
Abstract
Objective:
Musculoskeletal sonography (MSKS) is increasingly being used in the setting of juvenile idiopathic arthritis (JIA). The purpose of this narrative review was to describe the role of sonography in JIA and outline strategies for operators of pediatric MSKS.
Methods:
A literature review through multiple medical databases was conducted by restricting the search to medical subject headings (MeSH). Peer-reviewed English-language articles from 2007 to 2018 were included, which focused the on common sonographic findings of JIA.
Results:
Twenty-six articles were selected for inclusion in the study after a complete reading. Many studies aimed to address the validity of sonographic techniques in the assessment of JIA, but few studies discussed the specific sonographic appearances of JIA, scanning pitfalls, and appropriate imaging techniques.
Conclusion:
MSKS reveals subclinical manifestations of arthropathy, but the true value of detecting subclinical disease is not well understood. MSKS is limited in the evaluation of articular cartilage thinning and bony erosions. Responsiveness of MSKS in JIA remains to be formally assessed with higher quality studies.
Juvenile idiopathic arthritis (JIA) describes a spectrum of pediatric (<16 years) arthritides of unknown origin. Classifications include systemic, oligoarticular, rheumatoid factor–positive JIA, and more; however, describing the types of arthritis is beyond the scope of this article. JIA is considered an acquired autoinflammatory disease 1 found in children and affecting the joints in a global distribution. Patient demographics are difficult to report given the heterogeneity of the disease and contention around the subtypes. Children generally present with joint swelling, joint stiffness, fever, or limping pain. 2
JIA is well described in the literature from a clinician’s perspective, concerning the diagnosis and management of the disease; however, studies specifically analyzing the imaging characteristics of JIA and the role/value of sonography in this patient population appear to be lacking. The purpose of this narrative review is to address this gap in the literature and offer practical suggestions to musculoskeletal sonography (MSKS) operators when evaluating for JIA.
As a nonionizing, high-resolution imaging modality, MSKS is uniquely positioned as an excellent imaging tool in the pediatric JIA population. As such, it has seen widespread use, primarily for the evaluation of effusion and synovial hypertrophy. Although the diagnosis of JIA is typically clinical, the detection of subclinical JIA is especially important given that early aggressive medical intervention has been seen to alter the disease process to improve long-term outcomes. 2
Sonography is considered especially useful in assessing joints like the ankle, which are anatomically complex and therefore difficult to examine clinically. 3 MSKS adds value by assessing for joint effusion, tenosynovitis, and synovial hypertrophy and hyperemia. The presence or absence of these findings may indicate active disease versus JIA in remission. Sonography may also reveal related thinning of the articular cartilage and bony erosions, but these findings are less often appreciated. 4
In this narrative review article, a synthesis is provided of the current literature available on the role of sonography in JIA, accompanied by clinical images and useful tips and tricks aimed at the pediatric MSKS operator.
Methods
This study represents a narrative descriptive review of the literature surrounding the role of sonography in JIA. Search engines used included PubMed, Google Scholar, and ScienceDirect. English-language peer-reviewed articles from 2007 to 2018 were included in the review. Articles were included that focused on sonography in JIA and its imaging characteristics. Literature reviews and case studies/series were analyzed. The search was limited to studies with the Medical Subject Headings (MeSH) of ultrasonography, juvenile idiopathic arthritis, doppler, and synovitis. One author participated in the screening process, and both authors participated in full-text review. In the present review, it was decided not to include the dated terms for JIA (juvenile rheumatoid arthritis, juvenile chronic arthritis). A flowchart of the article selection is included in Figure 1.
