings representative of another gestational sac. 3D reconstruction was again used to confirm that there was no evidence of a yolk sac or embryo within this structure (Figures 3 and 4). An oblique view of both the mid-uterine segment and the left cornua demonstrated the presence of concomitant sacs with a normal-appearing left ovary (Figures 5 and 6). Findings are consistent with a cornual heterotopic double anembryonic gestation.
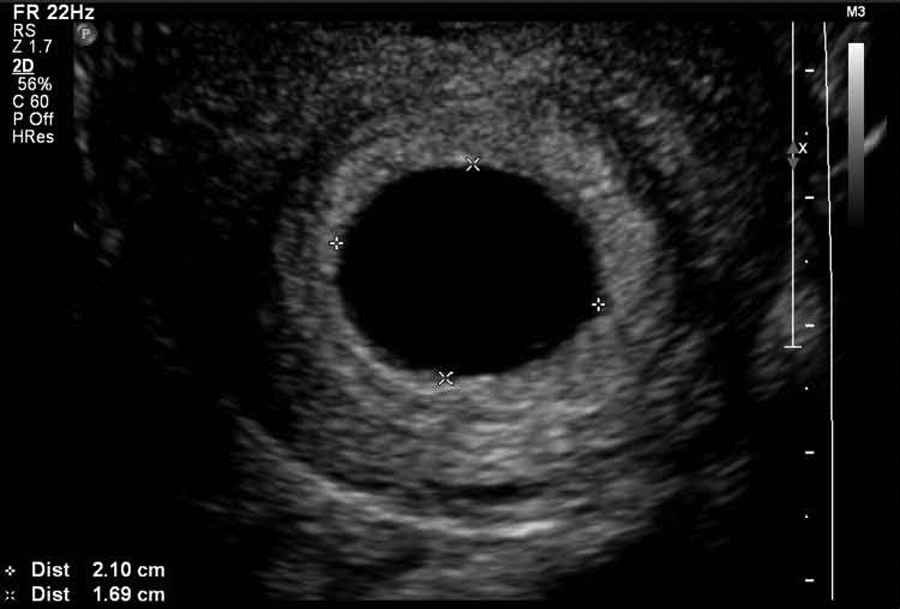
