
Abstract
Background:
The purpose of this study was to evaluate the diagnostic value of ultrasonography as compared with intra-abdominal pressure (IAP) measured with a urinary catheter.
Methods:
This was a cross-sectional study. The participants consisted of 146 patients hospitalized in the emergency wards of two hospitals in Isfahan (2017-2018). Following measurement of IAP through a urinary catheter, ultrasonographic measurement of the inferior vena cava (IVC) diameter, internal jugular vein diameter, common femoral vein (CFV) diameter, and ratio between the IVC and abdominal aortic diameters was completed. Correlation between these methods of measurements for IAP was investigated.
Results:
There was a significant positive correlation between intrabladder pressure and the right internal jugular vein (RIJV) and CFV (P < .001, R > 0). There was also a reverse significant correlation between intrabladder pressure and RIJV, IVC, IVC:aorta diameter, systolic blood pressure, and tricuspid annular plane systolic excursion (P < .001, r < 0). RIJV, CFV, and tricuspid annular plane systolic excursion were suitable predictors for the estimation of intrabladder pressure or IAP (P < .05), but IVC, IVC:aorta, and systolic blood pressure were not suitable factors for estimating IAP (P > .05).
Conclusion:
Ultrasonographic measurement is a noninvasive method for determining IAP.
Intra-abdominal pressure (IAP) is defined as the steady-state pressure concealed within the abdominal cavity and resulting from the interaction between the abdominal wall and viscera. IAP changes are dependent on the respiratory phase and abdominal wall resistance. 1 In healthy individuals in a supine position, normal IAP ranges from 0 to 6.5 mm Hg.2,3 IAP may reach 15 mm Hg in cases that are not of a serious pathologic condition (e.g., obesity). 1 IAP may temporarily increase for brief periods following some activities, including weight lifting, valsalva maneuver, or coughing. 4 Intra-abdominal hypertension (IAH) is defined as sustained or repeated IAP elevation >12 mm Hg and has a higher mortality rate than that of patients without IAH. 4 IAH is associated with adverse effects on organ function both inside and outside the abdominal cavity, including lungs, heart and arteries, kidney, and the digestive system. Abdominal compartment syndrome refers to IAH >20 mm Hg and is associated with end-organ dysfunction.5,6 Several risk factors are noted for abdominal compartment syndrome, including postoperative complications (bleeding, infusion of carbon dioxide into the abdomen during laparoscopy, etc.) and nonsurgical complications (intra-abdominal tumors, pneumoperitoneum, prone condition, peritoneal dialysis, etc.).5,6
Therefore, measuring IAP to prevent complications caused by high-risk changes in IAP is vital, especially in cases prone to develop elevated IAP caused by the aforementioned risk factors. Various invasive and noninvasive methods have been proposed for taking IAP measurements. IAP can be measured with a direct technique through the peritoneal catheter. Despite precise measurement, it is an invasive technique with potential side effects on the patient.7,8 Invasive techniques have been proposed for IAP measurement, including measuring intrabladder pressure, intragastric pressure, intracolonic pressure, and intrauterine pressure.9,10 Intrabladder pressure measurement is one of the fastest ways for measuring IAP, and approximately 90% of cases of intra-abdominal measurements are taken this way worldwide.9–11 A urinary catheter is inserted into the bladder for intrabladder pressure measurement. 11 Measurement of central venous pressure (CVP) is another technique for recording IAP measurements. Its association with API was highlighted in various studies.11–13 Other noninvasive techniques have been proposed for determining IAP, including ultrasonographic measurements of the inferior vena cava (IVC) diameter, the internal jugular vein (IJV) diameter, the common femoral vein (CFV) diameter, and the ratio between the IVC diameter and the abdominal aortic diameter. Association of these measurable indices with CVP allows for these methods to be used to make an IAP measurement.14–17 Precision of these techniques varies in different situations. For example, measurement of IVC diameter may be difficult or imprecise in cases of complications attributed to heart failure, pericardial fluid, abdominal mass, critically ill patients, or abdominal distension following fluid accumulation in the abdominal cavity. In such cases, other methods can be used, and complementary studies can be carried out to achieve more precise results.17,18
The tricuspid annular plane systolic excursion (TAPSE) method is one of these techniques that is commonly used to determine the right ventricle function in the systolic phase and its association with CVP. 19 Since the various studies comparing these methods of measurement have shown different results, the aim of this study was to evaluate the diagnostic value of ultrasonography at the inpatient’s bedside to compare with the intrabladder method with urine bladder catheterization in the diagnosis of IAP.