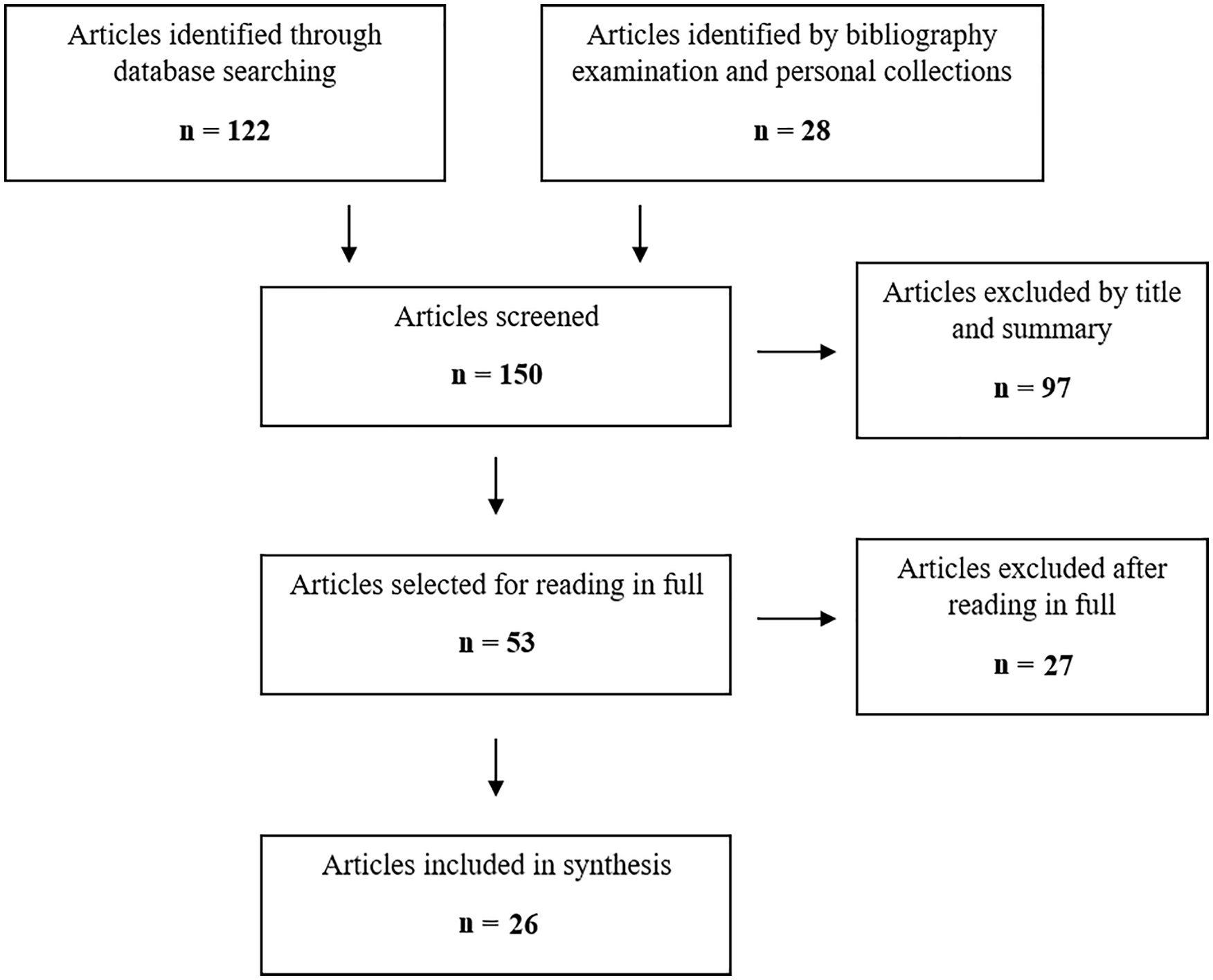
Flow diagram of review system and selection of sources.
All sonographic images included in the present review were retrieved from the authors’ research database using the ISYS Search software (Lexmark Enterprise Software LLC, Lenexa, KS, USA), which contains only fully anonymized data. All images in this database were acquired by registered sonographers at this facility using either a Philips iU22 (Philips Health Systems, Bothell, WA, USA) or Toshiba XG ultrasound machine (Toshiba Medical, Tampa, FL, USA).