2D image of the intrauterine gestational sac reveals a well-circumscribed anechoic structure with no evidence of an embryo or yolk sac.
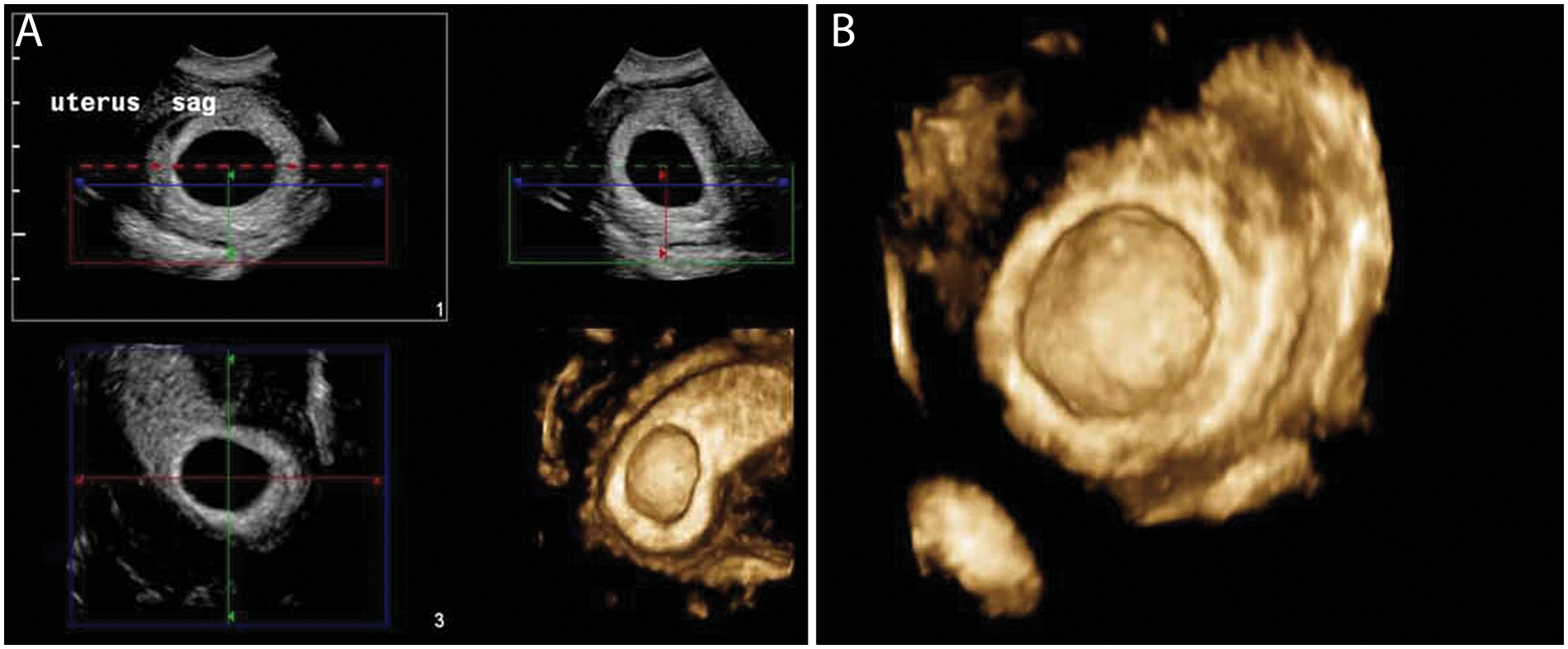
(A, B) 3D volume set and rendered image of the endometrial cavity reveals smooth luminal contour and no evidence of an embryo or yolk sac within the gestational sac.
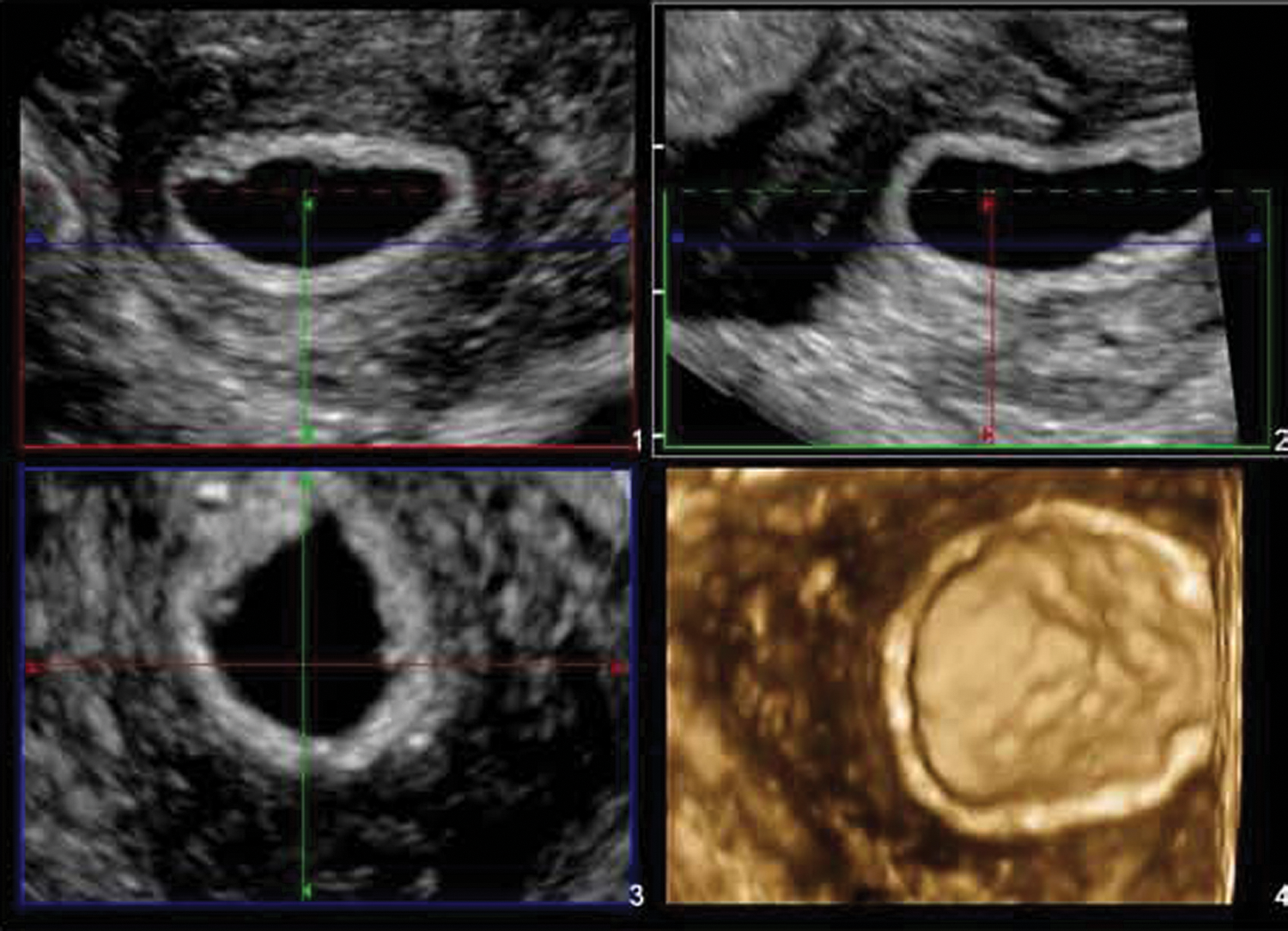
3D volume set of left cornua reveals smooth luminal contour and no evidence of an embryo or yolk sac within the ectopic gestational sac.
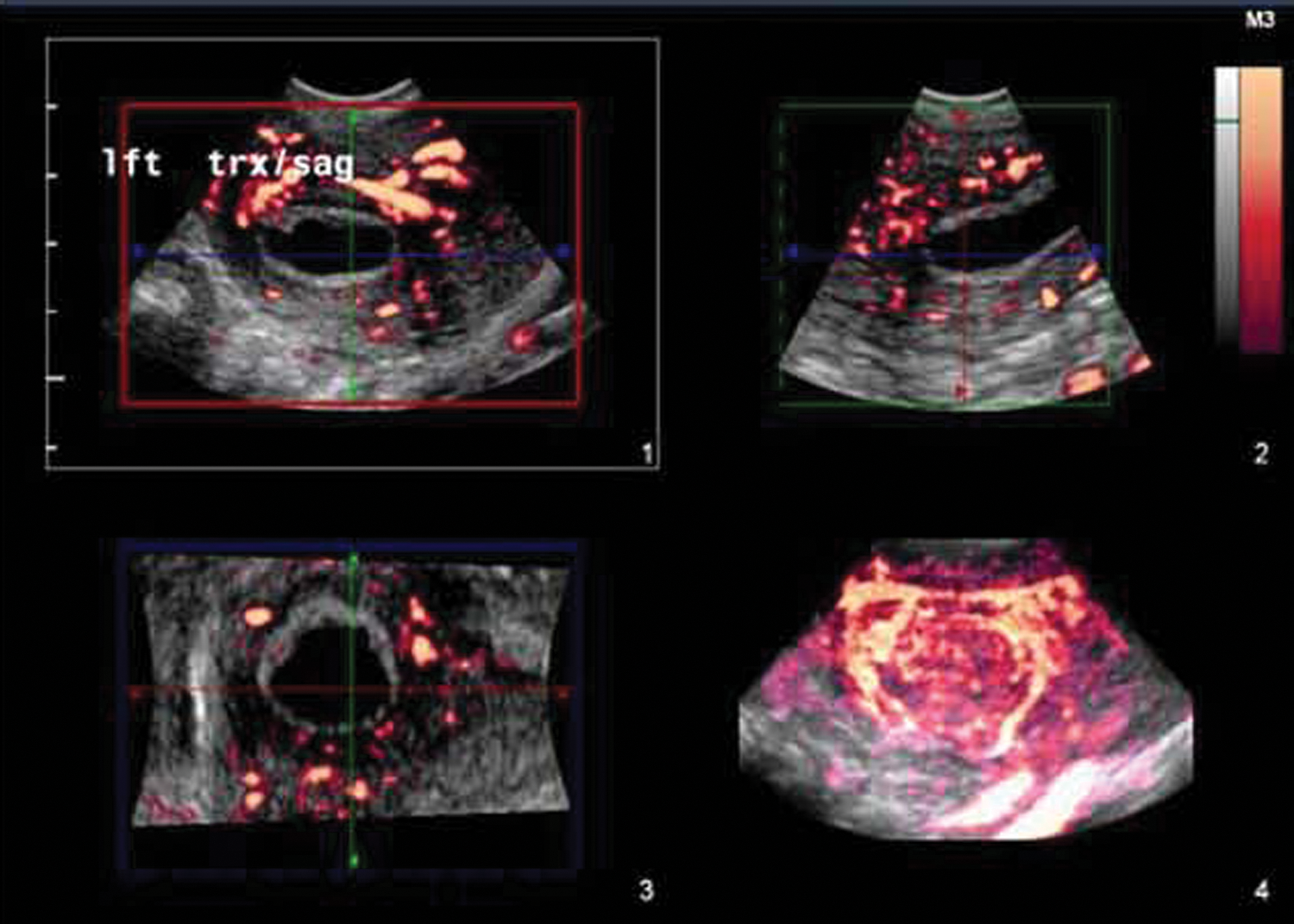