Methods
This was a cross-sectional study conducted during an inpatient admission. The participants consisted of 146 patients hospitalized in the emergency wards of two hospitals in Isfahan (2017-2018). The inclusion criteria were that patients had a urine bladder catheter and consented to the study. Exclusion criteria were patients without a urinary catheter and an inability to sleep in a supine position.
The proposal was approved, and a necessary license was obtained from the Ethics Committee of Isfahan University of Medical Sciences. Informed consent forms were obtained from all patients. The patients were selected via a nonprobability sampling. Basic information (age, sex, and history of disease) was collected and recorded in the patient’s record. Standard monitoring was applied to each patient (electrocardiography, systolic and diastolic blood pressure, respiratory rate, and heart rate).
Given that the patients had catheters, the drainage bag was removed, and 60 mL of normal saline was injected into the urinary catheter in a sterile fashion. After 30 to 60 seconds, the venous tube was connected to the catheter and placed vertically at a 90° angle to the pelvis of the patient. The pubic symphysis was considered as a zero point for measurement. The clamp was opened to raise the fluid column within the intravenous set. Maximum fluid height inside the tube was measured. Distribution of IAP was specified by the centimeters of water converted to millimeters of mercury (Table 1).
Intra-abdominal Pressure Grading.
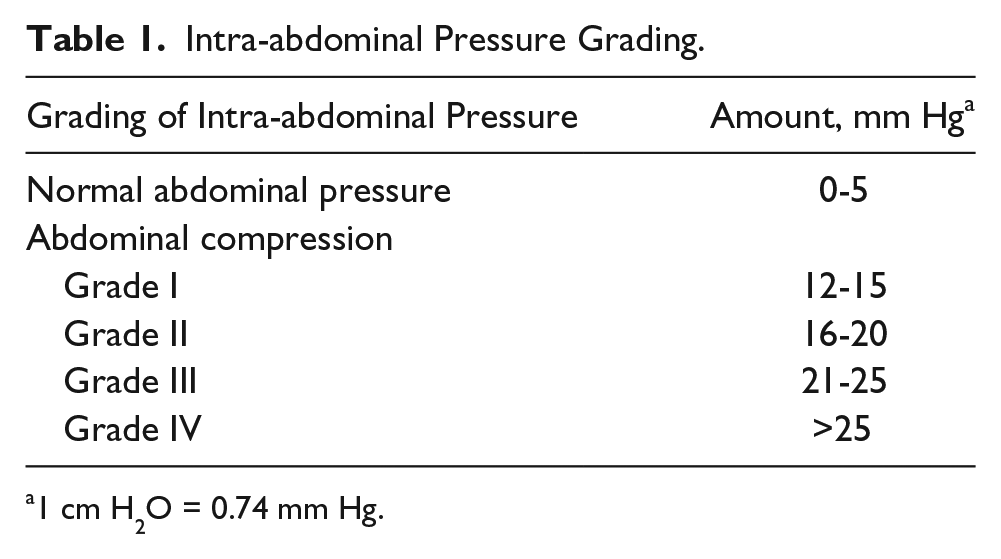
1 cm H2O = 0.74 mm Hg.