Results
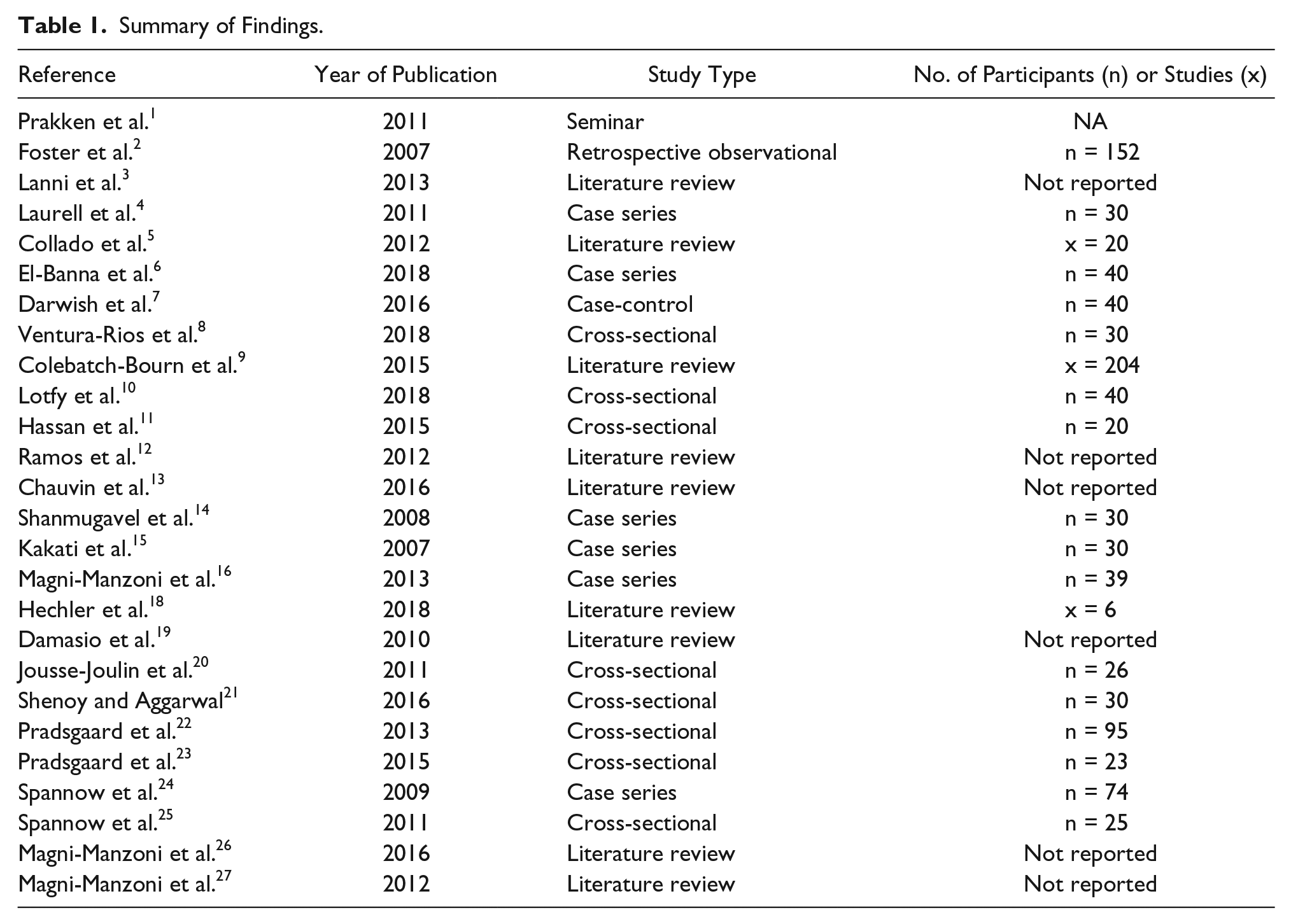
In total, 122 articles were identified through database searching, and 28 were identified by examination of the article bibliographies and from personal collections. Of 150 articles screened by title and summary abstract, 97 were excluded. The most common reasons for articles being excluded at this stage were focus of magnetic resonance imaging (MRI) versus sonography for diagnosis of JIA, focus on the use of novel sonographic techniques (quantitative ultrasound) in JIA, and focus on the use of corticosteroid injections in patients with JIA. Fifty-three articles were selected for full-text review and 26 articles were included in the final qualitative synthesis (see Table 1). The included articles were selected based on their relevance to the research topic and quality of study design.
Summary of Findings.