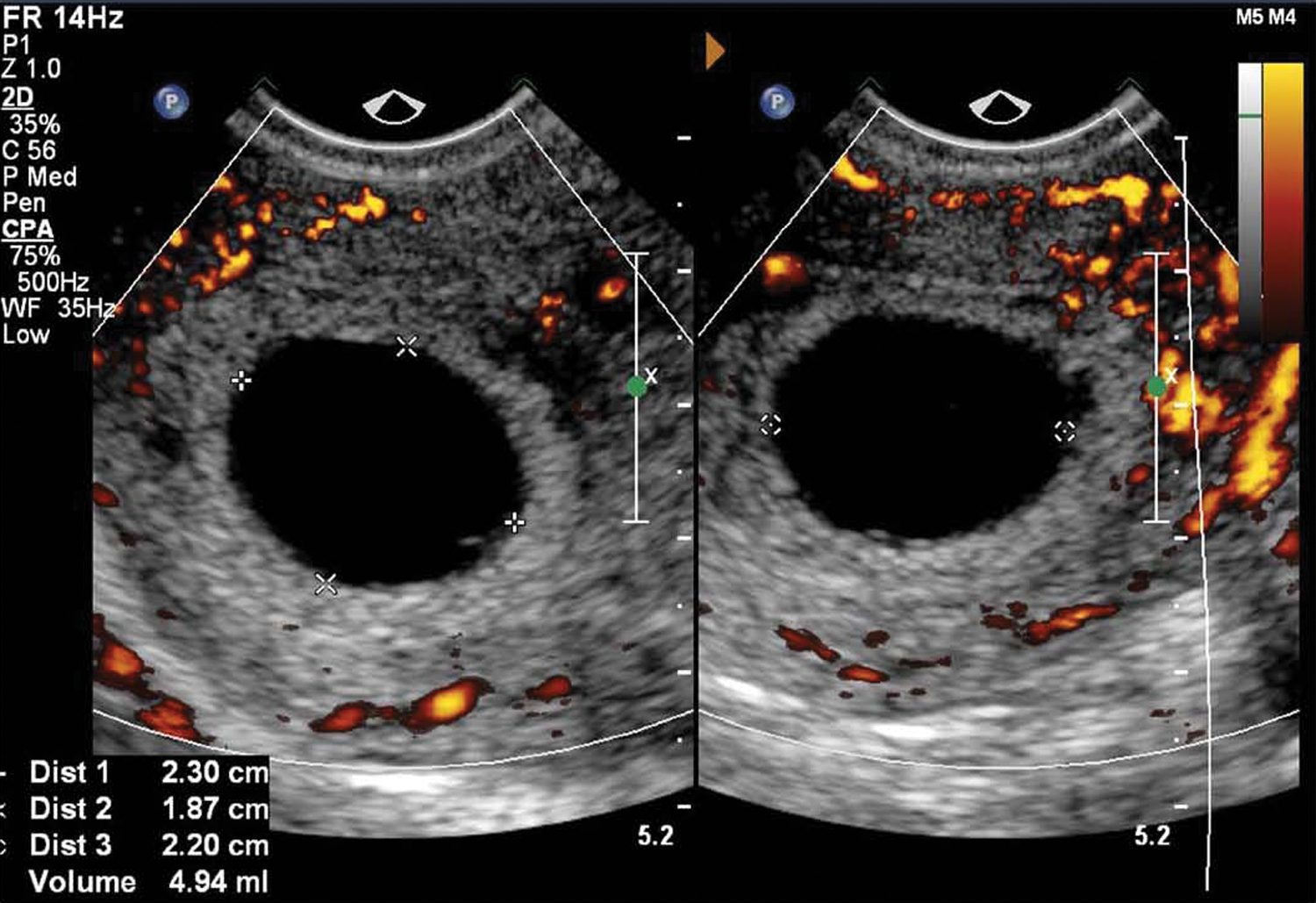
3D volume set of the ectopic gestational sac with color Doppler reveals clear decidual response and marked peritrophoblastic flow.
2D oblique plane through the mid-uterine segment and left cornua reveals both gestational sacs.
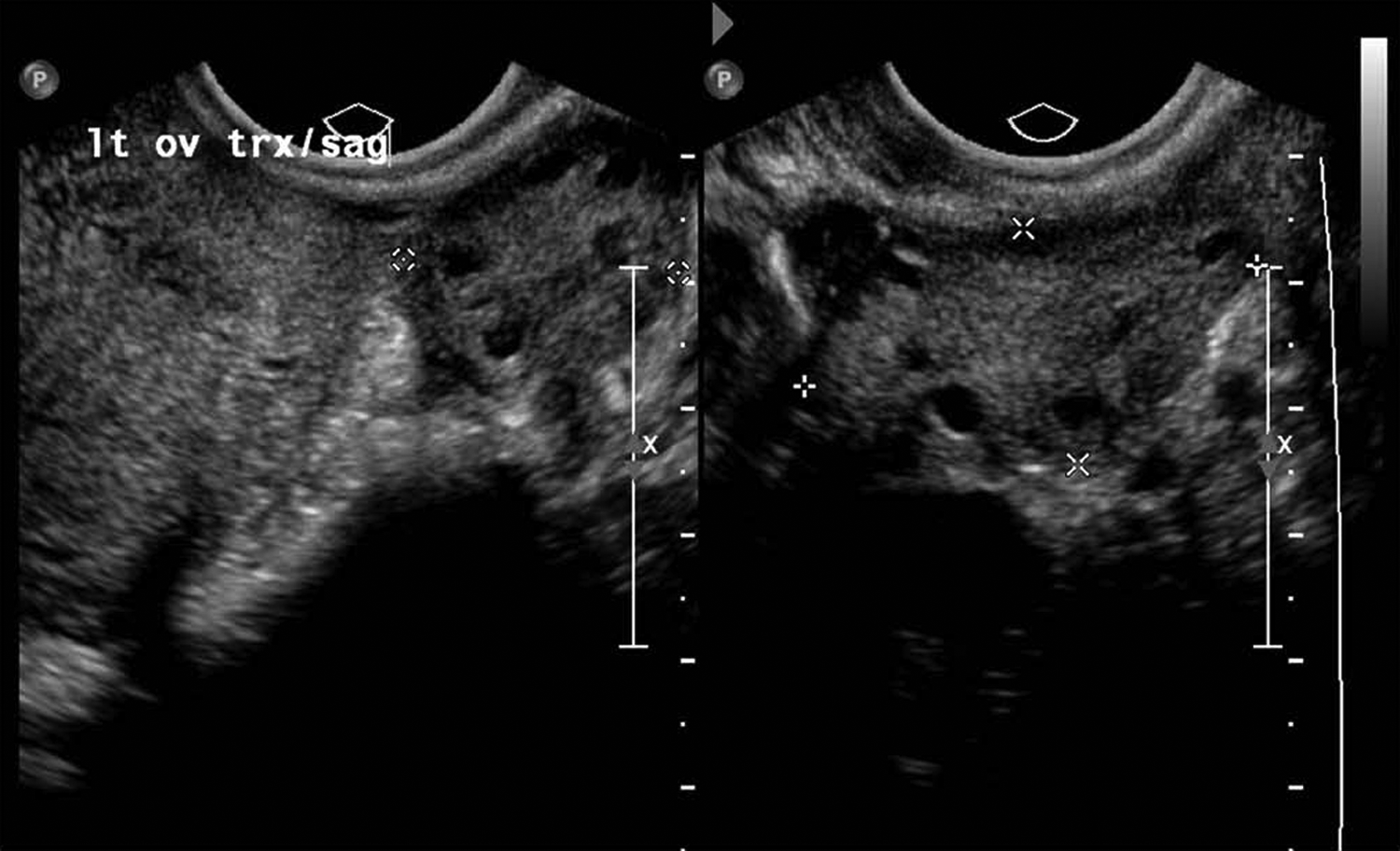
Transverse and sagittal 2D images of the left adnexa reveal a normal left ovary.
The patient was transferred to the Obstetric Testing and Triage clinic for evaluation and counseling. Further clinical assessment revealed