Intrabladder pressure was also measured and recorded. If IAP was >20 mm Hg, other symptoms were recorded, such as decreased urine output, decreased blood pressure, respiratory distress, and hypoxia. If two of the listed symptoms were noted and an elevated IAP detected, the patient was definitively diagnosed with abdominal compartment syndrome by the researcher.
Following IAP measurement through the bladder catheter, ultrasonographic measurement of the IVC diameter, the IJV diameter, the CFV diameter, and the ratio between the IVC diameter and the abdominal aortic diameter were completed. An individual trained in ultrasonography made the measurements but was not aware of the IAP measurement results obtained through the bladder catheter.
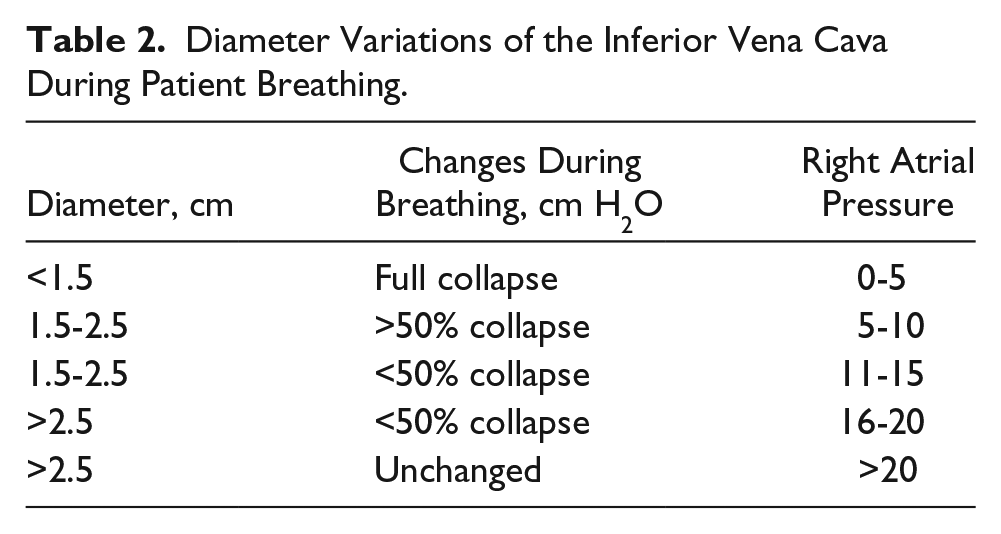
The protocol included all patients sleeping in the supine position with the ultrasound transducer placed below the xiphoid (1.5 cm below the diaphragm) to examine the IVC. The IVC diameter decreases and blood flow increases during normal inhalation. Changes in the ratio between the IVC diameter during inhalation and exhalation was more noticeable in patients with high intra-arterial blood pressure than in normal individuals. M-mode tracing was used to calculate the minimum IVC diameter during respiration (see Table 2). The SonoSite Edge ultrasound system (W/L38xi; FUJIFILM SonoSite) was used portably to conduct the imaging.
Diameter Variations of the Inferior Vena Cava During Patient Breathing.
The high-frequency linear transducer was used to measure the diameter of the CFV while the patient was in the supine position. The femoral vein lies within the femoral triangle in the inguinal-femoral area. The distal border of this area is formed by the inguinal ligament. The CFV, artery, and nerve lie within the triangle from medial to lateral borders.
The CFV was located, and the changing vein diameter and blood flow velocity were recorded with inhalation and exhalation. Femoral vein diameter ≤0.8 cm is a predictor of CVP <10 cm. A CFV diameter >1 cm is a predictor of elevated CVP. A CFV diameter >1.2 cm is a definitive predictor of elevated CVP. A CVP >12 mm Hg is considered elevated CVP.11–13
The transducer was placed at the vertex of the sternocleidomastoid muscle triangle (composed of clavicular and sternal muscles; the heads of the muscle attach to each other near the larynx) to examine the IJV. The IJV diameter was measured with a high-frequency (5-10 MHz) linear probe with respect to respiration.