MSKS has been shown to be superior to the clinical examination as it pertains to detecting early signs of JIA.5–8 In one study in which 1664 joints of 32 patients were assessed both clinically and with sonography, sonographic imaging revealed synovitis in 86 clinically normal joints. The same study also reports interobserver reliability scores of 83%, 84%, and 95% for the presence/absence of joint effusion, synovial hypertrophy and power Doppler signal, respectively. 4 Furthermore, the European League Against Rheumatism (EULAR)–Pediatric Rheumatology European Society (PReS) task force, after a structured review of 204 articles, concluded several points, including the following: (a) sonography and MRI are superior to clinical examination, (b) sonography/MRI may detect joint damage earlier than conventional radiography, and (c) sonography/MRI may detect inflammation in clinically inactive JIA. 9 Power Doppler is often reported to have excellent sensitivity to detect actively inflamed synovium10,11 and is an essential part of the sonographic assessment to assess for signs of active disease.
MSKS in the pediatric population has limitations due to the varying sonographic appearances of the developing skeleton. The high cartilage to bone ratio simulates effusion, and the presence of a vascularized epiphysis can easily be misinterpreted as synovial hyperemia. Furthermore, the irregular appearance of the ossification centers of bones in children may be mistaken for cortical erosions.3,12 As a result, the quality and effectiveness of MSKS in this population are highly operator dependent. This is also due, in part, to gaps in current knowledge regarding the normal sonographic appearance of the healthy growing pediatric skeleton. 13
In addition, sonography has limitations for accurately detecting evidence of degenerative disease, represented by the presence of bony erosions and thinning of articular cartilage.3,12 The authors were unable to locate any published works evaluating the ability of sonography to quantify synovial volume in JIA.
Although sonography has been validated in the literature in its ability to detect synovitis in JIA, few recent studies have assessed its responsiveness. Laurell et al. 4 demonstrated statistically significant decreases in talocrural synovial hypertrophy four weeks after therapeutic injection, and Shanmugavel et al. 14 indicated decrease in vascularity on power Doppler at two- and six-month follow-up examinations, but other studies either had mixed results 15 or were not recent enough to be included in this review.
One study by Magni-Manzoni et al. 16 followed children with sonographic evidence of subclinical JIA for two years and concluded that the sonographically detected synovial abnormalities did not predict a clinical flareup. This indicates that the true significance of subclinical disease detected by sonography is not well established and is indeed a contentious topic today. 17
There has been a recent interest in the role of sonography in detecting the involvement of the temporomandibular joint in JIA, 18 but there is a lack of high-quality studies on this topic.
Strategies
Improvements in sonographic imaging resolution over recent years have allowed for detailed evaluation of joints and tendons, especially in children, where high-frequency, high-resolution probes can be used routinely. In the subsequent sections, technical considerations for scanning JIA in children and imaging findings are explored.
Sonographer’s Notes
Albeit its many advantages, MSKS is very operator dependent, and scanning joints and tendons poses a unique challenge for the inexperienced scanner. MSKS operators should keep in mind that due to most pediatric patients’ small body habitus, it is easy to compress superficial structures in children. A light touch or the use of a standoff pad while scanning can prevent missing joint effusion, bursal inflammation, or even subtle synovial hypertrophy. As with most MSK scanning, contralateral comparison and dynamic evaluation are indispensable tools when the imaging findings are not immediately obvious. Those scanning patients with JIA should also remember this demographic often undergoes therapeutic injections, so discovering a hematoma is not unexpected. Also, ensure that a good clinical history is taken, as complex masses within the joint in the setting of a hemophiliac patient may be mistaken for sequelae of JIA. Finally, as with any type of pediatric scanning, the well-equipped sonographer will have appropriate implements on hand (toys, videos, etc.) to distract the child should it prove necessary to reduce motion artifact and to maintain the quality of the examination.
Imaging Findings
Joint effusion
The distension of the joint with excess intra-articular fluid is a nonspecific indicator of arthropathy and is often seen in active JIA. 19 Effusion is most often anechoic and collects around the joint with sharp margins, as seen in Figure 2. Noting this fact can help in distinguishing effusion from the anechoic appearance of articular cartilage in a child. If a complex intra-articular collection is identified, this can be differentiated from synovial hypertrophy by manual manipulation of the joint; an effusion should be mobile and demonstrate gravity dependency.