a quantitative β–human chorionic gonadotropin (β-hCG) of 41,016 mIU/mL. She was then placed on an ectopic systemic methotrexate treatment protocol.7,14,15 The patient received methotrexate, 50 mg/m2, and returned for a repeat physical examination and laboratory evaluation 96 hours later per the clinical protocol. At that time, her quantitative β-hCG was 35,047 mIU/mL. The patient was evaluated 72 hours later, per protocol, and her quantitative β-hCG continued to decline to 22,739 mIU/mL.
A follow-up sonographic examination revealed the continued presence of an intrauterine gestational sac measuring 2.30 × 2.20 × 1.87 cm and a left cornual gestational sac measuring 2.22 × 0.96 × 2.03 cm, both of which demonstrated a small regression in volume. In addition, the deciduae surrounding both gestational sacs appeared mottled and more irregular, consistent with tissue degeneration, presumed secondary to the methotrexate treatment (Figures 7 and 8). The patient continued clinical surveillance per protocol and tolerated the treatment very well without side effects. Two weeks after the single treatment, the β-hCG was 129 mIU/mL, declining further to 20 mIU/mL an additional week later. At that time, a sonography examination revealed complete absence of the intrauterine gestational sac. The cornual gestational sac was more collapsed; however, there continued to be moderate peripheral hypervascularity (Figures 9 and 10). One month later, seven weeks after receiving methotrexate, both sacs were completely resolved, and her β-hCG was less than 1 mIU/mL.