TAPSE was measured at the apical four-chamber view or subxiphoid view. This is considered to be the best view to observe the size of the right ventricle in contrast to the left ventricle. The normal ratio of the right:left ventricle is 6.10:1. Right ventricular hypertrophy (also called right ventricular enlargement) happens when the right and left ventricles have the same size at the atrioventricular valve. Flattening of the interventricular septum (D-shaped left ventricle) is another finding consistent with elevated right ventricle pressure. Apex-to-base left ventricular shortening is the best and most advanced parameter for assessment of global right ventricular function. TAPSE is defined as the total excursion of the tricuspid annulus from end diastole to end systole, and it is measured typically at the lateral annulus with M-mode. It should be noted that TAPSE >1.6 cm was considered normal function; values between 1 and 1.5 cm, mild-moderate; and values <1 cm, severe dysfunction. A low-frequency curved linear probe was used to measure the ratio of the abdominal aortic diameter to the IVC diameter.
Statistical Analysis
The sample size was 146 based on a study by Malik et al. 20 Collected data were entered into SPSS (v 24; IBM). Quantitative data were reported as mean ± SD and qualitative data as n (%). Diagnostic value tests, Pearson correlation coefficient, and multiple regression were used for data analysis. The significance level was <.05 in all analyses.
Results
In this study, 77 men and 63 women with a mean age of 57.14 ± 15.32 years participated. The mean systolic blood pressure in patients was 115.01 ± 24.54 mm Hg, and the intrabladder pressure was 16.07 ± 7.43 mm Hg. The mean internal diameter of the vein was 1.72 ± 0.33 cm; IVC diameter, 1.91 ± 0.72 cm; CFV diameter, 1.59 ± 0.70 cm; aorta, 2.54 ± 0.67 cm; TAPSE, 1.18 ± 0.38 cm; and IVC:aorta, 0.66 ± 0.31. In 50 (35.7%) patients, the IVC was collapsed; in 77 (55%), it was more or less than 50% collapsed; and in 12 (8.6%), it was unchanged.
In addition, the IAP was normal in 33 (23.6%) cases, grade I in 55 (39.3%), grade II in 21 (15%), grade III in 19 (13.6%), and grade IV in 12 (8.6%). Based on Pearson correlation, there was no significant correlation between age and diameter of the aorta with intrabladder pressure (P = .88). However, there was a significant positive correlation between intrabladder pressure and RIJV and CFV (P < .001, R > 0). There was also an inverse correlation between intrabladder pressure and IVC, IVC:aorta, SBP, and TAPSE (P < .001, r < 0) (Table 3).
Correlation Between Bladder Pressures and Other Measurements.

Abbreviations: CFV, common femoral vein; IVC, inferior vena cava; RIJV, right internal jugular vein; SBP, systolic blood pressure; TAPSE, tricuspid annular plane systolic excursion.
Based on multivariate regression, RIJV, CFV, and TAPSE are prognostic factors for predicting intrabladder pressure or IAP (P < .05), but IVC, IVC:aorta, and SBP are not suitable factors for estimating IAP (P > .05) (Table 4).