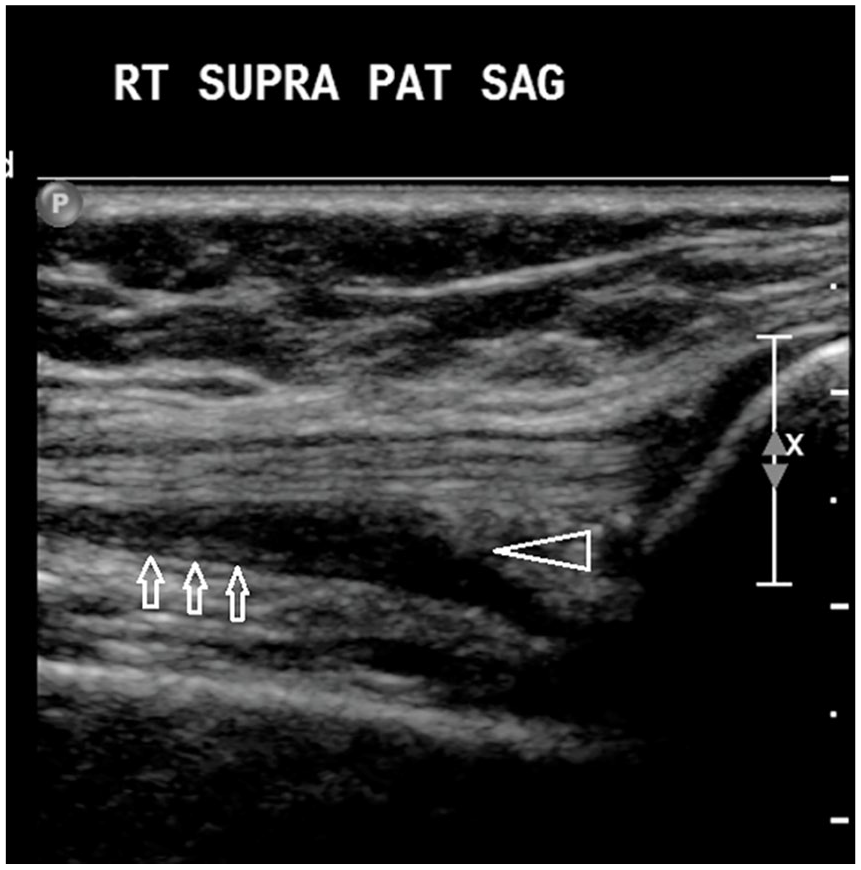
A mild to moderate joint effusion is seen in the suprapatellar recess of the knee, represented by a simple anechoic collection with angular margins (white arrowhead). Also seen outlining the effusion is thickened, hypoechoic synovium (white arrows).
Tenosynovitis
The sheaths of tendons adjacent to the affected joint(s) may also be affected in the setting of JIA, and tendon sheath thickening, inflammation, and fluid within the sheath may be seen. Tenosynovitis is defined as hypoechoic/anechoic thickening of the tendon sheath seen in two perpendicular planes with or without Doppler signal. 19 An example of florid tenosynovitis is shown in Figure 3.
Extensive synovial proliferation and inflammation of the tibialis posterior tendon and sheath in a 12-year-old patient with juvenile idiopathic arthritis with clinical indication of ankle swelling.