2D images of the intrauterine gestation sac on day 7 reveal changing mottled appearance of surrounding deciduae following methotrexate treatment‥
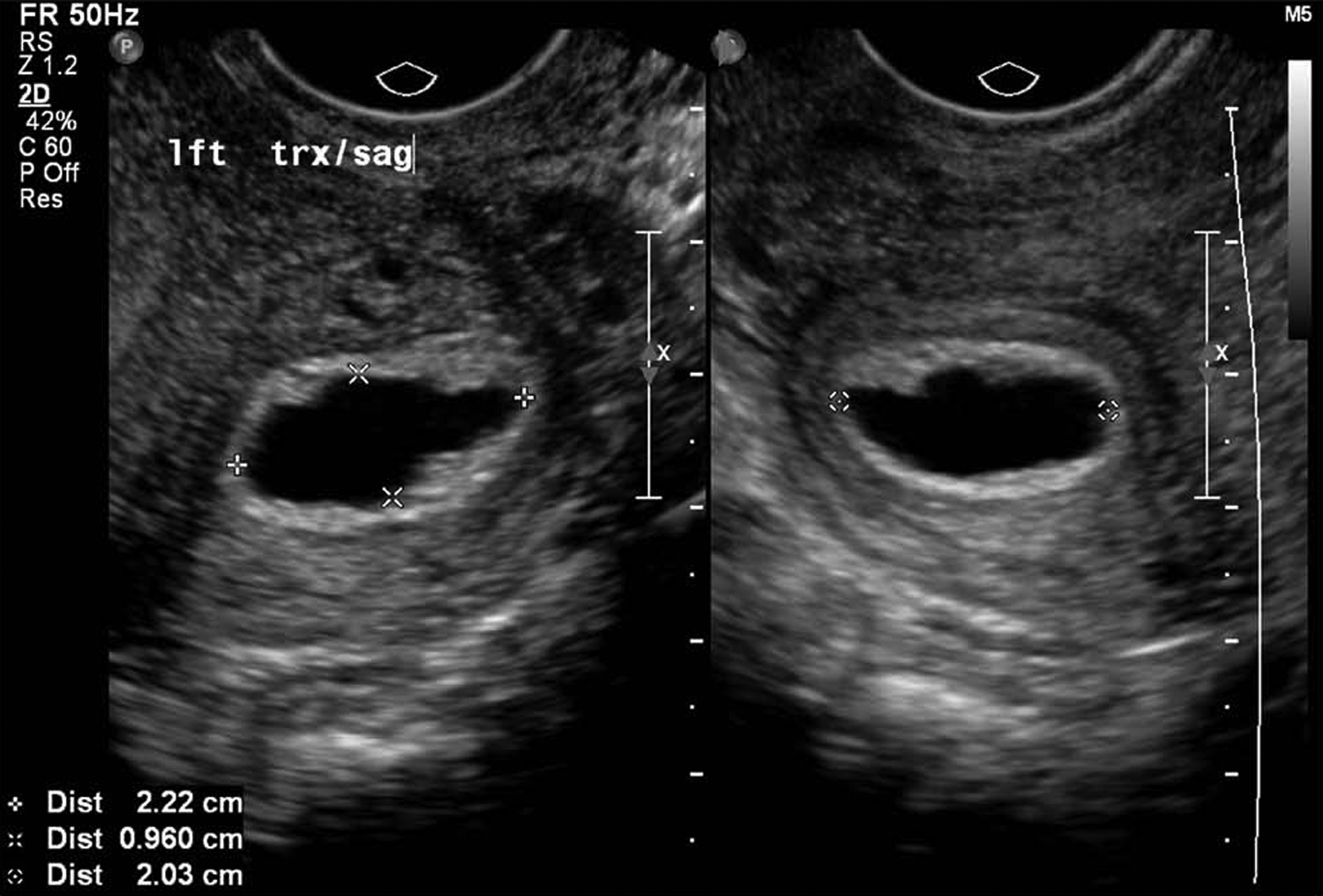
2D images of the cornual gestation sac on day 7 reveal changing mottled appearance of surrounding deciduae following methotrexate treatment.
2D images of sagittal uterus and transverse cornua on week 3 reveal complete resolution of the intrauterine gestational sac and a collapsed cornual gestational sac.
2D sagittal view with power Doppler imaging of the collapsing corneal gestational sac reveals a continued peripheral circumferential hypervascular pattern.