Coefficients Based on Variables Within the Study. a
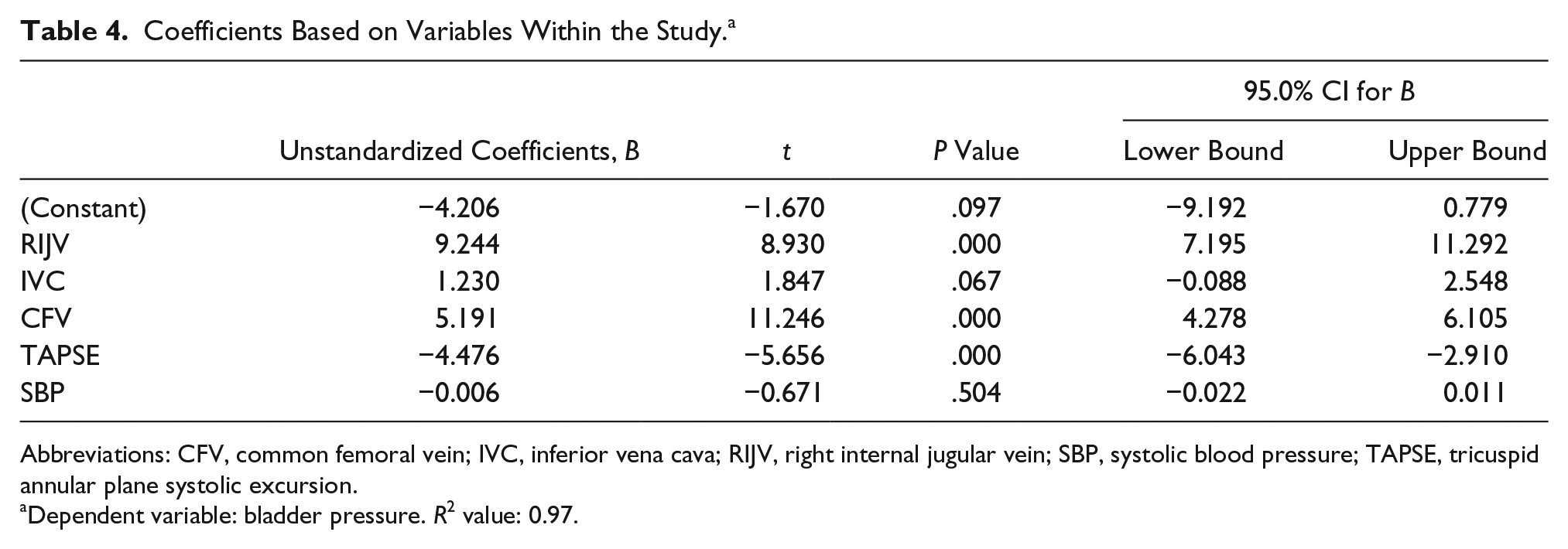
Abbreviations: CFV, common femoral vein; IVC, inferior vena cava; RIJV, right internal jugular vein; SBP, systolic blood pressure; TAPSE, tricuspid annular plane systolic excursion.
Dependent variable: bladder pressure. R2 value: 0.97.
Based on multiple regression, IAP can be measured with RIJV per the following formula:

Also, IAP can be measured with CFV per the following formula:

Finally, based on the analysis of variance test for imported models, these were chosen to determine overall prediction and, specifically, the effect of intrabladder pressure (Table 5).
Analysis of Variance for the Proposed Model. a
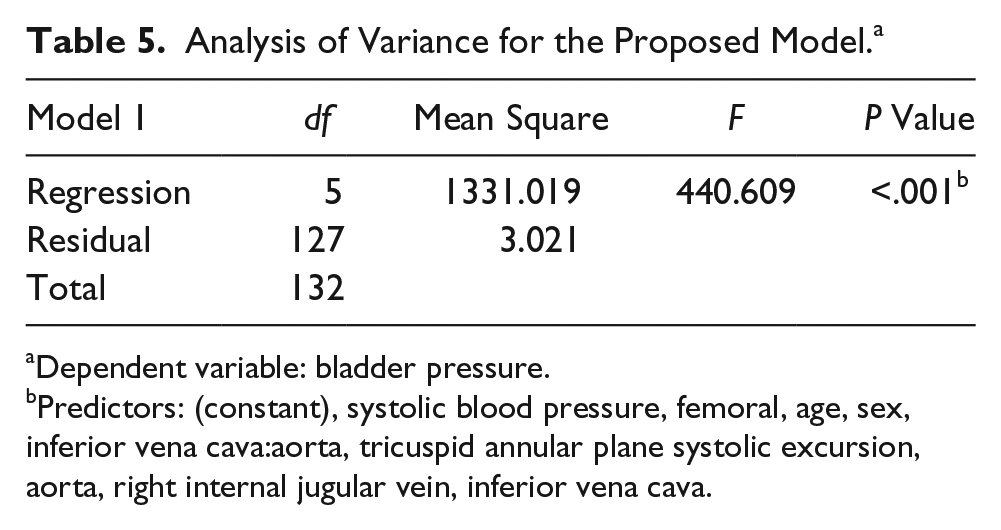
Dependent variable: bladder pressure.