Synovial hypertrophy/hyperemia
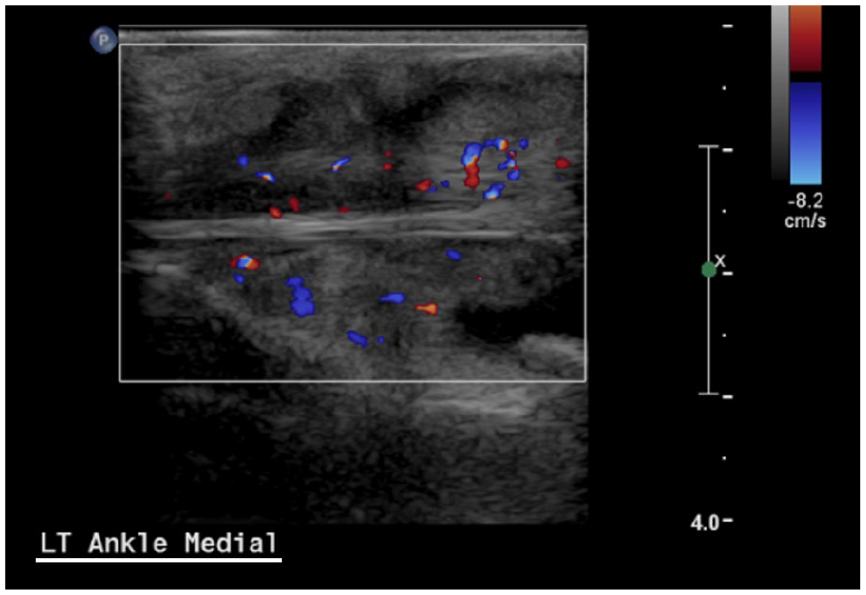
Inflammation of the synovial membrane is pathognomic of JIA and can be directly visualized with sonography as a complex, hypoechoic bulging of the synovium often accompanied by increased vascularity (Figure 4). Operators should keep in mind to reduce the Doppler scale to allow for detection of low-velocity blood flow in the periarticular structures. Increased vascularity of the hypertrophic synovium indicates active disease. 19 Remember that periarticular vascularity on Doppler without structural synovial abnormality on gray-scale sonography should be interpreted with caution, given the limited anatomical knowledge of normal feeding vessels in the pediatric joint. 13
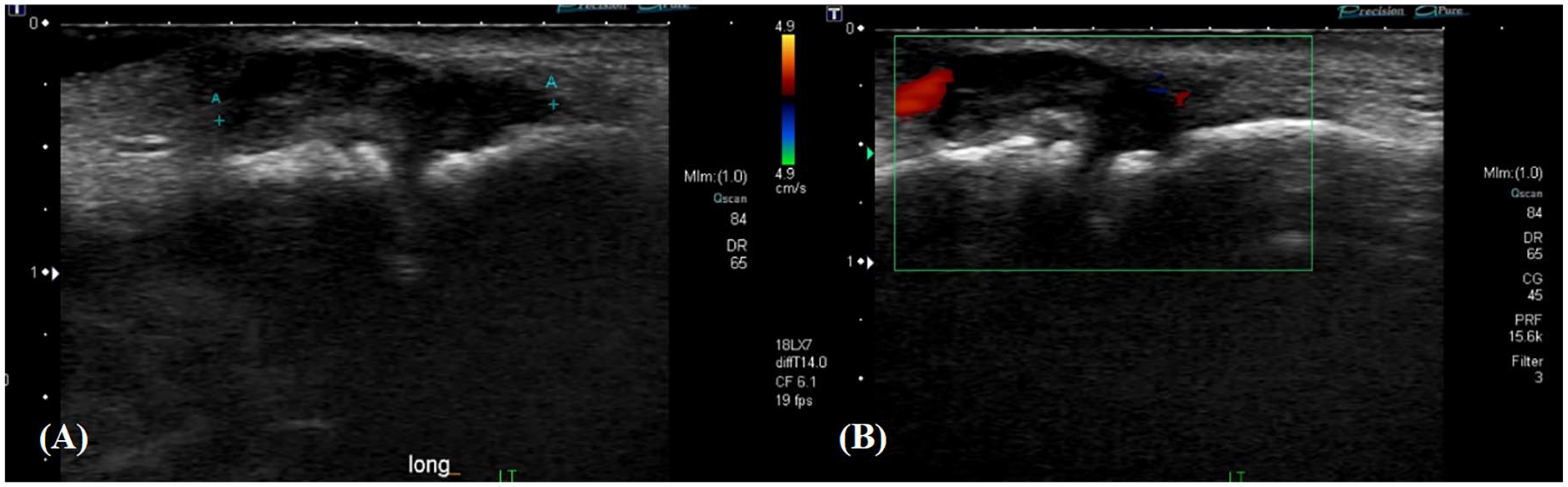
These images of a 12-year-old with juvenile idiopathic arthritis indicate synovial hypertrophy of the second proximal interphalangeal (PIP) joint of the foot both on B-mode (A) and with Doppler (B).