Discussion
An anembryonic gestation occurs when a fertilized egg implants into the uterine wall, but the embryo does not develop. It is sonographically diagnosed when a gestational sac is identified measuring greater than 20 mm but without evidence of a yolk sac or embryo. Also, the extrapolated growth rate for an anembryonic gestational sac is also slower, approximately 0.70 mm/d, as compared with 1.13 mm/d in the normal intrauterine pregnancy gestational sac.12,13
Heterotopic pregnancy occurs when an intrauterine and extrauterine pregnancy occur simultaneously. It has historically been reported as a rare event, but more recent publications consider it to be more prevalent. The incidence estimated in a 1948 publication was 1 in 30,000. 1 Contemporary incidences of heterotopic pregnancies occurring spontaneously range from 1 in 3800 for spontaneous fertilizations in 2000 and 2007 to 1 in 1285 pregnancies.2–4 With increasing utilization of ART, the reported incidence of heterotopic pregnancies seemingly approaches 1 in 100 in women completing multiple embryo transfer.5–8 Although it is uncertain if ART is a factor, reasons offered for an increase in heterotopic pregnancy include ovulation-inducing protocols that may result in more than one ovulated oocyte and alterations in tubal transport mechanism possibly affected by absolute and relative concentrations of estrogen and progesterone levels.16,17 There is an association of highest rates of heterotopic pregnancy when more than five embryos have been transferred to the uterus. 7 Other predisposing risks may include tubal damage with history of pelvic inflammatory disease, postinfection scarring of tubal pregnancies, tubal sterilization procedure history, or infertility.4,9,18–20
A cornual location of an ectopic is rare and accounts for less than 1% to 4% of the ectopic pregnancies.7,21 The term is often used interchangeably with interstitial pregnancy. Cornual pregnancies are of increased concern because of the risk for catastrophic hemorrhage and maternal morbidity. This can occur if an early diagnosis is not made, especially with subsequent rupture. Cornual pregnancy is sonographically identified when the gestational sac is surrounded by a thin rim (<5 mm) of cornual myometrium and is more than 1 cm from the lateral wall of the endometrial cavity. 21
Clinically, the diagnosis of a cornual ectopic pregnancy is made later rather than earlier, presumably due to the location and absence of premonitory symptoms such as pain. In addition, serum β-hCG levels resulting from two trophoblastic sites may confound the ability to fully employ a discriminatory hCG level, a critical parameter in typical diagnostic algorithms for eccyesis. 22 Unlike in the case being described, the masking effect of dual hCG sources would be more problematic in earlier-presenting pregnancies, particularly if the rate of increase of hCG was seemingly within clinical expectations. In this case, the initial β-hCG was 41,016 mIU/mL, and the results of the sonography examination superseded the implications of the glycoprotein level.
Medical management requires laboratory assessment with serial sonography surveillance to document morphologic changes of eccyesis. Since the onset of methotrexate treatment in the presence of cornual ectopic pregnancies, there has been limited disclosure in the literature. 23 The publication by Lau and Tulandi 7 in 1999 represents an early source in the ongoing management of interstitial ectopic pregnancies. There is a comparable paucity of data for medical or combined medical and surgical treatment strategies for true cervical ectopic pregnancies, another relatively rare site for eccyesis. 24 Data from serial sonography monitoring suggest a disparate pattern of resolution of anatomic sites of each anembryonic ectopic pregnancy. This protracted response has been previously described in a nonpublished ectopic pregnancy case presented at the University of New Mexico Health Sciences Center, where a cornual ectopic pregnancy was diagnosed at seven weeks. The embryo was visualized without heart motion and was treated with methotrexate. Serial β-hCG values were followed from an intercurrent level of more than 7000 mIU/ml to normal, less than 5 mIU/mL, without maternal symptoms; however, the embryonic tissue did not resolve over the same monitoring period. After documenting lack of resolution over two months, it was recommended that the patient have the ectopic pregnancy electively surgically removed. This was done with removal of the gestation sac and embryo through a cornual incision. In this case, the sonography data seem to confirm a differential response to the methotrexate injection.
Conclusion
This case reports on a heterotopic pregnancy conceived spontaneously as a first intended pregnancy in a woman without any identified risk factors not using fertility-promoting medication. The diagnosis was made incidentally during an initial visit for establishing prenatal care. Both pregnancies were anembryonic. Based on existing clinical data, the decision was made to treat her conservatively with methotrexate. The serial monitoring provided by sonography examinations suggested a differential rate of involution to each pregnancy site, with the intrauterine sac resolving sooner. The chronologic delay in involution of the gestational sac associated with the interstitial site had been noted before in an unpublished observation at this institution. In that prior case, a moribund fetus was present within the interstitially located gestational sac, and neither it nor the sac disappeared during methotrexate therapy, despite restoration of normal, nonpregnant hCG levels. This distinction may have implications for the medical versus clinical management of interstitial pregnancies, which are more likely to be encountered than true heterotopic pregnancy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.