Predictors: (constant), systolic blood pressure, femoral, age, sex, inferior vena cava:aorta, tricuspid annular plane systolic excursion, aorta, right internal jugular vein, inferior vena cava.
Discussion
Based on the results of this study, with increased intrabladder pressure or IAP, as expected, the measurements of the IVC, IVC:aorta, and TAPSE were decreased. Likewise, the measurements of the CFV, RIJV, and aortic diameter were unchanged. In this study, utilizing ultrasonographic measurement parameters was a more appropriate and noninvasive method than using a urine catheter for estimating IAP. Comparatively, regression analysis demonstrated that the RIJV, CFV, and TAPSE were prognostic factors for estimating IAP. However, the use of IVC:aorta and IVC or SBP is not a predictive factor for predicting IAP. Ultrasonography is a noninvasive cost-effective method for estimating IAP and may be a better technique. 21 Bauman et al. demonstrated a correlation between the collapsing of the IVC and IJV and spontaneous breathing; however, there was no correlation between IVC collapsing and positive ventilation pressure. Interestingly, decreasing IVC diameter was associated with increasing IAP. 16 According to their work, there was a significant reverse correlation between IVC and IAP that occurred in both spontaneous breathing and respiration with positive ventilation, which was higher in inhalation alone. In that study, IVC collapse was associated with compartment syndrome or increased IAP. 16
Foley urinary catheter is one of the most widely used methods for measurement of IAP. Fusco et al. demonstrated that injection of 50 mL of normal saline into a Foley catheter delivers more reliable results than injection of a lower volume of fluid. 22 In this study, 60 mL of normal saline was injected into the Foley catheter to obtain results that are more reliable. Ultrasonographic measurement of IAP is more reliable than catheterization. Blaivas showed that ultrasonographic measurement of IAP in patients with compartment syndrome is more advantageous than other methods. 23 A study by Cavaliere et al. indicated that ultrasonographic measurement of the IVC diameter is preferable to measurement of the diameter of other intra-abdominal veins for IAP determination. 24 Decreased diameter or collapsed veins indicated IAP elevation. This result is consistent with the results of this study, which showed that IVC decreases as IAP increases. IVC is more useful than other ultrasonographic markers for IAP assessment. Sixteen healthy individuals were examined in the Cavaliere et al. study in which IAP elevation was simulated with external pressure. The results showed that ultrasonography and IVC examination were the best methods for IAP determination. Sugrue et al. also assessed the efficacy of varied methods for making an IAP measurement but preferred ultrasonographic measurements and emphasized their use. 25 The results of the former studies were consistent with the results of this study. Therefore, sonographic measurement of IAP is superior over other methods.
Conclusion
The results of this study and other studies demonstrated that the ultrasonographic measurement of IAP is a useful and efficient method for IAP measurement. This is noninvasive method devoid of catheterization, which makes it a more tolerable measurement technique for patients. Therefore, it is suggested that ultrasonographic indices of IVC, RIJV, CFV, and TAPSE be used for IAP measurement in patients prone to develop IAP elevation. Limitations of the study were the small sample size, lack of assessment of other effective factors in IAP, and limited studies in this area of research. Therefore, it is highly recommended that similar studies be conducted with larger sample sizes to examine this noninvasive method.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.