Enthesitis
Enthesitis (inflammation of the tendon-bone junction) represents nearly 20% of JIA categories and is most commonly involved in children at the foot and knee. 12 Sonographic detection of enthesitis in children can be challenging due to the variable sonographic appearances of the growing skeleton. One study assessed reproducibility with ultrasound by defining enthesitis as a power Doppler signal indicating abnormal vascularization of the enthesis insertion into cortical bone. 20 Results were mixed (κ coefficients of 0.35 and 0.5 for concordance of sonography with clinical tenderness and swelling, respectively), which suggest that the clinical and imaging findings of enthesitis in JIA do not always agree. One confounding factor to keep in mind is the difficulty to differentiate normal feeding vessels in children from pathological inflammatory blood flow. 21
Thinning of articular cartilage
Sonographic measurement of articular cartilage thickness in this patient population remains controversial, although in this review, several studies report promising results, especially when used to measure distal femoral cartilage thickness at the intercondylar notch.22–25 Age and body mass indices are thought to be confounding factors in these measurements. An example of articular cartilage thinning over the medial femoral condyle is shown in Figure 5.
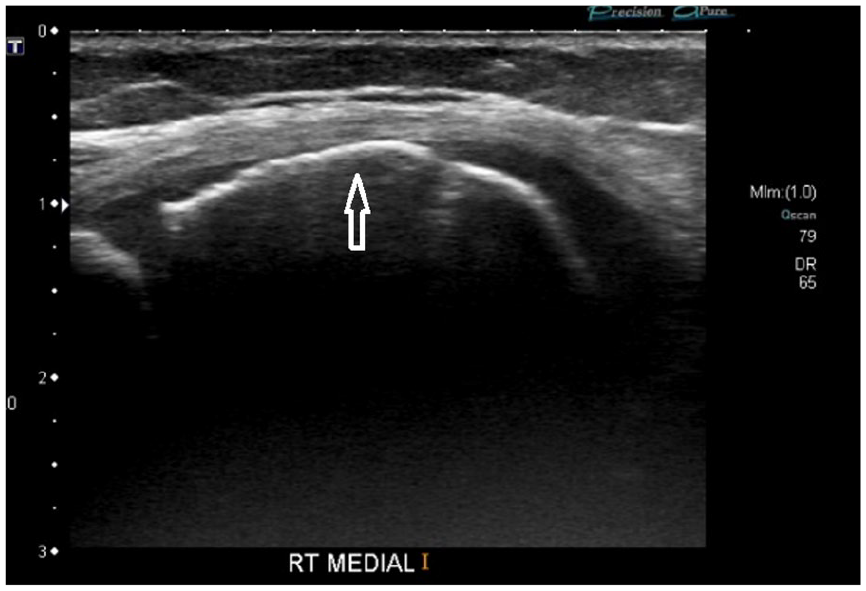
Thinning of the articular cartilage over the medial femoral condyle in a patient with juvenile idiopathic arthritis. There is total lack of visualization of the normal cartilaginous interface (white arrow).
Bony erosions
Erosion of the bony epiphyses (Figure 6) is an indicator of advanced arthropathy and suggests the presence of late-stage degenerative change. In the pediatric population, it is difficult to differentiate the sonographic appearance of ossification centers, which appear irregular, with true erosion, and so other imaging modalities such as MRI or conventional radiography (CR) remain gold standard for detecting epiphyseal erosion. 3
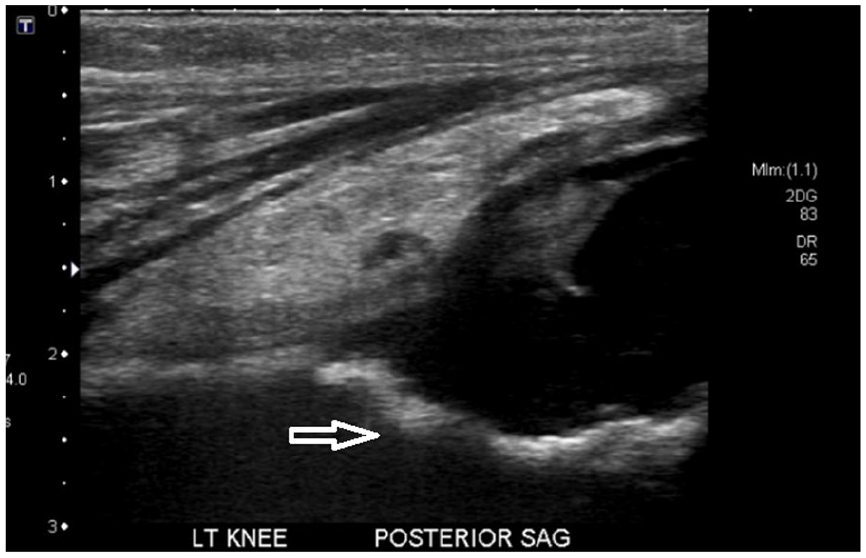
A posterior subperiosteal collection is seen behind the knee in a patient with worsening suprapatellar fluid collection. Deep to the posterior collection, there is evidence of cortical irregularity suggestive of bony erosion (white arrow).
Discussion
Sonography is an inexpensive, nonionizing, noninvasive, and real-time imaging modality to assess joints and other musculoskeletal structures. Children tend to tolerate the examination very well, eliminating the need for sedation. Magni-Manzoni comments on how this type of scanning can even be fun for some children, or they are amenable to taking a nap during the examination. 26 The use of toys, videos, and other distractions, combined with a welcoming environment, can pacify even the most difficult pediatric patient.
Sonography is superior to clinical examination and conventional radiography for detecting early signs of JIA, especially with the application of Doppler. However, the relevance of early findings in the disease is not well established. Further studies specifically assessing the ability of sonographic disease indicators to predict clinical flares of joint pain/swelling would be useful. This will be especially important considering recent technological improvements in the detection of low-velocity blood flow, requiring us to reexamine the true relevance of sonographically detectable microvasculature in the joints of patients with JIA.
Pediatric MSKS remains highly operator dependent, and this issue is further compounded by the fact that the bony and vascular sonographic anatomy of the growing skeleton is not well understood. Novice operators should remember to avoid excess transducer pressure for fear of compressing synovium/vessels and to use contralateral comparison when the presence of disease is not clear. To avoid increasing the rates of false positives for synovitis in patients with JIA, operators should avoid using Dopplers in areas without gray-scale sonographic evidence of synovial hypertrophy, as normal vasculature may be misinterpreted as synovial inflammation.
Sonography is limited in its ability to evaluate structures deep within the joint, and so for the assessment of degenerative joint disease and the quantification of synovial volume, MRI is the preferred modality. 27 To date, no studies have been published applying 3-dimensional ultrasound technologies to the joints of patients with JIA to measure synovial volume.
Further high-quality studies are needed to assess the responsiveness of MSKS as a tool to measure clinically meaningful change in patients with JIA.
Study Limitations
The current study represents a narrative review of the literature as it concerns the role of MSKS in JIA, and as such, a systematic analysis of study data is not included. Here, the authors focus on imaging in JIA as it would relate to the ultrasound operator, and so the diagnosis, classification, and treatment of JIA are outside the scope of the current work. Only one author conducted the screening of articles to be included, which introduces a potential for selection bias, and only English-language articles were considered in the qualitative synthesis, introducing a risk of incomplete retrieval of relevant research.
Conclusion
Although the management of JIA is well described, a definite paucity exists when it comes to its specific sonographic appearances and techniques for scanning. Here, to address this gap in the literature, the authors have presented a narrative review of the current published works on the role of sonography in JIA, supplemented by their own experience and technical knowledge of MSKS. Although highly operator dependent, MSKS is an excellent evaluation tool in the setting of JIA to detect subclinical disease for early intervention or to differentiate between active versus inactive disease. The main imaging findings include joint effusion and synovial hypertrophy/hyperemia. The ability of sonography to monitor the joint’s response to therapy is less well established. The literature also appears conflicted on the ability of sonography to detect bony erosion and measure articular cartilage (as compared to MRI), and further investigation is warranted. Although many studies confirm the validity of sonography to assess synovitis in JIA, its utility as an outcome tool is not well established, as few recent studies have assessed its responsiveness.
Footnotes
Acknowledgements
We thank the Head of Ultrasound Research at the Hospital for Sick Children, Dr. Arun Mohanta, as well as the ultrasound staff for the valuable diagnostic images shared in this literature review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.